


















































![imaging of scrotum [Repaired] [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/imagingofscrotumrepairedrepaired-230522050410-51cee1e6-thumbnail.jpg?width=560&fit=bounds)




















More Related Content
Similar to TUMOURS OF parotid gland and salivary glands.pptx (20)
More from HamSayshi1 (20)


















Recently uploaded (20)




















TUMOURS OF parotid gland and salivary glands.pptx
- 1. TUMOURS OF PAROTID GLAND DR. HAMZA AHMAD RESIDENT SURGEON UNIT-1
- 2. History: 1.Patient Information: Name: Muhammad Iqbal Masih Age: 55 year Gender: Male Marital status: Married Religion: Christian Known Hypertensive and X-ray operator by profession comes to the Out-patient department with following complaints: ŌĆó Painful swelling in the left cheek-----6 months
- 3. History: 2.History of presenting illness: Mr. Iqbal was in his usual state of health 6 months back when he first noticed a swelling in left parotid region initially about the size of pea & gradually increase in size to a size of lemon. The swelling is painful. The pain is intermittent, dull in character worsened by eating, and occasionally radiates to the left ear. He denies any history of fever, weight loss, or facial weakness. He has no history of dry mouth, altered taste sensations & dysphonia. He has no other similar swelling elsewhere in the body. 3.Past Medical History: Hypertension (controlled with medication), No history of diabetes or other significant medical conditions. 4.Past Surgical History: He had history of cholecystectomy few years back. 5.Personal History: Smoker & Occasional alcohol consumption. 6.Family History: No family history of head & neck cancer, salivary gland tumors or other malignancies.
- 4. Clinical Examination: General Examination: Patient of average build physique & height is conscious, cooperative, and well-oriented to time, place, and person. Vital signs are within normal limits. No signs of pallor and cyanosis and clubbing etc. Rest of general physical examination is unremarkable. Head and Neck Examination: A firm, non-tender, mobile swelling is palpable in the left parotid region just below the left ear lobule, swelling is rubbery in consistency with negative translumination.The overlying skin appears normal and have mild erythema. There is no local rise of temperature. The swelling measures approximately 2x2 cm in size. Intraoral Examination: No abnormalities detected. Neck Examination: No cervical lymphadenopathy detected. Nerve Examination: Facial and trigeminal nerve examination unremarkable.
- 5. Differential diagnosis: Ō¢¬ Parotid gland tumors 1. WarthinŌĆÖs Tumor 2. Pleomorphic adenoma Ō¢¬ Metastasis tumor from skin, oral cavity etc. Ō¢¬ Lipoma
- 7. Ultrasound of swelling: ŌĆó Ultrasound shows a well-defined homogeneous hypoechoic lesion 2x2 cm in superficial lobe of left parotid gland. ŌĆó The lesion shows multiple cystic spaces with internal septations. ŌĆó No evidence of invasion into adjacent structures ŌĆó There is no intralesional flow signal. ŌĆó The rest of the gland shows normal echo pattern without dilated ducts and stone. ŌĆó The right submandibular gland and superficial lobes of both parotid glands show normal echo pattern, size without focal lesion/ dilated ducts. ŌĆó The thyroid gland shows normal echo pattern without focal lesion. ŌĆó There is no cervical lymphadenopathy.
- 8. CT-SCAN: Ō¢¬ Axial scans shows the presence of an ovoid-shape, well-defined, homogeneous lesion of 2x2cm, with rapid enhancement located in the left parotid gland. Ō¢¬ No invasion of the surrounding structures was noted. Ō¢¬ No displacement of the surrounding structured noted. Ō¢¬ Rest of the scan appears normal.
- 9. Fine needle aspiration Cytology (FNAC): ŌĆóAspirate reveals abundant lymphoid tissue with oncocytic cells. ŌĆóCytology is consistent with a Warthin tumor (papillary cystadenoma lymphomatosum).
- 10. WarthinŌĆÖs Tumor of parotid gland Definitive Diagnosis
- 11. Introduction: Tumors of the salivary glands are: ŌĆó Most heterogeneous group of tumors. ŌĆó Greatest diversity of morphologic features. ŌĆó uncommon. ŌĆó The majority of these neoplasms are benign 80% Ō¢¬ and only 20% are malignant. ŌĆó The various types of salivary gland tumors are best distinguished by their histologic patterns.
