Syphilis and hearing loss
ŌĆóDownload as PPTX, PDFŌĆó
2 likesŌĆó195 views

This document discusses the origins, stages, transmission, diagnosis, and treatment of syphilis. It notes that syphilis was first observed following European contact with the Americas in 1494. Syphilis can cause significant pregnancy and birth complications, and in 1990 it caused over 200,000 deaths worldwide. The document outlines the four stages of syphilis infection - primary, secondary, latent, and tertiary - and describes their associated symptoms. Diagnosis involves clinical exams and tests like dark-field microscopy and serology. Treatment is with benzathine penicillin injections. The document concludes with a case study of a child presenting with late congenital syphilis and Hutchinson's triad of symptoms.







Syphilis and hearing loss
- 1. By: A.A.ADENIJI FAM MED REGISTRAR . ENT ROTATTION Tygerberg Academic Hospital 23/07/2015
- 2. .Origin of syphilis *Pre columbus and columbus hypothesis *First out break..1494/1945 *Obstetric sequelea ..700,000 to 1.6million pregnancy affected yearly. *20% perinatal dealth in subsharan African annually. *202,000 mortality in 1990 *1999 syphilis surge..12million, 90% in developing countries.
- 3. *202,000 mortality in 1990 *1999 syphilis surge..12million, 90% in developing countries. *113,000 mortality in 2010 *prevalence are proportionally high among iv drug users, HIV patients and msm. *1990 : increased rate among heterosexuals in china and Russia *syphilis increase risk of HIV by 2 to 5 times.
- 4. ’üĮ *Spirocheate infections: ’üĮ -T pallidium ’üĮ ..sub species: ’üĮ .pertenueŌĆ”.yaws ’üĮ .careteumŌĆ”Pinta ’üĮ .Endemicum..Bejel ’üĮ Only pallidium causes neurological diseases.
- 5. ’üĮ Primary transmission: sexual contact. ’üĮ Vertical transmission..in utero ’üĮ Compromised mucosa ’üĮ Blood products. ’üĮ Needle sharing
- 6. ’üĮ 4 stages ’üĮ *Primary ’üĮ *Secondary ’üĮ *Latent ’üĮ *Tertiary
- 8. ’üĮ Direct contact with infected lesion. ’üĮ Chancre within 3 to 90 days ’üĮ Chancre:often single, painless ulceration with clean border and sharp base. ’üĮ Extragenital:2%-7%, cervical:44%, penile in heterosexual:99%,Anal/recta in MSM:34%, LN :80%
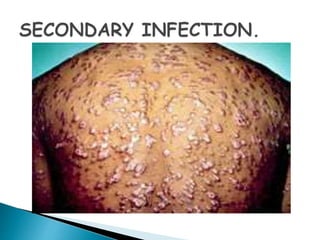
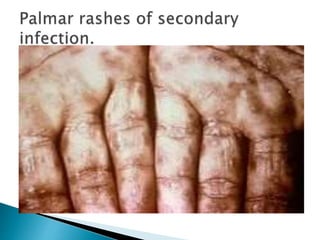
- 11. ’üĮ 4 to 10 wks after primary infection ’üĮ Variation of presentation involving:skin, mucous membrane, maculopapular rashes in the palm, trunk, soles or extremeties ’üĮ Fever, sorethroath, malaise, weight loss, hair loss, headcahes, ’üĮ Rarely:intestitial keratitis, uveaitis, optic neuritis and hepatitis. ’üĮ Most patients do not have previous primary infection. 25% may have recurrence.
- 12. ’üĮ Serologic proof of infection with no symptoms. ’üĮ Early L: Less than a year after primary infection ’üĮ Late L: Over a year after primary infection. ’üĮ Late LS are often asymptomatic.
- 13. ’üĮ 3 TO 15 years after primary infection ’üĮ -Gummatous syphilis(15%) ’üĮ -Late neurosyphilis(6.5%) ’üĮ -Cardiovascular syphilis(10%) ’üĮ This is a non infective syphilis
- 14. *Clinical suspicion and investigation. *Direct and indirect investigations. *DIRECT: Dark ground microscopy,Direct fluoresent antibody test and Nucleic acid amplification test *INDIRECT: Non treponema(VDRL and RPR). *Treponema Test:TPHA and FTA_Abs *Trepona usually becomes positive 2-5 wks after initial infection.
- 15. Primary preventionŌĆÖ ’üĮ Secondary prevention. ’üĮ RPR titre>1.4 ’üĮ Benzathine penicillin 2.4 million units wkly for 3 wks. ’üĮ If mother has received less than 3 doses child to be treated for congenital syphilis ’üĮ 28 days course of erythromycin or doxycyline in penicillin allergic patients. Symptomatic baby: procaine pen 50000 u dly for 10 days.
- 16. ’üĮ ASE PRESENTATION A 7-year-old female presented with her mother to the clinic with the complaints of poor dental esthetics. The patient was diagnosed with late congenital syphilis (2 years after ’üĮ birth). She was non-reactive for HIV. The patient was on regimen of penicillin treatment from late congenital syphi- lis and corticoid therapy. HutchinsonŌĆÖs triad was detected by the presence of interstitial keratitis (’¼ü gure 1 ), with cor- neal scarring and initial presentation of bilateral blindness; deafness from auditory nerve disease and dental defects ( ’¼ü gures 2 and 3 ). Restorations in posterior teeth were observed and it is not possible to af’¼ü rm the presence of mulberry molars ( ’¼ü gure 4) . The patientŌĆÖs mother reported precocious loss of deciduous teeth because of dental caries.
- 17. ’üĮ Congenital syphilis sometimes is undiagnosed and often inadequately treated. 14 It is also associated with poor socio-economic conditions with a low educational level, 2 as demonstrated in the case report presented, with the sev- eral complications of disease. Most of the clinical signs of congenital syphilis were developed later, 4 2 years after birth. All the characteristics of HutchinsonŌĆÖs triad were identi’¼ü ed. 4 ŌĆō 7 Interstitial kerati- tis was diagnosed when she was 6-year-old, 10 with a bad prognosis. Although eighth nerve deafness often starts when the child is between 8 and 10 years of age, 11 the patient had hearing loss when she was 6-years-old. In the case reported, dental defects were observed only on anterior teeth. This ’¼ü nding is associated of degenerative changes in the enamel epithelium induced by T pallidum , leading to the complete destruction of the ameloblasts dur- ing odontogenesis.
- 18. ’üĮ As a result, formation of abortive enamel and also cessation of enamel production occurred. 5 7 It was not possible to af’¼ü rm the presence of mulberry molars because of dental restorations. Premature loss of primary teeth associated with congen- ital syphilis has been reported. 8 However; it is not possible to af’¼ü rm if this occurrence in the patient was associated with congenital syphilis or premature loss of deciduous teeth because of caries reported. ’üĮ Congenital syphilis is an eminently preventable disease. In order to reduce the likelihood of its occurrence, a repeat test towards the end of gestation or at the time of delivery should be done for women in high-risk groups. 1
- 19. ’üĮ Congenital syphilis re’¼é ects a failure of prenatal care systems and syphilis control programs as found in this case reported. *Detection and appropriate timely penicillin treatment is a highly effective intervention to reduce this infection disease, avoiding signi’¼ü cant morbidity in the future. ’üĮ HutchinsonŌĆÖs triad usually becomes apparent after 5-years of age.
- 20. ’üĮ BLIND RATS ARE WISE. ’üĮ DEAF RATS ARE STURBBORN. ’üĮ RATHER BE BLIND THAN BEING DEAF. ’üĮ TAKE CARE OF YOUR EAR.