Univentricular circulation
Download as pptx, pdf1 like888 views
This document discusses cardiovascular physiology concepts related to cardiac output, blood flow distribution, and oxygen delivery and utilization in the body. It covers topics like the factors that affect cardiac output, regional resistance factors, blood flow redistribution, and the relationships between cardiac output, blood flow ratios in the pulmonary and systemic circulations, oxygen saturation levels, and oxygen delivery. The key ideas are that optimal oxygen delivery occurs at a pulmonary to systemic flow ratio of 1, with the lowest total cardiac output, and that subtle imbalances can significantly impact oxygen saturation and delivery levels.
1 of 18
Download to read offline
Ad
Recommended
Fluid manage 최종[1]
Fluid manage 최종[1]Seungyoun Kang
Ěý
1. Maintaining adequate oxygen delivery to tissues is important for shock patients. This involves optimizing factors like cardiac output, hemoglobin, and oxygen saturation through fluid resuscitation and vasopressor support if needed.
2. Hypovolemic shock results from a loss of intravascular volume that exceeds 15% of total blood volume. Rapid volume replacement is critical to restore tissue perfusion and prevent end-organ damage.
3. Crystalloids and colloids can both be used for initial fluid resuscitation in bleeding shock, with colloids being more effective at expanding plasma volume. Albumin, hetastarch, and gelatin are options for colloid fluid resuscitation.Regional circulations by rajnee
Regional circulations by rajneeDRRAJNEE
Ěý
The document discusses regional circulations, focusing on coronary, cerebral, and cutaneous circulation. It provides details on the anatomy, blood supply, regulation, and clinical implications of each circulation. For coronary circulation, it describes the blood vessels that supply the heart muscle and how blood flow is regulated to meet myocardial oxygen demands. For cerebral circulation, it outlines the unique anatomical features of the brain's blood supply and factors that control blood flow. For cutaneous circulation, it explains the role of arteriovenous anastomoses and arterioles in regulating heat transfer and sympathetic nervous system control of cutaneous blood flow.Physiology part1
Physiology part1Tamara Chávez
Ěý
The document discusses the physiology of fluid distribution in the body, highlighting the division into intracellular and extracellular compartments, with key solutes such as sodium and albumin playing crucial roles in osmolarity and volume regulation. It covers mechanisms of hormonal regulation by aldosterone and anti-diuretic hormone, factors influencing renal function, and the dynamics of hydrostatic and oncotic pressures affecting fluid flux. Additionally, it addresses pathology related to fluid disturbances, including causes and types of edema and pulmonary edema, as well as methods for measuring blood volume and compartmental distribution.Physio Renal 5.
Physio Renal 5.Shaikhani.
Ěý
The document discusses control of sodium excretion and extracellular fluid volume through various mechanisms:
1. Sodium excretion is controlled by ADH, thirst, salt appetite, and cardiovascular reflexes.
2. Extracellular sodium and osmolarity are controlled by an osmoreceptor feedback system involving ADH and thirst, as well as salt appetite at low sodium levels.
3. Aldosterone regulates sodium absorption in the distal tubules and sodium excretion is well-controlled even without aldosterone feedback through mechanisms like ADH and thirst.Tonicity disorders v2
Tonicity disorders v2qbank org
Ěý
The document discusses water and sodium balance in the body and various disorders that can arise from imbalances. It begins by explaining the concept of balance between fluids, electrolytes, and compartments in the body. It then discusses various sodium, water, and volume disorders like hyponatremia, hypernatremia, hypovolumia, hypervolemia, and their causes. It provides details on pseudohyponatremia and different types of dehydration. Treatment approaches for various disorders are summarized. Overall, the document provides a comprehensive overview of fluid, electrolyte, and acid-base balance in the human body.Pathophysiology of Acute Renal Faliure
Pathophysiology of Acute Renal FaliureARK College of Pharmacy, Kaushambi, UP
Ěý
Acute renal failure (ARF), also known as acute kidney failure (AKI), is characterized by a sudden decline in renal function, leading to an increase in serum creatinine and a decrease in glomerular filtration rate (GFR). The condition can be categorized into pre-renal, intra-renal, and post-renal causes, with symptoms including oliguria, fatigue, and muscle tenderness. Management involves dietary adjustments, intravenous therapy, diuretics, and potential dialysis to address metabolic imbalances and remove toxins.intracranial pressure
intracranial pressuregeeta joshi
Ěý
The document discusses intracranial pressure (ICP), detailing its components, normal values, and causes of increased ICP such as brain volume change, blood volume increases, and CSF volume abnormalities. It also outlines the pathophysiology, symptoms, and manifestations of increased ICP as well as potential management strategies, including osmotic diuretics and interventions to maintain cerebral perfusion. Key points include the effects of increased ICP on cognition and the importance of monitoring and maintaining appropriate blood pressure and oxygenation.Body fluids and electrolytes
Body fluids and electrolytesLafee H. Alfa'ous
Ěý
The document provides an overview of body fluids and electrolytes, detailing the distribution of fluid in the human body, types of body fluids, and their compositions. It discusses the significance of sodium, potassium, magnesium, calcium, and chloride ions in maintaining fluid balance and lists disorders such as hypernatremia and hyponatremia, along with their causes, symptoms, and management strategies. Treatment protocols for electrolyte imbalances are also outlined, emphasizing the importance of careful correction to prevent complications.Oxygen therapy
Oxygen therapy Surendra Patel
Ěý
Oxygen is a vital gas necessary for bodily functions and should be treated as a drug for hypoxemia, not for general breathlessness. The document details the physiological processes of oxygen transport, therapeutic applications, and the importance of monitoring and proper administration of oxygen therapy, highlighting the risks associated with oxygen toxicity and pulmonary complications. It emphasizes the need for careful assessment and tailored oxygen delivery based on individual patient conditions.Oxygen therapy and physiology
Oxygen therapy and physiologybhavya226982
Ěý
This document provides an overview of oxygen therapy. It discusses oxygen transport and delivery in the body, including how oxygen levels decrease from the atmosphere to tissues. It outlines indications for oxygen therapy when hypoxemia is present. Various oxygen delivery devices are described, including nasal cannulas, masks, and catheters. Low-flow systems provide variable oxygen concentrations while high-flow systems and reservoir masks provide more consistent fixed concentrations. Complications of oxygen therapy are also mentioned.Seminar on oxygen insufficiency
Seminar on oxygen insufficiencySimran Kaur
Ěý
This document provides information on oxygen insufficiency and discusses key points:
- Oxygen is essential for life and is involved in cellular respiration. It makes up 20.94% of air by volume.
