












Vein of galen malformation
- 1. VEIN OF GALEN MALFORMATION
- 2. ŌĆó PRESENTATION ŌĆó AS CCF IN THE FIRST WEEK OF LIFE AND HAVE POOR PROGNOSIS
- 3. VEIN OF GALEN ŌĆó The congenital malformation develops during weeks 6-11 of fetal development as a persistent embryonic prosencephalic vein of Markowski thus, VGAM is actually a misnomer. ŌĆó The vein of Markowski actually drains into the vein of Galen.
- 4. ŌĆó It can produce hydrocephalus if it obstructs the sylvian aqueduct
- 7. ŌĆó True VOG ARE FED FROM ŌĆō ANTERIOR CHOROIDAL ŌĆō MEDIAL AND LATERAL CHOROIDAL ŌĆō MESENCEPHALIC ŌĆō PERICALLOSAL VESSELS
- 8. TYPES OF VEIN OF GALEN MALFORMATION ŌĆó PURE INTERNAL FISTULA ŌĆó ŌĆś ŌĆó FISTULA BETWEEN THALAMOPERFORATORS AND VEIN OF GALEN ŌĆó MIXED FORM(MOST COMMON TYPE) ŌĆó PLEXIFORM TYPE
- 9. CLINICAL FEATURES ŌĆó RESPIRATORY DISTRESS ŌĆó REFUSAL OF FEED ŌĆó HYDROCEPHALUS ŌĆō SUNSET SIGN ŌĆó CYANOSIS ŌĆó SEIZURES
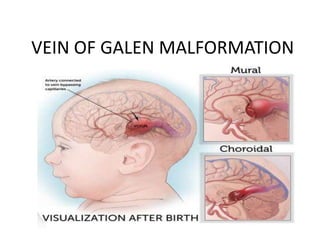
- 10. CLASSIFICATION ŌĆó LASJAUNIAS CLASSIFICATION ŌĆō CHOROIDAL ŌĆō MURAL
- 11. CLASSIFICATION ŌĆó YASARGILL CLASSIFICATION ŌĆó TYPE I ŌĆō PURE CISTERNAL CONNECTION BETWEEN VOG AND PERICALLOSAL / POSTERIOR CEREBRAL ŌĆó TYPE II - MULTIPLE FISTULUS CONNECTION BETWEEN THALAMOPERFORATORS AND VOG
- 12. ŌĆó TYPE III ŌĆō HIGH FLOW MIXED TYPE I AND TYPE II TYPE IV PARENCHYMAL AVM WITH DRAINAGE
- 14. TREATMENT ŌĆó OPTION COMPRISES OF ŌĆō EMBOLIZATION ŌĆō RESECTION ŌĆō RADIOSURGERY