- 12. Anatomy: Ō¢¬ 3 major salivary glands: 1. The parotid glands 2. The submandibular glands 3. The sublingual glands Ō¢¬ Other locations: lateral margin of tongue, palate, lips, buccal mucosa.
- 13. Parotid gland: ŌĆó The parotid gland - largest of the three major glands and weighs on average between 14 and 30 g. ŌĆó Composed almost entirely of serous cells. ŌĆó Sebaceous glands may be observed in 10% to 42% of normal parotid glands . ŌĆó The parotid glands contain 3 to 32(average: 20) intraglandular lymph nodes. ŌĆó Largest salivary gland & roughly wedge shaped. ŌĆó Lies b/w Sternomastoid and mandible below the External auditory meatus. ŌĆó Coverings : ŌĆó True capsule ŌĆó False capsule ŌĆō a layer from the deep cervical fascia. Ō¢¬ Parotid glands duct also called as StensonŌĆÖs duct Ō¢¬ It emerges from the anterior border of the gland, superficial to the masseter muscle, then it pierces the buccinator muscle & opens into the oral cavity on the inner surface of the cheek, usually opposite to the maxillary second molar.
- 14. Lobes of Parotid gland: ŌĆó Parotid divided into: 1. Superficial-------80% 2. Deep lobes-------20% by the facial nerve. ŌĆó Fasciovenous plane of Patey.
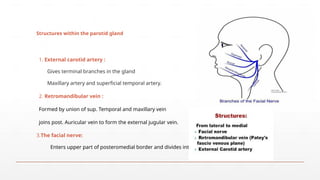
- 16. Structures within the parotid gland 1. External carotid artery : Gives terminal branches in the gland Maxillary artery and superficial temporal artery. 2. Retromandibular vein : Formed by union of sup. Temporal and maxillary vein joins post. Auricular vein to form the external jugular vein. 3.The facial nerve: Enters upper part of posteromedial border and divides into:
- 17. Nerve supply of parotid gland: Ō¢¬ Parasympathetic fibres :- Secretomotor Ō¢¬ Preganglionic fibres arise from the inferior salivatory nucleus Ō¢¬ Pass through glossopharyngeal nerve Ō¢¬ Relay in ottic ganglion Ō¢¬ Postganglionic fibres reach the gland through auriculotemporal nerve Ō¢¬ Sympathetic fibres :- Vasomotor Ō¢¬ Sensory nerves :- Auriculotemporal nerve
- 19. Rule of 80ŌĆÖs: 80% of parotid tumors are benign. ŌĆó 80% of parotid tumors are Pleomorphic adenomas. ŌĆó 80% of salivary gland Pleomorphic adenomas occur in the parotid . ŌĆó 80% of parotid Pleomorphic adenomas occur in the superficial lobe. ŌĆó 80% of untreated Pleomorphic adenomas remain benign.
- 20. Epidemiology: ŌĆó Uncommon neoplasms. ŌĆó 2%-3%of all head and neck neoplasms. ŌĆó Most salivary gland tumors originate in the parotid glands (64%-80%), malignancy (15%- 32%). ŌĆó 7-11% occur in the submandibular glands, malignancy (37% - 45%). ŌĆó less than 1% in the sublingual glands,malignancy (70%-90%), Ō¢¬ 9%-23% in the minor glands. ŌĆó Benign tumors account for 63% to 78% of all salivary gland neoplasms.
- 21. Etiology: ŌĆó Viruses- EBV, CMV, Polyoma virus ŌĆó Ionizing radiation. ŌĆó Increased occupational risks- asbestos, nickel compounds or silica dust. ŌĆó Employment in the woodworking, rubber industries & beauty saloons. ŌĆó Lifestyle- WarthinŌĆÖs tumors showed a strong association with cigarette smoking. ŌĆó Endogenous hormones.
- 22. Parotid neoplasms: Ō¢¬ Benign Ō¢¬ Pleomorphic adenoma ( MC benign ) Ō¢¬ WarthinŌĆÖs tumor ( 2nd MC Benign ) Ō¢¬ Malignant Ō¢¬ Mucoepidermoid carcinoma ( Highest Malignant Potential ) Ō¢¬ Adenoid cystic carcinoma Ō¢¬ Acinic cell carcinoma ( Most Painful ) Ō¢¬ Adenocarcinoma Ō¢¬ Squamous cell carcinoma ( Most Aggressive )
- 23. Etiology:
- 24. Pleomorphic adenoma: Ō¢¬ It is also known as ŌĆ£Mixed salivary tumorŌĆØ Ō¢¬ It is the most common benign tumor of salivary glands ŌĆō 80 % Ō¢¬ Characterized by neoplastic proliferation of parenchymatous glandular cells along with myoepithelial components 60-70%- Parotid glands ,40-60%- Submandibular glands, 40-70%- Minor salivary glands Seldomly- Sublingual glands. Age: 30-50 years Sex: female> male ŌĆō 3:1 ŌĆō 4:1 1. In Parotid- Presents in the superior lobe as a mass over the angle of the mandible, below and infront of the ear. 2. Painless, slow growing, firm mass, initially small in size and begins to increase in size. 3. Recurrent tumor- multinodular, fixed on palpation. 4. Palate ŌĆō intraorally common site.