- Oxygen insufficiency, or hypoxia, occurs when oxygen delivery to tissues is inadequate to meet metabolic demands. This can be caused by problems with ventilation, gas exchange, oxygen transport, or cellular respiration.
- Symptoms of hypoxia range from shortness of breath to confusion and loss of consciousness. Diagnostic tests for hypoxia include blood gas analysis, pulse oximetry, pulmonary function tests, and imaging studies.
- Nursing management of patients with oxygen insufficiency focuses onTissue oxygenation
Tissue oxygenationmauryaramgopal
Ěý
Tissue oxygenation involves the cascade of oxygen from the atmosphere to the mitochondria in cells. Oxygen partial pressure progressively decreases from 150 mmHg in inspired air to 10-20 mmHg in cell mitochondria. Factors like ventilation, cardiac output, hemoglobin levels, and oxygen consumption can impact oxygen levels at different points in the cascade. Clinicians assess tissue oxygenation using variables derived from oxygen delivery and uptake, such as oxygen saturation, lactate levels, and base deficit. Monitoring these factors provides insight into a patient's oxygenation status.CO2 gap and lactic acidosis in critical care
CO2 gap and lactic acidosis in critical careDeepika317565
Ěý
A type appoach in intensive care unit
Basic knowledge about CO2 production and circulation
Importance to Carbon dioxide in the management of critically ill
Useful in categorizing patients
Classify various types of shock
Classic hypoxia
Identify the cause of failure and deterioration of clinical status of patient
Helps guide therapy for patients in circulatory failure
Throws light About lactic acidosis,it's formation , circulation, metabolism and monitoring Shock Kuliah Residen.pptx
Shock Kuliah Residen.pptxAdindaNurulHuda1
Ěý
Shock is defined as an acute circulatory dysfunction resulting in inadequate tissue perfusion. It occurs when oxygen demand exceeds supply due to disturbances in the oxygen transport cascade. The key variables in oxygen transport are oxygen delivery (DO2), oxygen content (CaO2), cardiac output (CO), and oxygen uptake (VO2). In shock, oxygen extraction increases (higher ER) to compensate for low DO2 until end-organ dysfunction occurs. Shock progresses from compensated to uncompensated states and can be classified as hypovolemic, cardiogenic, distributive, or obstructive. Assessment involves monitoring vital signs, urine output, and markers of tissue perfusion like lactate to guide resuscitation goals.Vso2(venous oximetry) mixed venous o2 sat
Vso2(venous oximetry) mixed venous o2 satHossam atef
Ěý
1. Mixed venous blood is a mixture of blood from the systemic veins excluding shunted blood, with components from the superior vena cava, inferior vena cava, and coronary sinus.
2. Sustained tissue hypoxia is a major factor in the development of multiorgan failure. Mixed venous oximetry can measure the balance between oxygen delivery and demand.
3. Central venous oxygen saturation (ScvO2) closely parallels mixed venous oxygen saturation (SvO2) but may be 7-10% higher in shock states, due to regional variations in blood flow and oxygen supply/demand.Vso2(venous oximetry) mixed venous o2 sat
Vso2(venous oximetry) mixed venous o2 satHossam atef
Ěý
1. Mixed venous blood is a mixture of blood from the systemic veins that has undergone gas exchange in the tissues, excluding shunted blood. It provides information on the balance between oxygen delivery and consumption on a systemic level.
2. The mixed venous oxygen saturation (SvO2) reflects this balance, with a normal value around 75%. A low SvO2 indicates oxygen delivery is not meeting tissue demands, while a high SvO2 suggests impaired tissue extraction of oxygen.
3. The central venous oxygen saturation (ScvO2) approximates SvO2 but is usually a few points higher. Both can help guide resuscitation in shock states like sepsis when used as targets forOxygen cascade & therapy
Oxygen cascade & therapyDr. Taraknath Chatterjee
Ěý
The document discusses the mechanics of gas exchange and oxygen transportation in the human body, emphasizing the significance of partial pressures, the oxygen cascade, and hemoglobin's oxygen-binding properties. It also covers the clinical aspects of oxygen therapy, including indications, delivery systems, and the importance of individual target saturation levels for different patient populations. It concludes with a warning about the potential toxic effects of prolonged high concentrations of oxygen.OXYGEN THERAPHY.pptx
OXYGEN THERAPHY.pptxdrrajugandham1
Ěý
The document discusses oxygen therapy and administration, including the types of oxygen delivery systems like nasal cannulas, simple face masks, and reservoir masks. It covers indications for oxygen therapy when hypoxemia is present based on arterial blood gas values. Equations are provided for calculating oxygen content, delivery, uptake, and extraction from the blood under normal conditions.Oxygen therapy 2021
Oxygen therapy 2021Assist. Prof. Radhwan Hazem Alkhashab
Ěý
Oxygen therapy aims to increase alveolar oxygen levels in hypoxemic patients. It is important to monitor cardiovascular parameters like mixed venous oxygen saturation to optimize oxygen delivery and consumption balance. Different devices can deliver varying concentrations of oxygen depending on the condition. High concentrations over long periods can cause toxicity issues like pulmonary fibrosis or retrolental fibroplasia in neonates. The risks and benefits of oxygen therapy must be carefully considered.oxygenation ppt Gk
oxygenation ppt Gk GhaziKumbher
Ěý
This document provides an overview of oxygenation, respiration, and the cardiovascular system. It defines key terms related to oxygenation and discusses the mechanisms of respiration and the cardiovascular system. Factors that can affect oxygenation are explained. Common manifestations of altered respiratory and cardiovascular function include hypoxia, altered breathing patterns, decreased cardiac output, and impaired tissue perfusion. Nursing measures to ensure patient airway and emergencies related to the respiratory and cardiovascular systems are also outlined. The document concludes by differentiating between medical and surgical asepsis.Alveolar gases and diffusion
Alveolar gases and diffusionGeorge Wild
Ěý
The document discusses alveolar and arterial gases and diffusion across the respiratory membrane. It introduces key terms like PACO2, PAO2, PaCO2 and PaO2. It explains that alveolar levels determine arterial levels through diffusion. Factors like ventilation rate, oxygen concentration, and metabolism can affect both alveolar and arterial gas levels. Optimal ventilation-perfusion matching is needed for efficient gas exchange and delivery of oxygen to tissues while removing carbon dioxide.Acute Respiratory Failure
Acute Respiratory FailureDang Thanh Tuan
Ěý
