




























toxoplasma.pptx
- 2. ï HISTORY ï MORPHOLOGY ï LIFECYCLE ï TRANSMISSION ï PATHOPHYSIOLOGY ï CLINICAL MANIFESTATIONS ï DIAGNOSIS ï TREATMENT ï PREVENTION
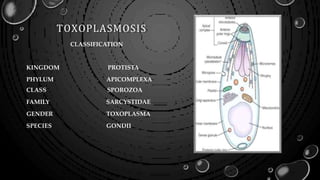
- 3. SIR HENRY NICOLLE ïą TOXOPLASMOSIS GONDII DISCOVERED AND NAMED BY CHARLES JULES HENRY NICOLLE (1866-1936) AND MONCEAUX IN 1908. ïą AN INTRACELLULAR PARASITE WAS ISOLATED FROM THE LIVER AND SPLEEN OF A WILD AFRICAN RODENT CTENODACTYLUS GONDII. ïą A YEAR LATER THEY CALLED IT TOXOPLASMA GONDII BECAUSE OF ITS ARCHED SHAPE (TOXON: ARCH) AND BECAUSE OF THE COMMON NAME IN WHICH IT WAS FOUND, THE GONDII.
- 5. 1908 1923 Janku Chorioretinitis 1939 Wolff and Col Congenital meningoencephalitis 1948 Sabin and Feldman Reaction Serological 1949 Frenkel Hypersensitivity test 1970 renkel & hutchison True Form of Transmission
- 6. MORPHOLOGY âĒ ASEXUAL FORMS TACHYZOITE BRADYZOITE (TISSUE CYST) âĒ SEXUAL FORM OOCYST
- 7. TACHYZOITES ïą ACTIVELY M U LT I P LY I N G F O R M CRESCENT SHAPE SEEN IN ACUTE INFECTION ïą INFECT ALL THE NUCLEATED M A M M A L I A N CELLS ïą INSIDE THE HOST CELL, THE TACHYZOITES ARE S U R RO U N DE D BY A VACUOLE - ASEXUAL M U LT I P L I C AT I O N OCCURS - ROSETTES
- 8. BRADYZOITES ïą RESTING STAGE OF THE PARASITE ïą SEEN IN C H RO N I C INFECTIONS MOST C O M M O N SITE IS MUSCLES A N D BRAIN ïą INSIDE THE CYST - SLOWLY M U LT I P LY I N G TROPHOZOITES ARE CALLED AS BRADYZOITES
- 9. OOCYST SEXUAL F O R M OF THE PARASITE F O U N D O N LY IN CATS A N D FELINES
- 10. LIFE CYCLE
- 11. TRANSMISSION ïą INGESTION OF SPO RU LA TED O O C YSTS FRO M C O N TA M IN A TED SOIL, F O O D OR WATER ïą INGESTION OF TISSUE CYST C O N TA I N I N G BRADYZOITES F RO M U N D E RC O O K E D MEAT ïą BY BL O O D TRA N SFU SIO N , N EED LE STIC K IN JU RIES, O RG A N TRANSPL ANTATION ïą TRANSPLACENTRAL TRANSMISSION ïąLABORATORY ACCIDENTS ( TACHYZOITES IN BLOOD)
- 12. The Tachyzoites arereproduced Dissemination Following route lymphatic/ hematogenous Penetrates the intestinal wall PATHOPHYSIOLOGY
- 13. PATHOGENESIS âĒ FORMATION OF TACHYZOITES âMULTIPLY AND DISSEMINATION âĒ LYMPHATIC TISSUE-FOLLICULAR HYPERPLASIA âĒ SKELETAL MUSCLE âĒ MYOCARDIUM-FOCAL NECROSIS (MUSCLE CYSTS) âĒ RETINA ,CHOROID-GRANULOMATOUS LESION âĒ LUNGS-INTERSTITIAL PNEUMONIA âĒ CNS â NECROSIS AND MICROGLIAL NODULES âĒ OTHER ORGANS-PANCREATITIS,GLOMERULONEPHRITIS
