













Trauma from occlusion
- 1. B Y : D R . R . S E S H A N R A K K E S H
- 2. OUTLINE 1. Definition of TFO. 2. Physiologic adaptive capacity of the periodontium to occlusal forces. 3. Factors that help increase traumatic forces. 4. Classification of TFO. 5. Clinical features of TFO. 6. Radiographic findings of TFO. 7. Treatment of TFO.
- 3. DEFINITION Ą° a condition where injury results to the supporting structures of the teeth by the act of bringing the jaws into a closed position .Ąą(Stillman -1917) Ą° damage in the periodontium caused by stress on the teeth produced directly or indirectly by teeth of the opposing jaw.Ąą (WHO in 1978)
- 4. PHYSIOLOGIC ADAPTIVE CAPACITY OF THE PERIODONTIUM TO OCCLUSAL FORCES ? The periodontium attempts to accommodate the forces exerted on the crown. ? This adaptive capacity varies in different persons and in the same person at different times. ? When occlusal forces exceeds the adaptive and reparative capacity of the periodontal tissues, tissue injury results (trauma from occlusion)
- 5. FACTORS THAT HELP INCREASE TRAUMATIC FORCES: (MAGNITUDE, DIRECTION & DURATION) A) When MAGNITUDE of occlusal forces is increased: 1. The periodontium responds with a widening of the periodontal ligament space. 2. An increase in the number and width of periodontal ligament fibers. 3. Increase in the density of alveolar bone.
- 6. B) Direction of the occlusal forces. ? The periodontal ligament fibers are arranged so that the occlusal forces are applied along the long axis of the tooth. ? Change in the direction of the occlusal forces lead to change the orientation of periodontal ligament fibers.
- 7. C) Duration and frequency of occlusal forces. ? Constant pressure on the bone is more injurious than intermittent forces. ? The more frequent the application of an intermittent force, the more injurious the force to the periodontium.
- 8. CLASSIFICATION ? Based on the duration: ?Acute ?Chronic ? Based on the causative factors: ?Primary ?Secondary ?Combined
- 9. ACUTE TRAUMA FROM OCCLUSION ? Results from an abrupt occlusal impact, such as that produced by biting on a hard object (e.g., an olive pit). In addition, restorations or prosthetic appliances that interfere with the direction of occlusal forces on the teeth may induce acute trauma.
- 10. Clinical features : ? Tooth pain. ? Sensitivity to percussion. ? Tooth mobility.
- 11. CHRONIC TRAUMA FROM OCCLUSION ? It is more common than the acute form and is of greater clinical significance. ? It most often develops from gradual changes in occlusion produced by ? Tooth wear, ? Drifting movement, and ? Extrusion of teeth, combined with parafunctional habits such as bruxism and clenching,
- 12. Primary trauma from occlusion ? A tissue reaction, which is elicited around a tooth with normal height of the periodontium (no attachment loss!) ? It can caused by high filling. faulty restorations or fixed and removable prosthesis, causing large force on the abutment or opposing teeth.
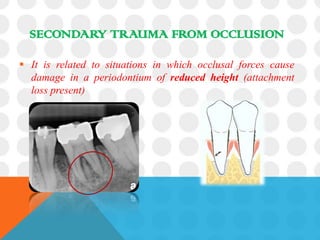
- 13. SECONDARY TRAUMA FROM OCCLUSION ? It is related to situations in which occlusal forces cause damage in a periodontium of reduced height (attachment loss present)
- 14. COMBINED TRAUMA FROM OCCLUSION ?It is the injury that occurs to the periodontium resulting from abnormal occlusal forces that are applied to a tooth or teeth with abnormal periodontal support.
- 15. CLINICAL FEATURES OF TFO 1) Mobility (progressive) 2) Pain on chewing or percussion 3) Fremitus 4) Occlusal prematurities/discrepancies 5) Wear facets in the presence of other clinical indicators 6) Tooth migration 7) Chipped or fractured tooth (teeth) 8) Thermal sensitivity
- 16. RADIOGRAPHIC FINDINGS OF TFO ? Increased width of periodontal ligament space. ? Thickening of lamina dura. ? Vertical or angular bone loss. ? Radiolucency in furcation areas. ? Funnel lshapped bone loss.
- 17. TREATMENT A goal of periodontal therapy in the treatment of occlusal traumatism should be to maintain the periodontium in comfort and function.
- 18. In order to achieve this goal a number of treatment considerations must be considered including one or more of the following : 1. Occlusal adjustment 2. Management of parafunctional habits 3. Temporary, provisional or long-term stabilization of mobile teeth with removable or fixed appliances 4. Orthodontic tooth movement 5. Occlusal reconstruction 6. Extraction of selected teeth