Acute respiratory failure is a life-threatening condition caused by the failure of oxygen and carbon dioxide exchange in the lungs. Prompt recognition and initiation of supportive treatments like oxygen supplementation are crucial for successful outcomes. Blood gas analysis helps differentiate between pulmonary and extra-pulmonary causes of hypoxemia and hypercapnia, with an increased alveolar-arterial oxygen difference being a sensitive indicator of respiratory diseases interfering with gas exchange. Management involves treating the underlying etiology, providing oxygen, and considering intubation and mechanical ventilation for persistent hypoxemia, progressive acidosis, or altered mental status.A C U T E R E S P I R A T O R Y F A I L U R E
A C U T E R E S P I R A T O R Y F A I L U R EDang Thanh Tuan
Ěý
Acute respiratory failure is a life-threatening condition caused by the failure of oxygen and carbon dioxide exchange in the lungs. Prompt recognition and initiation of supportive treatments like oxygen supplementation are crucial for successful outcomes. Blood gas analysis helps differentiate between pulmonary and extra-pulmonary causes of hypoxemia and hypercapnia, with an increased alveolar-arterial oxygen difference being a sensitive indicator of respiratory diseases interfering with gas exchange. Management involves treating the underlying etiology, providing oxygen, and considering intubation and mechanical ventilation for persistent hypoxemia, progressive acidosis, or altered mental status.High output cardiac failure
High output cardiac failureUscom - Presentations
Ěý
High Output Cardiac Failure
The tissues, not the heart, determine cardiac output by controlling local blood flow through vasodilation in response to changes in oxygen and carbon dioxide levels. As vascular resistance decreases, stroke volume increases, maintaining blood pressure. A high cardiac output becomes "high output failure" when blood pressure cannot be maintained against low systemic vascular resistance, or oxygen delivery is insufficient. The diagnostic triad is high cardiac output, low blood pressure, and very low systemic vascular resistance. Treatment focuses on balancing oxygen delivery and demand by optimizing preload, contractility, and afterload through fluid administration and inotropic support tailored to individual hemodynamic parameters.Monitoring Hypoxia and oxygen supplementation
Monitoring Hypoxia and oxygen supplementationYouttam Laudari
Ěý
1) Hypoxia can lead to decreased ATP synthesis, lactic acidosis, impaired protein synthesis, and irreversible cell changes due to increased cytosolic calcium.
2) Pao2, Sao2, and oxygen content are important measures of oxygen levels in the blood. Pulse oximetry can monitor Sao2 non-invasively but has limitations.
3) Arterial blood gas analysis precisely measures oxygen, carbon dioxide, pH, and bicarbonate levels to assess oxygenation and ventilation.Hypoxia today
Hypoxia todayYouttam Laudari
Ěý
1) Hypoxia can lead to decreased ATP synthesis, lactic acidosis, impaired protein synthesis, and irreversible cell changes due to increased cytosolic calcium.
2) Pao2, Sao2, and oxygen content are important measures of oxygen levels in the blood. Pulse oximetry can monitor Sao2 non-invasively but has limitations.
3) Arterial blood gas analysis precisely measures oxygen, carbon dioxide, pH, bicarbonate, and base excess levels to evaluate oxygenation and ventilation.Acute resp failure.pptx
Acute resp failure.pptxDipali Dumbre
Ěý
This document discusses gas exchange and respiratory failure. It defines hypoxemic respiratory failure as inadequate oxygen transfer resulting in low arterial oxygen levels, and hypercapnic respiratory failure as insufficient carbon dioxide removal leading to high arterial carbon dioxide levels. The major mechanisms of hypoxemic failure are ventilation-perfusion mismatching, shunting, diffusion limitation, and hypoventilation, while hypercapnic failure results from an imbalance between ventilatory supply and demand. Diseases like pneumonia, pulmonary edema, and COPD can cause either type of respiratory failure through various pathophysiological mechanisms.Ebstein Anomaly
Ebstein AnomalyDr. Abhinav Agarwal
Ěý
The document discusses congenital heart defects, particularly focusing on conditions like Ebstein's anomaly, which affects <1% of patients and shows a prevalence of 2.4/10,000. It outlines associated symptoms, genetic factors, treatment options, and long-term prognosis, including survival rates and likelihood of reoperation. Key management strategies for affected patients include various surgical interventions and considerations for arrhythmias.Pah management
Pah managementDr. Abhinav Agarwal
Ěý
This document summarizes key information about pulmonary hypertension (PH) management including: median survival rates; clinical presentation; diagnostic testing including echocardiogram, right heart catheterization, and biomarkers; risk assessment; and therapy. Median survival is 2.8 years for adults and 10 months for pediatric patients with PH. Clinical presentation includes symptoms of exertional shortness of breath, fatigue, and right ventricular failure. Diagnostic testing is aimed at confirming the diagnosis, assessing severity, and identifying the cause of PH. Risk assessment evaluates factors like functional capacity, right ventricular function, and complications to determine low, intermediate, or high risk status. Therapy involves general measures, PH-specific drug therapy, and interventional procedures in advanced cases.More Related Content
Similar to Univentricular circulation (20)
Oxygen therapy
Oxygen therapy Surendra Patel
Ěý
Oxygen is a vital gas necessary for bodily functions and should be treated as a drug for hypoxemia, not for general breathlessness. The document details the physiological processes of oxygen transport, therapeutic applications, and the importance of monitoring and proper administration of oxygen therapy, highlighting the risks associated with oxygen toxicity and pulmonary complications. It emphasizes the need for careful assessment and tailored oxygen delivery based on individual patient conditions.Oxygen therapy and physiology
Oxygen therapy and physiologybhavya226982
Ěý
This document provides an overview of oxygen therapy. It discusses oxygen transport and delivery in the body, including how oxygen levels decrease from the atmosphere to tissues. It outlines indications for oxygen therapy when hypoxemia is present. Various oxygen delivery devices are described, including nasal cannulas, masks, and catheters. Low-flow systems provide variable oxygen concentrations while high-flow systems and reservoir masks provide more consistent fixed concentrations. Complications of oxygen therapy are also mentioned.Seminar on oxygen insufficiency
Seminar on oxygen insufficiencySimran Kaur
Ěý
This document provides information on oxygen insufficiency and discusses key points:
- Oxygen is essential for life and is involved in cellular respiration. It makes up 20.94% of air by volume.
- Oxygen insufficiency, or hypoxia, occurs when oxygen delivery to tissues is inadequate to meet metabolic demands. This can be caused by problems with ventilation, gas exchange, oxygen transport, or cellular respiration.
- Symptoms of hypoxia range from shortness of breath to confusion and loss of consciousness. Diagnostic tests for hypoxia include blood gas analysis, pulse oximetry, pulmonary function tests, and imaging studies.