- 14. âĒ IN IMMUNOCOMPETENT INDIVIDUALS,IMMUNE MECHANISMS LIKE MACROPHAGES,CD8+ CELLS,NK CELLS,INTERFERON GAMMA,IL-2,12 âĒ KILL OR INHIBIT THE REPLICATION âĒ IMMUNOGLOBULINS A,M,G DEVELOP âĒ TISSUE CYSTS BECOME ACTIVE WITHIN 7 DAYS AND REACTIVATION OCCURS
- 15. ACUTE OR CHRONIC âĒ THE RAPIDLY MULTIPLYING CRESCENTRIC CELL (TACHYZOITES ) INITIATE THE ACUTE STAGE OF DISEASE âĒIN FUTHER DEVELOPMENT THEY PENETRATE NEW CELLS ESPECIALLY EYE AND BRAIN. âĒFURTHER DEVELOPMENT SLOWS DOWN IN THESE ORGANS CALLED AS BRADYZOITES TO FORM A QUIESCENT TISSUE CYSTS âĒ THE EVENT LEAD TO CHRONIC STAGE OF DISEASE
- 16. CLINICAL MANIFESTATIONS ïą FEATURES IN I M M U N O C O M P E T E N T INDIVIDUAL ïą FEATURES IN IMMUNODEFICIENT INDIVIDUAL ïą CO N G E N I TA L TOXOPLASMOSIS ïą OCULAR TOXOPLASMOSIS
- 17. IMMUNOCOMPETENT ïą ACUTE STAGE-ASYMPTOMATIC ïą SYMPTOMATIC ï§ HEADACHE,FATIGUE ï§ MALAISE ï§ FEVER ï§ CERVICAL LYMPHADENOPATHY âĒ SUBOCCIPITAL,SUPRACLAVICULAR,INGUIN AL,MEDIASTINAL(DISCRETE,MULTIPLE,VARI ABLE IN CONSISTENCY)
- 18. IMMUNOCOMPROMISED âĒ ACUTE INFECTION OR REACTIVATION OF BRADYZOITES âĒ DEADLIEST-TOXOPLASMIC ENCEPHALITIS âĒ EITHER FOCAL DYSFUNCTION TO NON FOCAL MENINGOENCEPHALITIS âĒ DUE TO VASCULITIS,EDEMA AND HEMORRHAGE âĒ ALTERED MENTATION(75%),SEIZURES(33%), FOCAL NEUROLOGICAL SIGNS(60%), HEADACHE(56%), FEVER(50%) âĒ BRAINSTEM-CRANIAL NERVE PALSY,DYSMETRIA,ATAXIA âĒ BASAL GANGLIA-HYDROCEPHALUS,CHOREIFORM MOVEMENTS, CHOREOATHETOSIS âĒ DD-CRYPTOCOCCAL MENINGITIS,HSE,TM,CNS LYMPHOMA âĒ LUNG-ARDS,HEMOPTYSIS,DIC
- 19. OCULAR TOXOPLASMOSIS ïą BLURRED VISION,SCOTOMA,PHOTOPHOBIA ïą MACULAR INVOLVEMENT-LOSS OF CENTRAL VISION, NYSTAGMUS SECONDARY TO POOR FIXATION ïą EOM- CONVERGENCE-STRABISMUS ïą FLARE UPS OF CHORIORETINITIS-DESTROY RETINAL TISSUEâGLAUCOMA ïą CONGENITAL LESIONS-MASSIVE CHORIORETINAL DEGENERATION WITH EXTENSIVE FIBROSIS ïą IN PATIENTS WITH AIDS,DIFFUSE RETINAL NECROSIS- FREE TACHYZOITES+CYSTS CONTAINING BRADYZOITES
- 21. ïą OCCURS DURING FIRST TIME IN PREGNANCY ïą INFECTION OF PLACENTA-HEMATOGENOUS INFECTION OF FETUS ïą AS GESTATION INCREASES-RATE OF TRANSMISSION INCREASES BUT SEVERITY DECREASES ïą INFECTED CHILDREN INITIALLY ASYMPTOMATIC,PERSISTENCE OF T.GONDII- REACTIVATION-MOST FREQUENTLY CHORIORETINITIS ïą CHORIORETINITIS,STRABISMUS,BLINDNESS,EPILEPSY,ANEMIA,JAUNDICE,RASH ïą MICROCEPHALY,INTRACRANIAL CALCIFICATION,HYDROCEPHALUS,PNEUMONITIS TRIMESTER FIRST SECOND THIRD Trasmission rate 10-25% 30-54% 60-65%
- 22. DIAGNOSIS ïą DIRECT MICROSCOPY ïą DETECTION OF TACHYZOITES IN B LO O D A N D TISSUE CYST IN TISSUE BIOPSY ïą STAINING METHODS: o GIEMSA o PAS o SILVER STAINS o IMMUNOPEROXIDASE STAIN
