Typhoid fever
ŌĆó
2 likesŌĆó517 views

Typhoid fever is caused by the bacterium Salmonella Typhi. It affects 17 million people worldwide each year. The presentation summarized the causative agent, epidemiology, symptoms, diagnosis, treatment, prevention and nursing care for typhoid fever. Key points include that it is transmitted through contaminated food or water and symptoms include sustained fever, abdominal pain and rose colored spots. Diagnosis involves blood and stool cultures. Treatment involves antibiotics like chloramphenicol or fluoroquinolones for 2-4 weeks. Prevention requires safe food handling and sanitation. Nursing care focuses on bedside care, monitoring symptoms and educating family.







![Symptoms
ŌĆó Fever [usually higher in the
evening]
- Intermittent Fever initially
- Sustained Fever to high
temperatures later](https://image.slidesharecdn.com/typhoid-210710184817/85/Typhoid-fever-10-320.jpg)



















Typhoid fever
- 2. Other names: ŌĆó Enteric Fever ŌĆó Bilious Fever ŌĆó Yellow Jack
- 4. 3 main antigenic factors: ŌĆó the O, or somatic antigen ŌĆó the Vi, or encapsulation antigen ŌĆó the H, or flagellar antigen
- 5. Epidemiology ŌĆó World: 17 million cases per year ŌĆó U.S.: 400 cases per year (70% in travelers) ŌĆó Philippines: (Nov 2006) 478 in Agusan del Sur; (May 2004) 292 in Bacolod City
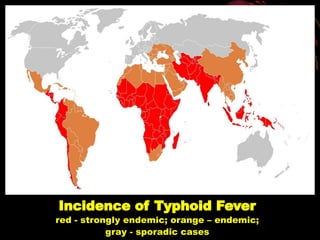
- 6. Incidence of Typhoid Fever red - strongly endemic; orange ŌĆō endemic; gray - sporadic cases
- 7. Mode of Transmission Ingestion of contaminated food or water; rarely from person to person transmission through fecal-oral route.
- 8. Incubation Period First 7-14 days after ingestion
- 9. Symptoms ŌĆó Diarrhea may occur ŌĆó Active infection ŌĆó Severe Headache ŌĆó Generalized Abdominal Pain ŌĆó Anorexia
- 10. Symptoms ŌĆó Fever [usually higher in the evening] - Intermittent Fever initially - Sustained Fever to high temperatures later
- 11. Symptoms Severe cases ŌĆó ulcers on the intestinal wall ŌĆó shock ŌĆó delirium ŌĆó stupor
- 12. Pathognomonic Sign ŌĆó Rose Spots Blanching pink macular spots 2-3 mm over trunk
- 13. Complications Intestinal perforation, gastrointestinal hemorrhage and peritonitis may occur in the 3rd and 4th week of illness; rarely pancreatitis, hepatic and splenic abscesses, disseminated intravascular coagulation, myocarditis, meningitis, encephalitis.
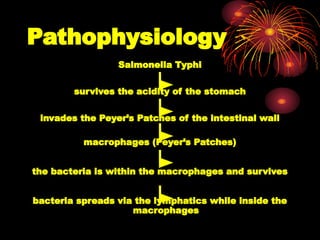
- 14. Pathophysiology Salmonella Typhi survives the acidity of the stomach invades the PeyerŌĆÖs Patches of the intestinal wall macrophages (PeyerŌĆÖs Patches) the bacteria is within the macrophages and survives bacteria spreads via the lymphatics while inside the macrophages
- 15. Pathophysiology access to Reticuloendothelial system, liver, spleen, gallbladder and bone marrow First week: elevation of the body temperature Second week: abdominal pain, spleen enlargement and rose spots Third week: necrosis of the PeyerŌĆÖs Patches leads to perforation, bleeding and, if left untreated, death is imminent
- 16. Diagnostics CBC (normal WBC despite fever), platelet count Tourniquet Test
- 17. Diagnostics Typhi dot test (if illness is 4 days or longer) Interpretation: Ig M Ig G (+) (- ) Acute infection (+) (+) Recent infection (- ) (+) Equivocal: Past infection or acute infection
- 18. Diagnostics Malarial smear (Differential diagnosis) Chest X-ray Urinalysis
- 19. Diagnostics First Week of illness: Blood C/S Second Week of illness: Urine G/S, C/S Third Week of illness: Stool C/S
- 20. Management A. Prevention: ŌĆó Choose foods processed for safety ŌĆó Prepare food carefully ŌĆó Foods prepared by others (avoid if possible)
- 21. Management ŌĆó Keep food contact surfaces clean ŌĆó Eat cooked food as soon as possible ŌĆó Maintain clean hands
- 22. Management ŌĆó Steam or boil shellfish at least 10 minutes ŌĆó All milk and dairy products should be pasteurized ŌĆó Control fly populations
- 23. Management B. Antibiotics For uncomplicated cases, use Conventional Therapy: 1. Chloramphenicol 3-4 gm per day PO in 4 divided doses x 14 days (50-100 mg/kg BW) except it with low WBC. 2. Co-trimoxazole forte or double-strength tab BID PO x 14 days 3. Amoxicillin 4-6 gm per day PO in 3 divided doses x 14 days
- 24. Management For cases with complications, presence of severe symptoms, or clinical deterioration despite conventional therapy, use Empiric Therapy for Suspected Resistant Typhoid Fever: 1. Ceftriaxone (Rocephin) 3 gm IV infusion OD x 5-7 days Ceftriaxone may be used for pregnant women and children. 2. Fluoroquinolones: Ciprofloxacin (Ciprobay) 500 mg tab PO BID x 7-10 days Ofloxacin (Inoflox) 400 mg tab PO BID x 7-10 days Perfloxacin (Floxin) 400 mg tab PO BID x 7-10 days
- 25. Management C. Vaccines 5 years 1 capsule every other day, total of 3 capsules Oral 6 years Ty21 a, live 3 years 0.5 ml Subcutaneous 2 years Vi CPS 3 years 0.5 ml (0.25 ml for children < 10y) x 2 times, 4 weeks apart Subcutaneous 5 years Killed whole-cell vaccine Revaccination Dosage Route Age Vaccine
- 26. Management D. Public Health Nursing Responsibility - Teach members of the family how to report all symptoms to the attending physician especially when patient is being cared for at home.
- 27. Management - Teach, guide and supervise members of the family on nursing techniques which will contribute to the patientŌĆÖs recovery.
- 28. Management - Interpret to family nature of disease and need for practicing preventive and control measures.
- 29. Management E. Nursing Care - Demonstrate to family how to give bedside care, such as tepid sponge bath, feeding, changing of bed linen, use of bedpan and mouth care.
- 30. Management - Any bleeding from the rectum, blood in stools, sudden acute abdominal pain, restlessness, falling of temperature should be reported at once to the physician or the patient should be brought at once to the hospital.
- 31. Management - Take TPR, I&O and teach family members how to take and record same.
- 32. Historical Background Mary Mallon (September 23, 1869 ŌĆō November 11, 1938)
- 33. Thank you!