- Nursing management of patients with oxygen insufficiency focuses onTissue oxygenation
Tissue oxygenationmauryaramgopal
Ěý
Tissue oxygenation involves the cascade of oxygen from the atmosphere to the mitochondria in cells. Oxygen partial pressure progressively decreases from 150 mmHg in inspired air to 10-20 mmHg in cell mitochondria. Factors like ventilation, cardiac output, hemoglobin levels, and oxygen consumption can impact oxygen levels at different points in the cascade. Clinicians assess tissue oxygenation using variables derived from oxygen delivery and uptake, such as oxygen saturation, lactate levels, and base deficit. Monitoring these factors provides insight into a patient's oxygenation status.CO2 gap and lactic acidosis in critical care
CO2 gap and lactic acidosis in critical careDeepika317565
Ěý
A type appoach in intensive care unit
Basic knowledge about CO2 production and circulation
Importance to Carbon dioxide in the management of critically ill
Useful in categorizing patients
Classify various types of shock
Classic hypoxia
Identify the cause of failure and deterioration of clinical status of patient
Helps guide therapy for patients in circulatory failure
Throws light About lactic acidosis,it's formation , circulation, metabolism and monitoring Shock Kuliah Residen.pptx
Shock Kuliah Residen.pptxAdindaNurulHuda1
Ěý
Shock is defined as an acute circulatory dysfunction resulting in inadequate tissue perfusion. It occurs when oxygen demand exceeds supply due to disturbances in the oxygen transport cascade. The key variables in oxygen transport are oxygen delivery (DO2), oxygen content (CaO2), cardiac output (CO), and oxygen uptake (VO2). In shock, oxygen extraction increases (higher ER) to compensate for low DO2 until end-organ dysfunction occurs. Shock progresses from compensated to uncompensated states and can be classified as hypovolemic, cardiogenic, distributive, or obstructive. Assessment involves monitoring vital signs, urine output, and markers of tissue perfusion like lactate to guide resuscitation goals.Vso2(venous oximetry) mixed venous o2 sat
Vso2(venous oximetry) mixed venous o2 satHossam atef
Ěý
1. Mixed venous blood is a mixture of blood from the systemic veins excluding shunted blood, with components from the superior vena cava, inferior vena cava, and coronary sinus.
2. Sustained tissue hypoxia is a major factor in the development of multiorgan failure. Mixed venous oximetry can measure the balance between oxygen delivery and demand.
3. Central venous oxygen saturation (ScvO2) closely parallels mixed venous oxygen saturation (SvO2) but may be 7-10% higher in shock states, due to regional variations in blood flow and oxygen supply/demand.Vso2(venous oximetry) mixed venous o2 sat
Vso2(venous oximetry) mixed venous o2 satHossam atef
Ěý
1. Mixed venous blood is a mixture of blood from the systemic veins that has undergone gas exchange in the tissues, excluding shunted blood. It provides information on the balance between oxygen delivery and consumption on a systemic level.
2. The mixed venous oxygen saturation (SvO2) reflects this balance, with a normal value around 75%. A low SvO2 indicates oxygen delivery is not meeting tissue demands, while a high SvO2 suggests impaired tissue extraction of oxygen.
3. The central venous oxygen saturation (ScvO2) approximates SvO2 but is usually a few points higher. Both can help guide resuscitation in shock states like sepsis when used as targets forOxygen cascade & therapy
Oxygen cascade & therapyDr. Taraknath Chatterjee
Ěý
The document discusses the mechanics of gas exchange and oxygen transportation in the human body, emphasizing the significance of partial pressures, the oxygen cascade, and hemoglobin's oxygen-binding properties. It also covers the clinical aspects of oxygen therapy, including indications, delivery systems, and the importance of individual target saturation levels for different patient populations. It concludes with a warning about the potential toxic effects of prolonged high concentrations of oxygen.OXYGEN THERAPHY.pptx
OXYGEN THERAPHY.pptxdrrajugandham1
Ěý
The document discusses oxygen therapy and administration, including the types of oxygen delivery systems like nasal cannulas, simple face masks, and reservoir masks. It covers indications for oxygen therapy when hypoxemia is present based on arterial blood gas values. Equations are provided for calculating oxygen content, delivery, uptake, and extraction from the blood under normal conditions.Oxygen therapy 2021
Oxygen therapy 2021Assist. Prof. Radhwan Hazem Alkhashab
Ěý
Oxygen therapy aims to increase alveolar oxygen levels in hypoxemic patients. It is important to monitor cardiovascular parameters like mixed venous oxygen saturation to optimize oxygen delivery and consumption balance. Different devices can deliver varying concentrations of oxygen depending on the condition. High concentrations over long periods can cause toxicity issues like pulmonary fibrosis or retrolental fibroplasia in neonates. The risks and benefits of oxygen therapy must be carefully considered.oxygenation ppt Gk
oxygenation ppt Gk GhaziKumbher
Ěý
This document provides an overview of oxygenation, respiration, and the cardiovascular system. It defines key terms related to oxygenation and discusses the mechanisms of respiration and the cardiovascular system. Factors that can affect oxygenation are explained. Common manifestations of altered respiratory and cardiovascular function include hypoxia, altered breathing patterns, decreased cardiac output, and impaired tissue perfusion. Nursing measures to ensure patient airway and emergencies related to the respiratory and cardiovascular systems are also outlined. The document concludes by differentiating between medical and surgical asepsis.Alveolar gases and diffusion
Alveolar gases and diffusionGeorge Wild
Ěý
The document discusses alveolar and arterial gases and diffusion across the respiratory membrane. It introduces key terms like PACO2, PAO2, PaCO2 and PaO2. It explains that alveolar levels determine arterial levels through diffusion. Factors like ventilation rate, oxygen concentration, and metabolism can affect both alveolar and arterial gas levels. Optimal ventilation-perfusion matching is needed for efficient gas exchange and delivery of oxygen to tissues while removing carbon dioxide.Acute Respiratory Failure
Acute Respiratory FailureDang Thanh Tuan
Ěý
Acute respiratory failure is a life-threatening condition caused by the failure of oxygen and carbon dioxide exchange in the lungs. Prompt recognition and initiation of supportive treatments like oxygen supplementation are crucial for successful outcomes. Blood gas analysis helps differentiate between pulmonary and extra-pulmonary causes of hypoxemia and hypercapnia, with an increased alveolar-arterial oxygen difference being a sensitive indicator of respiratory diseases interfering with gas exchange. Management involves treating the underlying etiology, providing oxygen, and considering intubation and mechanical ventilation for persistent hypoxemia, progressive acidosis, or altered mental status.A C U T E R E S P I R A T O R Y F A I L U R E
A C U T E R E S P I R A T O R Y F A I L U R EDang Thanh Tuan
Ěý
Acute respiratory failure is a life-threatening condition caused by the failure of oxygen and carbon dioxide exchange in the lungs. Prompt recognition and initiation of supportive treatments like oxygen supplementation are crucial for successful outcomes. Blood gas analysis helps differentiate between pulmonary and extra-pulmonary causes of hypoxemia and hypercapnia, with an increased alveolar-arterial oxygen difference being a sensitive indicator of respiratory diseases interfering with gas exchange. Management involves treating the underlying etiology, providing oxygen, and considering intubation and mechanical ventilation for persistent hypoxemia, progressive acidosis, or altered mental status.High output cardiac failure
High output cardiac failureUscom - Presentations
Ěý
High Output Cardiac Failure
The tissues, not the heart, determine cardiac output by controlling local blood flow through vasodilation in response to changes in oxygen and carbon dioxide levels. As vascular resistance decreases, stroke volume increases, maintaining blood pressure. A high cardiac output becomes "high output failure" when blood pressure cannot be maintained against low systemic vascular resistance, or oxygen delivery is insufficient. The diagnostic triad is high cardiac output, low blood pressure, and very low systemic vascular resistance. Treatment focuses on balancing oxygen delivery and demand by optimizing preload, contractility, and afterload through fluid administration and inotropic support tailored to individual hemodynamic parameters.Monitoring Hypoxia and oxygen supplementation
Monitoring Hypoxia and oxygen supplementationYouttam Laudari
Ěý
1) Hypoxia can lead to decreased ATP synthesis, lactic acidosis, impaired protein synthesis, and irreversible cell changes due to increased cytosolic calcium.