- 25. WarthinŌĆÖs tumor: ŌĆó WarthinŌĆÖs tumour, also known as adenolymphoma or cystadenoma lymphomatosum, is a benign tumour. ŌĆó They are the second most common benign salivary gland tumours (5ŌĆō15%) Mainly seen in older men, after the 5th & 6th decade of life. ŌĆó They have been associated with cigarette smoking as well as radiation exposure. ŌĆó They are almost exclusively seen in the parotid gland, especially in the inferior pole, and are rarely seen in the peri-parotid nodes. ŌĆó They can occur synchronously or metachronously in the same or bilateral glands. (10-15% Bilateral) ŌĆó They are also known to occur with other salivary gland neoplasms such as pleomorphic adenoma and salivary duct carcinoma. ŌĆó Clinically, they present as painless, small slow-growing soft cystic fluctuant swellings. Facial palsy is rare. Malignant transformation is extremely rare. Recurrences are very rare and may be due to multifocal tumours.
- 26. Mucoepidermoid tumor: Ō¢¬ Commonest type of malignant salivary tumor in adults Ō¢¬ Commonest malignant tumor of parotid in childhood Ō¢¬ Common in middle age (35-65 years of age) Ō¢¬ Female predilection Blue / Red in color Ō¢¬ Parotid is the most common site of tumor Ō¢¬ 2nd common is palate minor salivary gland Ō¢¬ Radiation ŌĆō etiological factor Ō¢¬ t(11;19)(q21;p13) chromosome translocation resulting in a MECT1-MAML2 fusion gene Ō¢¬ Presents as painless, slow-growing mass that is firm or hard. Ō¢¬ Grossly ŌĆō Un encapsulated mass with cystic spaces Ō¢¬ Facial nerve involvement in late stages
- 27. ADENOID CYSTIC CARCINOMA ŌĆó Slow growing, aggressive neoplasm. ŌĆó 2nd MC malignant tumor. ŌĆó Common malignant tumor- submandibular, sublingual & minor salivary , ŌĆó 2/3rd ŌĆō occurs in minor salivary glands. ŌĆó Clinical Features: 1) MC seen in females’āĀ 5th -6th decade. Local recurrence common (30-50%). 2) Parotid, submaxillary, palate & tongue - MC involved. 3) Early local pain (surface ulceration), FN palsy, local invasion & fixation to deeper structure. LN metastasis’āĀ 10%-30%. ŌĆó 4) Tendency to spread through perineural spaces (20%-30%) ŌĆó Commonly involved nerves- Facial nerve, mandibular & maxillary nerve’āĀ Pathway for invasion of the skull base. ŌĆó More frequent- advanced, recurrent & high grade tumors.
- 28. Acinic cell carcinoma 3rd most comman malignant Ca. of parotid gland. Low malignancy. M:F=3:2, More common in males mainly in middle ages (44yrs) Tumor may be multifocal or B/L. Clinically ŌĆō Painless lump, Encapsulated & lobulated. Chiefly occurs’āĀ Parotid (80%) ŌĆó Most common intraoral site’āĀ Lips & buccal mucosa ŌĆó Local recurrence & distal metastasis. Has the best survival rate of any salivary cancer. ŌĆó Excision of a facial nerve is not justified unless it is involved.
- 29. Squamous cell carcinoma: ŌĆó Primary salivary gland SCC is very rare(<1%) Ō¢¬ Parotid (80%), submandibular gland(20%) ŌĆó Age : 60 to 65years, M:F= 2:1. ŌĆó History of previous radiotherapy.