- 23. SEROLOGY ïą DETECTION OF TOXOPL ASMA ANTIGEN BY ELISA ïą DETECTION OF TOXOPL ASMA ANTIBODY BY o SABIN F E L D M A N DYE TEST o INDIRECT FLUORESCENT ANTIBODY TEST o IGM ELISA o IGG ELISA o IGG AVIDITY TEST
- 24. âĒ PARALLEL IGG TESTING -4 FOLD RISE IN PAIRED SERA OF 3 WEEKS APART- ACUTE INFECTION âĒ IGG âLOW AVIDITY-ACUTE INFECTION(<3 MONTHS) âĒ HIGH -CHRONIC INFECTION(>3 MONTHS) âĒ PRESENCE OF IGA,M,E âACUTE INFECTION âĒ OTHER METHODS-DOUBLE SANDWICH IGM ELISA & IGM IMMUNOSORBENT ASSAY
- 25. MOLECULAR METHODS ïąPOLYMERASE CHAIN REACTION ïąAMPLIFICATION OF B1 GENE DETECTION OF T.GONDII DNA ïąSAMPLES o AMNIOTIC FLUID o PERIPHERAL BLOOD o CSF o URINE o AQUEOUS & VITREOUS FLUID
- 26. TREATMENT âĒ GOAL-TO ARREST THE REPLICATION OF PARASITE AND PREVENT FURTHER DAMAGE TO ORGANS INVOLVED âĒ IMMUNOCOMPETENT âĒ IMMUNOCOMPROMISED âĒ CONGENITAL
- 27. IMMUNOCOMPETENT âĒ NOT REQUIRE SPECIFIC THERAPY âĒ IF OCULAR+ ,TREATED FOR 1 MONTH â PYRIMETHAMINE+SULFADIAZINE/CLINDAMYCIN OR PREDNISONE
- 28. IMMUNOCOMPROMISED âĒ AIDS PATIENTS SEROPOSITIVE FOR T.GONDII âCD4+T LYMPHOCYTE COUNT<100/MCGL(SCREENING AIDS PATIENTS) âĒ IF CD4+T LYMPHOCYTE COUNT>200,NO NEED OF PROPHYLAXIS âĒ TRIMETHOPRIM-SULFAMETHOXAZOLE âĒ NOT TOLERATE-DAPSONE+PYRIMETHAMINE âĒ ATOVAQUONE +/_ PYRIMETHAMINE âĒ PROPHYLACTIC MONOTHERAPY- DAPSONE,PYRIMETHAMINE,AZITHROMYCIN,CLARITHROMYCIN,AEROSOLIZE D PENTAMIDINE âĒ PATIENT+HIV- CD4+T LYMPHOCYTE COUNT>200 FOR ATLEAST 6 MONTHS AFTER ART+ASYMPTOMATIC---DISCONTINUE THE PROPHYLAXIS
- 29. CONGENITAL INFECTION âĒ NEONATES-ORAL PYRIMETHAMINE(1MG/KG) âĒ SULFADIAZINE (100 MG/KG) âĒ FOLINIC ACID FOR 1 YEAR âĒ PREDNISOLONE(1MG/KG PER DAY)-MAY BE USED âĒ PREGNANT-SPIRAMYCIN(IN ACUTE CASE EARLY IN PREGNANCY) âĒ PYRI/SULFA/FOLINIC ACID âAFTER 18 WEEKS OF PREGNANCY
- 30. PREVENTION IS BETTER THAN CURE âĒ AVOIDANCE OF HUMAN CONTACT WITH CAT FECES IS HIGHLY IMPORTANT âĒ CHANGING OF CAT LITTER AND SAFE DISPOSAL CAN PREVENT TRANSMISSION âĒMEAT SHOULD BE COOKED TO INTERNAL TEMPERATURE OF 74-75DEGREE CELCIUS âĒ WASH YOUR HANDS AFTER HANDLING RAW MEAT âĒ PROTECT CHILDREN'S PLAY AREAS FROM CAT AND DOG DROPPINGS âĒWASH YOUR HANDS VERY WELL AFTER BEIN G IN CONTACT WITH SOIL POSSIBLY CONTAMINATED BY ANIMAL FECES âĒ SCREENING OF IMMUNOCOMPROMISED FOR ANTIBODY TO T.GONDII âĒ PREGNANT WOMEN SHOULD AVOID CONTACT WITH KITTENS
- 31. REFERENCES âĒ PRINCIPLES AND PRACTICES OF INFECTIOUS DISEASES,8TH EDITION- MANDELL,DOUGLAS