2) Pao2, Sao2, and oxygen content are important measures of oxygen levels in the blood. Pulse oximetry can monitor Sao2 non-invasively but has limitations.
3) Arterial blood gas analysis precisely measures oxygen, carbon dioxide, pH, and bicarbonate levels to assess oxygenation and ventilation.Hypoxia today
Hypoxia todayYouttam Laudari
Ěý
1) Hypoxia can lead to decreased ATP synthesis, lactic acidosis, impaired protein synthesis, and irreversible cell changes due to increased cytosolic calcium.
2) Pao2, Sao2, and oxygen content are important measures of oxygen levels in the blood. Pulse oximetry can monitor Sao2 non-invasively but has limitations.
3) Arterial blood gas analysis precisely measures oxygen, carbon dioxide, pH, bicarbonate, and base excess levels to evaluate oxygenation and ventilation.Acute resp failure.pptx
Acute resp failure.pptxDipali Dumbre
Ěý
This document discusses gas exchange and respiratory failure. It defines hypoxemic respiratory failure as inadequate oxygen transfer resulting in low arterial oxygen levels, and hypercapnic respiratory failure as insufficient carbon dioxide removal leading to high arterial carbon dioxide levels. The major mechanisms of hypoxemic failure are ventilation-perfusion mismatching, shunting, diffusion limitation, and hypoventilation, while hypercapnic failure results from an imbalance between ventilatory supply and demand. Diseases like pneumonia, pulmonary edema, and COPD can cause either type of respiratory failure through various pathophysiological mechanisms.More from Dr. Abhinav Agarwal (9)
Ebstein Anomaly
Ebstein AnomalyDr. Abhinav Agarwal
Ěý
The document discusses congenital heart defects, particularly focusing on conditions like Ebstein's anomaly, which affects <1% of patients and shows a prevalence of 2.4/10,000. It outlines associated symptoms, genetic factors, treatment options, and long-term prognosis, including survival rates and likelihood of reoperation. Key management strategies for affected patients include various surgical interventions and considerations for arrhythmias.Pah management
Pah managementDr. Abhinav Agarwal
Ěý
This document summarizes key information about pulmonary hypertension (PH) management including: median survival rates; clinical presentation; diagnostic testing including echocardiogram, right heart catheterization, and biomarkers; risk assessment; and therapy. Median survival is 2.8 years for adults and 10 months for pediatric patients with PH. Clinical presentation includes symptoms of exertional shortness of breath, fatigue, and right ventricular failure. Diagnostic testing is aimed at confirming the diagnosis, assessing severity, and identifying the cause of PH. Risk assessment evaluates factors like functional capacity, right ventricular function, and complications to determine low, intermediate, or high risk status. Therapy involves general measures, PH-specific drug therapy, and interventional procedures in advanced cases.Pediatric Obesity
Pediatric ObesityDr. Abhinav Agarwal
Ěý
The document discusses childhood obesity, its definitions, and classification, highlighting that obesity rates in children globally have risen significantly, particularly in developing countries like India. It outlines epidemiology, risk factors, pathophysiology, evaluations, management strategies, and prevention techniques, while also referencing the WHO's initiative to address the issue. The need for multidisciplinary approaches, including dietary changes, physical activity, and potential pharmacological or surgical interventions, is emphasized to combat this growing health concern.Diabetic Ketoacidosis
Diabetic KetoacidosisDr. Abhinav Agarwal
Ěý
The document outlines a management protocol for diabetic ketoacidosis (DKA) in children, detailing presentation symptoms, diagnostic criteria, severity classification, and step-by-step treatment guidelines. Key management practices include fluid resuscitation, electrolytes monitoring, insulin therapy, and careful monitoring of vital signs and laboratory values. Emergency interventions and fluid management strategies are emphasized, with specific protocols for potassium and bicarbonate supplementation.Abga
AbgaDr. Abhinav Agarwal
Ěý
The document discusses acid-base disorders, including normal (mixed) acidemia, primary and secondary metabolic acidosis/alkalosis, and compensatory responses by the body. Key formulas for calculating expected values and identifying different disorders are provided, highlighting the importance of compensation while noting that the body never overcompensates. It emphasizes that renal compensatory responses are slow, occurring over 2 to 4 days.Chronic liver disease
Chronic liver diseaseDr. Abhinav Agarwal
Ěý
The document provides an overview of chronic liver disease (CLD), including its definition, major causes (viral, autoimmune, metabolic, and drug-induced), and clinical manifestations. It discusses diagnostic methods, treatment options, and management strategies for conditions such as hepatitis B and C, autoimmune hepatitis, and Wilson's disease. Additionally, it covers the complexities of portal hypertension and the importance of early intervention in preventing progression of liver disease.Apparent life threatening event
Apparent life threatening eventDr. Abhinav Agarwal
Ěý
The document discusses apparent life-threatening events (ALTE) in infants, defining the condition, its epidemiology, clinical presentations, risk factors, and evaluations involved. It highlights that ALTE events can arise from various benign conditions and outlines diagnostic dilemmas and necessary investigations for accurate assessment. Additionally, guidelines on monitoring and caregiver education to prevent further episodes are provided.Ebola virus
Ebola virusDr. Abhinav Agarwal
Ěý