- 30. Grade of tumor: Ō¢¬ Low grade: Ō¢¬ Well-differentiated cells with little cellular atypia Ō¢¬ High proportion of mucous cells Ō¢¬ Prominent cyst formation Ō¢¬ Intermediate grade: intermediate features Ō¢¬ High grade: Ō¢¬ Poorly differentiated with cellular pleomorphism Ō¢¬ High proportion of squamous cells Ō¢¬ Solid with few if any cysts
- 31. Malignancy should be suspected when: ’ü▒ Rapid growth ’ü▒ Facial nerve palsy ’ü▒ Painful ’ü▒ Skin infiltration ’ü▒ Get fixed to massester muscle ’āĀ Trismus ’ü▒ Feels stony hard ’ü▒ Presence of lymph nodes in neck
- 32. Prognostic factors ’ü▒ Histopathological diagnosis ’ü▒ Facial nerve paralysis ’ü▒ Skin involvement ’ü▒ Stage ’ü▒ Location ’ü▒ Incidence of recurrence ’ü▒ Distant metastasis ’ü▒ Radiotherapeutic sensitivity ’ü▒ Chemotherapeutic sensitivity
- 33. TNM classification of carcinomas of the major salivary glands
- 34. Main investigations: ( USG,FNAC & CT Scan ) Ō¢¬ FNAC:- 1) Accuracy’āĀ95-98% 2) Diff benign from malignant disease. 3) The key to successful FNAC is immediate evaluation of the specimen for adequacy. Ultrasound: 1) Ideal tool for the initial assessment of superficially located tumors of the parotid and submandibular gland’āĀ Distinguish intrinsic from extrinsic neoplasm. 2) USG f/o malignant tumors include ill-defined margins, heterogeneous architecture, subcutaneous invasion, & the presence of LN metastases.
- 35. CT & MRI: 1) Effective modalities for imaging the size, the local, and the regional extension of the primary tumor and the neck metastasis & to differentiate intra from extra glandular mass. 2) CT’āĀ IOC for subtle cortical involvement & bone destruction. 3) MRI’āĀ IOC for bone marrow invasion. 4) MRI’āĀIOC for detecting perineural spread. 5) Contrast-enhanced MRI’āĀ IOC for intracranial invasion Disadvantage Of MRI :- 1) Less sensitive in cystic lesions. 2) Inability to detect calcification.
- 36. Investigations: 1 )Plain X ray 2) X ray chest’āĀ To R/O secondaries. 3) OPG’āĀ To R/O mandibular involvement. 4) Open biopsy’āĀ Rarely used due to risk of recurrence & FN damage’āĀ Useful HP guidance for use of palliative CTRT, poor surgical candidate, obvious malignancy. 5) Sialography:- a) C/I:-Acute infection, Iodine allergy, Multiple myeloma. b) Limitation:- Mass < 2mm, Deep lobe pathology. 6) Radiosialography’āĀ Tc99’āĀ To detect mass lesion & parenchyma function’āĀ No use in ductal system study. 7) Colour doppler sonography’āĀ Non invasive ’āĀ Evaluates vascular anatomy. 8) PET’āĀ Differentiate benign from malignant lesions.
- 37. Treatment: ( Parotidectomy ) Ō¢¬ Indications: Ō¢¬ Chronic parotitis Ō¢¬ Salivary calculi Ō¢¬ Parotid tumors Ō¢¬ T1,T2,T3 ŌĆō Total conservative parotidectomy Ō¢¬ T4 ŌĆō Radical parotidectomy Ō¢¬ Types: Ō¢¬ Superficial parotidectomy Ō¢¬ Total conservative parotidectomy Ō¢¬ Radical parotidectomy
- 38. Indications of facial nerve sacrifice: Ō¢¬ Preoperative weakness / paralysis of nerve Ō¢¬ Intraoperative evidence of gross invasion Ō¢¬ Tumors transgressing through facial nerve from superficial to deep lobe Ō¢¬ Nerve stump is checked for frozen section for negative margins, if positive, mastoidectomy & nerve dissection is required
- 39. Indications of PORT: Ō¢¬ 1) High-grade tumor Ō¢¬ 2) Deep lobe cancers Ō¢¬ 3) All T3 and T4 cancers Ō¢¬ 4) Recurrent disease Ō¢¬ 5) Documented LN metastasis Ō¢¬ 6) Extraparotid extension Ō¢¬ 7) Gross/microscopic residual disease Ō¢¬ 8) Tumor involving or close to the facial nerve. 1) Clinically cervical Lympadenopathies (15%). 2) Parotid tumor bigger than 4cm’āĀ Occult metastasis risk >20%. 3) High grade malignancy’āĀ Occult metastasis risk >25%. Indications of neck dissection:
- 40. Treatment plan of parotid gland tumors:
- 42. Treatment:
- 43. Chemotherapy useful in pallation & in inoperable cases. Combination regimen have not proven better results 2 groups Epidermoid like tumor i.e. Sq. cell CA Mucoepidermoid Ca. Adeno Ca like tumors i.e. Adenoid cystic Ca, Acinic cell Ca, Ca. ex polymorphic Ca Methotrexate Cisplatin Adriamycin Cisplatin 5-flurouracil COMPLICATIONS OF PAROTID SURGERY
- 44. THANK YOU TILL NEXT ░š▒§▓čĘĪŌĆ”ŌČ─”ŌČ─”ŌČ─”