The document provides a comprehensive overview of Ebola Virus Disease (EVD), covering aspects such as its transmission, pathogenesis, clinical features, diagnosis, case definitions, management, and prevention strategies. It highlights the high case fatality rates associated with EVD and outlines the risks of infection, particularly related to handling infected animals and during human interactions. The document also discusses the importance of healthcare precautions, accidental exposure protocols, and summarizes findings from EVD outbreaks in West Africa.Ambiguous Genitalia
Ambiguous GenitaliaDr. Abhinav Agarwal
Ěý
The clinical case presentation involves an early preterm infant with ambiguous genitalia including an underdeveloped scrotum and hypospadias. Examination of the elder sibling also revealed ambiguous genitalia. Initial investigations showed normal hormone levels. The differential diagnoses considered included congenital adrenal hyperplasia, androgen insensitivity syndrome, and 5-alpha reductase deficiency. Further evaluation of the elder sibling confirmed a diagnosis of 5-alpha reductase deficiency based on a poor response to hCG stimulation testing. The case highlights the approach to evaluating infants with disorders of sex development.Ad
Recently uploaded (20)
transpersonal therapy in india Best spiritual healer in delhi.pdf
transpersonal therapy in india Best spiritual healer in delhi.pdfmarketing877802
Ěý
Welcome to the Life Healer Clinic, where profound healing meets transformative journeys. As the best spiritual healer in India and home to the finest Past Life Regression Therapy therapists, we are dedicated to guiding you towards holistic well-being. Our expert practitioners blend ancient wisdom with modern techniques, providing personalized and effective solutions for emotional liberation, stress reduction, and spiritual connection. Embark on a transformative odyssey with us at Life Healer Clinic, where healing isn't just a process but a way of life.Dengue Epidemiology_Intersectoral Response_Dr Pankaj Singh.pptx
Dengue Epidemiology_Intersectoral Response_Dr Pankaj Singh.pptxpanpunpra
Ěý
Basic Information on Dengue Epidemiology and role of Important Stakeholder/Departments in Mitigation & Response to Dengue Errors that Could be Deemed Fraudulent in Ambulance Billing.pptx
Errors that Could be Deemed Fraudulent in Ambulance Billing.pptxjohnbutlermbc
Ěý
Ambulance Billing could be replete with errors that could end up in being a fraudulent case. Know how to ensure correct billing.
Common Medical Billing Errors.pppptttttx
Common Medical Billing Errors.pppptttttxjohnbutlermbc
Ěý
Explaining how Common Medical Billing Errors could be costing you revenue loss, and how Medical Billers and Coders can help you to reduce it.
ULCERS, SINUSES & FISTULAE in surgery ward.ppt
ULCERS, SINUSES & FISTULAE in surgery ward.pptSholayMeiteiKangjam
Ěý
ulcers, sinuses and fistulae in surgery wardHISTORY OF CLINICAL PSYCHOLOGY, History of Clinical Psychology across word to...
HISTORY OF CLINICAL PSYCHOLOGY, History of Clinical Psychology across word to...LakeshSahu3
Ěý
History of Clinical Psychology including the history of Psychology in Indian and Status of Psychology in IndiaPublic-Private Partnerships in Healthcare_ A Sustainable Model for African Na...
Public-Private Partnerships in Healthcare_ A Sustainable Model for African Na...oliverwanyama96
Ěý
Across Africa, healthcare systems are under increasing pressure from rising populations, chronic underfunding, and infrastructure gaps that limit access to quality care. In response, Public-Private Partnerships (PPPs) are gaining momentum as a sustainable model to deliver healthcare infrastructure, services, and innovation.
Dengue Basic Information_Mitigation & Response_Dr. Pankaj Singh
Dengue Basic Information_Mitigation & Response_Dr. Pankaj Singhpanpunpra
Ěý
Dengue Basic Information_Mitigation & Response_Dr. Pankaj SinghPersonalized Autism Therapies: Where Are We Currently?
Personalized Autism Therapies: Where Are We Currently?Advancells: Stem Cell Lab and Research
Ěý
Autism, a neurodevelopmental disorder affecting social communication and behavior, impacts approximately 61.8 million people worldwide. Each patient exhibits unique symptoms and needs, emphasizing the importance of tailored treatment strategies. Explore the growing scientific interest in personalized approaches and the promising role of regenerative medicine in autism treatment. Discover how customized strategies are shaping the future of neurodevelopmental disorder care.Exploring Technological Advancements in Bioresorbable Vascular Scaffolds for ...
Exploring Technological Advancements in Bioresorbable Vascular Scaffolds for ...ganeshdukare428
Ěý
Introduction: The Emergence of Bioresorbable Solutions in Cardiovascular Care
Cardiovascular disease remains the leading cause of death worldwide, and with growing awareness, technological innovation has become the backbone of modern cardiology. One such innovation making significant strides is the bioresorbable vascular scaffold (BVS) — a next-generation alternative to traditional metallic stents used in the treatment of coronary artery disease (CAD). Designed to temporarily support the vessel and gradually dissolve, BVS devices restore natural vessel function without leaving a permanent implant.
Technological progress has been instrumental in addressing early challenges associated with these scaffolds, such as limited radial strength and late thrombosis. This article delves into the cutting-edge advancements transforming BVS and how these developments are improving patient outcomes and expanding clinical adoption.
The global bioresorbable vascular scaffold market size is estimated to be valued at US$ 592.8 Million by 2032 from US$ 314.4 Million in 2025. It is expected to register a CAGR of 8.3% in the forecast period between 2025 and 2032.
Shamis Tate Shares 5 Essential Brain Health Tips.pdf
Shamis Tate Shares 5 Essential Brain Health Tips.pdfShamis Tate
Ěý
Neurologist Shamis Tate shares 5 simple and effective brain health tips. Learn how good sleep, healthy food, staying active, using your mind, and connecting with others can help keep your brain strong, sharp, and healthy. Easy steps that anyone can follow to feel better and think clearer every day.Trending-Now_-Ayurvedic-Bone-Regeneration-Therapies-for-AVN-_2025_.ppt
Trending-Now_-Ayurvedic-Bone-Regeneration-Therapies-for-AVN-_2025_.pptkhephioisols
Ěý
Discover how Ayurvedic therapies in 2025 offer non-invasive, holistic solutions for avascular necrosis (AVN), promoting bone regeneration and improved mobilityMCH (MATERNAL AND CHILD HEALTH) HEALTH Programmes
MCH (MATERNAL AND CHILD HEALTH) HEALTH ProgrammesDr. Mamta Gehlawat
Ěý
A glimpse of some important existing MCH related programmes and schemes for 3rd year MBBS studentsIsothermal Assays and their applications
Isothermal Assays and their applicationsArchanaPrakash23
Ěý
Nucleic acid amplification Techniques other then PCR and their applicationsDeep Vein Thrombosis Treatment in East Brunswick, NJ
Deep Vein Thrombosis Treatment in East Brunswick, NJVein & Vascular Medicine Clinic
Ěý
Deep Vein Thrombosis (DVT) is a serious condition that often develops silently, especially after long periods of immobility. This blog explores the common symptoms—like leg swelling, tenderness, and warmth—and explains when to seek medical help to prevent life-threatening complications like pulmonary embolism. Learn how to recognize early warning signs and reduce your risk through simple lifestyle changes.
Radiological diagnosis of Gastric carcinoma
Radiological diagnosis of Gastric carcinomaabid hossain
Ěý
radiological presentation of stages of gastric cancer , different modalities to identify and doagnose them Revision Total Hip Replacement (THR): Surgical Principles, Techniques, and Bo...
Revision Total Hip Replacement (THR): Surgical Principles, Techniques, and Bo...Dr. Prabhat Pandey
Ěý
Revision Total Hip Replacement (THR) is among the most demanding procedures in orthopedic surgery. Unlike primary THR, it involves addressing pre-existing complications such as implant failure, dislocation, bone loss, or infection, often in the presence of compromised soft tissues and bone quality. While primary THR offers high success rates and reproducible outcomes, revision THR requires greater surgical expertise, meticulous planning, and personalized execution to restore function and minimize complications.
This presentation by Dr. Prabhat Pandey is designed as a comprehensive resource for orthopedic surgeons, residents, and joint reconstruction teams who seek to understand and master the essential principles, decision-making algorithms, and advanced techniques used in revision THR.
Revision hip arthroplasty is associated with:
Increased operative time and blood loss
Higher complication rates: infection, dislocation, thromboembolism, nerve injury, and periprosthetic fracture
The need to manage weakened bone stock and soft tissue envelope
Difficulty in removing failed implants, including intramedullary components.
Revision surgery is warranted in cases of:
Prosthetic dislocation or instability
Mechanical loosening of components
Implant wear or breakage
Periprosthetic fracture
Deep infection
Osteolysis or bone resorption
Painful loosening without overt signs of mechanical failure
Each case demands tailored intervention based on the severity and combination of these factors.
3. Principles of Successful Revision THR
Safe removal of loose or failed components
Preservation of host bone and soft tissue integrity
Effective reconstruction of bone defects using bone grafts or metal augments
Achieving stability of the revision components
Restoration of biomechanics, particularly the anatomical center of rotation.
Dislocation rates:
0.3–10% in primary THR
Up to 28% in revision THR
Influencing Factors:
Surgical approach
Abductor muscle function
Component malpositioning
Patient compliance
Prosthesis longevity
Underlying diagnosis (e.g., hip fracture, neuromuscular disorder
Revision Total Hip Replacement is not merely a technical endeavor—it is a test of surgical judgment, experience, and adaptability. Successful outcomes hinge on:
Thorough preoperative assessment
Judicious use of classification systems like Paprosky
Proficiency in implant removal
Skillful reconstruction of defects
Meticulous postoperative care
This presentation distills the complex decision-making process into an organized, practical guide for any surgeon facing the challenge of revision THR.
Understanding Surgical Approaches and Their Risks
Dislocation Types and Management
Preoperative Planning Essentials
Surgical Options for Instability and Revision
Operative Exposure and Implant Removal
Techniques for Removing Cemented Implants
Cementless Implant Removal
Managing Bone Deficiency in the Acetabulum
Paprosky Classification: Detailed Breakdown
PPT Anticancer agent for B Pharm Fifth Semester students
PPT Anticancer agent for B Pharm Fifth Semester studentsDinesh Kawade
Ěý
Anti-neoplastic agents:
Alkylating agents: Meclorethamine*, Cyclophosphamide, Melphalan,Chlorambucil, Busulfan, Thiotepa
Antimetabolites: Mercaptopurine*, Thioguanine, Fluorouracil, Floxuridine, Cytarabine, Methotrexate*, Azathioprine
Antibiotics: Dactinomycin, Daunorubicin, Doxorubicin, Bleomycin
Plant products: Etoposide, Vinblastin sulphate, Vincristin sulphate
Miscellaneous: Cisplatin, Mitotane.
Revision Total Hip Replacement (THR): Surgical Principles, Techniques, and Bo...
Revision Total Hip Replacement (THR): Surgical Principles, Techniques, and Bo...Dr. Prabhat Pandey
Ěý
Ad
Univentricular circulation
- 2.  Cardiac output affected by  Preload  Afterload  Rate  Rhythm  Contractility  AP shunts  Regional Resistance  Neurohumoral Factors (Inflammation, sympathetic nervous system)  Local Factors (Autoregulation)
- 3.  Redistribute Blood flow to brain and heart  Mesentric and splanchnic circulation- silent ischemia during compensated shock  Baroreflex - Contractility, HR, SVR & decreases venous capacitance  Often body impairs systemic flow in face of myocardial dysfunction (regional ischaemia due to high SVR)  Ischaemic organ damage can occur even in presence of normal global oxygen economy  Regional Ischaemia →MODS→Death
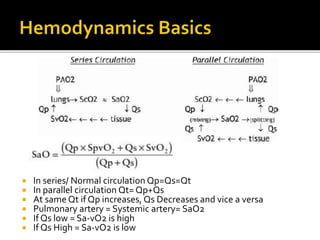
- 4.  In series/ Normal circulation Qp=Qs=Qt  In parallel circulation Qt= Qp+Qs  At same Qt if Qp increases, Qs Decreases and vice a versa  Pulmonary artery = Systemic artery= SaO2  If Qs low = Sa-vO2 is high  If Qs High = Sa-vO2 is low
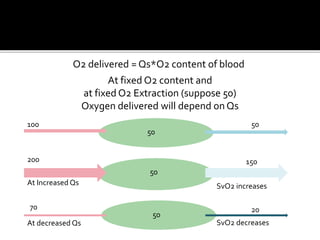
- 5. 200 At Increased Qs At decreased Qs 150 2070 50 50 100 50 50 SvO2 decreases SvO2 increases O2 delivered = Qs*O2 content of blood At fixed O2 content and at fixed O2 Extraction (suppose 50) Oxygen delivered will depend on Qs
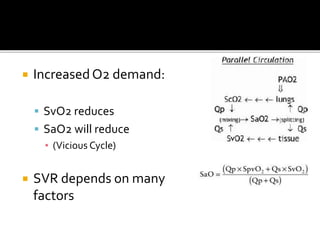
- 6.  Increased O2 demand:  SvO2 reduces  SaO2 will reduce ▪ (Vicious Cycle)  SVR depends on many factors
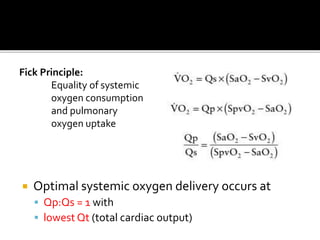
- 7.  Optimal systemic oxygen delivery occurs at  Qp:Qs = 1 with  lowest Qt (total cardiac output) Fick Principle: Equality of systemic oxygen consumption and pulmonary oxygen uptake
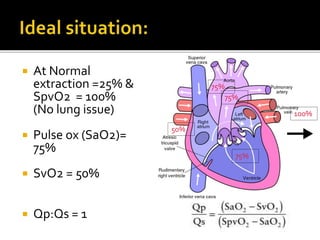
- 8.  At Normal extraction =25% & SpvO2 = 100% (No lung issue)  Pulse ox (SaO2)= 75%  SvO2 = 50%  Qp:Qs = 1 75% 75% 75% 50% 100%
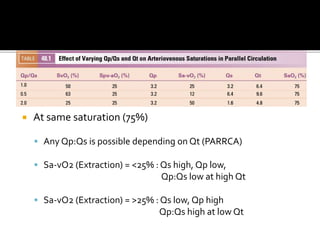
- 9.  At same saturation (75%)  Any Qp:Qs is possible depending on Qt (PARRCA)  Sa-vO2 (Extraction) = <25% : Qs high, Qp low, Qp:Qs low at high Qt  Sa-vO2 (Extraction) = >25% : Qs low, Qp high Qp:Qs high at low Qt
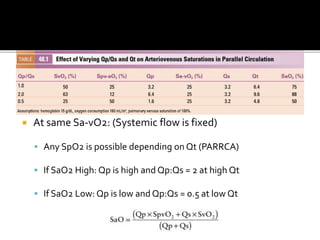
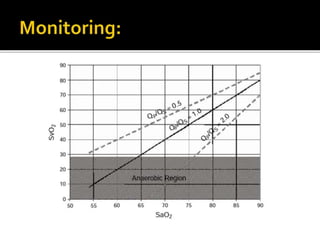
- 10.  At same Sa-vO2: (Systemic flow is fixed)  Any SpO2 is possible depending on Qt (PARRCA)  If SaO2 High: Qp is high and Qp:Qs = 2 at high Qt  If SaO2 Low: Qp is low and Qp:Qs = 0.5 at low Qt
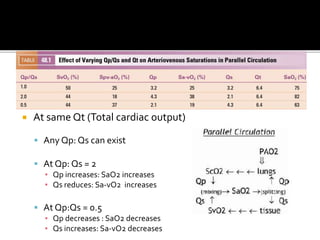
- 11.  At same Qt (Total cardiac output)  Any Qp: Qs can exist  At Qp: Qs = 2 ▪ Qp increases: SaO2 increases ▪ Qs reduces: Sa-vO2 increases  At Qp:Qs = 0.5 ▪ Qp decreases : SaO2 decreases ▪ Qs increases: Sa-vO2 decreases
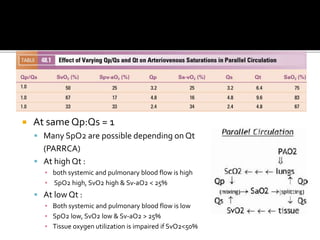
- 12.  At same Qp:Qs = 1  Many SpO2 are possible depending on Qt (PARRCA)  At high Qt : ▪ both systemic and pulmonary blood flow is high ▪ SpO2 high, SvO2 high & Sv-aO2 < 25%  At low Qt : ▪ Both systemic and pulmonary blood flow is low ▪ SpO2 low, SvO2 low & Sv-aO2 > 25% ▪ Tissue oxygen utilization is impaired if SvO2<50%
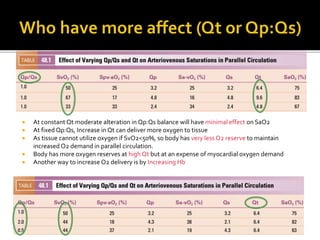
- 13.  At constant Qt moderate alteration in Qp:Qs balance will have minimal effect on SaO2  At fixed Qp:Qs, Increase in Qt can deliver more oxygen to tissue  As tissue cannot utilize oxygen if SvO2<50%, so body has very less O2 reserve to maintain increased O2 demand in parallel circulation.  Body has more oxygen reserves at high Qt but at an expense of myocardial oxygen demand  Another way to increase O2 delivery is by Increasing Hb
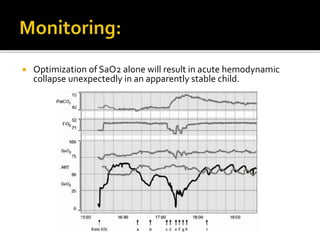
- 15.  Optimization of SaO2 alone will result in acute hemodynamic collapse unexpectedly in an apparently stable child.
- 16.  Gas manipulation of PVR  Inspired CO2: Increased PVR, decreased SVR, Increased O2 delivery (esp. brain)  Subatmospheric FiO2: Raises PVR  Controlled PPV while avoiding hypervenilation (PEEP)  O2 can be used if:  Respiratory pathology is present  Restrictive communications  Control of elevated SVR was more effective than increasing PVR  Inotropes increase SVR at high doses  Inodilators preferred (while preventing significant hypotension)  Morphine reduces Sympathetic outflow  Regional saturations of brain, liver, kidney, gut and muscle can be measured to rule out regional ischaemia  Increase Hct > 50% increases O2 carrying capacity
- 17.  Pulmonary venous SpvO2 = 100%  Variablity in Arteriovenous saturation difference  Not possible to obtain true sytemic venous mixed venous saturation
- 18.  Thank you