2. o Weaning from mechanical ventilation is the process of reducing ventilatory
support, ultimately resulting in a patient breathing spontaneously and being
extubated.
o This process can be achieved rapidly in 80% of patients when the original cause
of the respiratory failure has improved.
3. 3
o Weaning in progress is an intermediate category (between weaning success
and weaning failure) for patients who are extubated but continue to receive
ventilatory support by noninvasive ventilation (NIV)
o Weaning success is defined as absence of ventilatory support 48 hours
following the extubation
o Weaning failure is defined as either the failure of spontaneous breathing trial
(SBT) or the need for reintubation within 48 hours following extubation.
o Patients who fail the SBT exhibit clinical signs:
o tachypnea, tachycardia, hypertension, hypotension, hypoxemia,
acidosis, or arrhythmias.
o Physical signs of SBT failure may include :
o agitation, distress, diminished mental status, diaphoresis and
increased work of breathing
4. 4
o Factors associated with successful weaning
(i) has the underlying condition improved?
(ii) is the patientĪ»s general condition optimal?
(iii) have potential airway problems been identified and
remedied? (iv) is breathing adequate?
5. I) Has the underlying condition improved?
o cause of their respiratory failure has to be resolved to a reasonable level.
II) General optimization :
o Patients who are re-intubated in general have worse outcomes.
o Common causes of weaning failure are:
1. Central drive :
reduced by: Sedatives,
Direct insults to the respiratory centre
Metabolic alkalosis (commonly exacerbated by
hypokalaemia) Loss of hypoxic drive (COPD)
9. 9
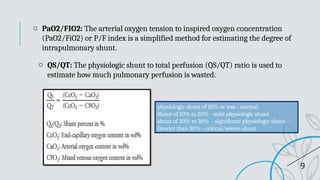
o PaO2/FIO2: The arterial oxygen tension to inspired oxygen concentration
(PaO2/FiO2) or P/F index is a simplified method for estimating the degree of
intrapulmonary shunt.
o QS/QT: The physiologic shunt to total perfusion (QS/QT) ratio is used to
estimate how much pulmonary perfusion is wasted.
physiologic shunt of 10% or less - normal.
Shunt of 10% to 20% - mild physiologic shunt
shunt of 20% to 30% - significant physiologic shunt.
Greater than 30% - critical/severe shunt
10. III) Airway problems resolved or not
o the artificial airway needs to be removed.
o Good upper airway reflexes, including an adequate cough and minimal secretions.
o An adequate conscious level is required for airway maintenance after extubation.
o Airway (particularly laryngeal) oedema may be a cause of difficulty in breathing after
extubation.
risk factors : traumatic or difficult intubation,
history of self extubation, overinflated tracheal
tube cuff intubation for extended
periods.
o The ability to breathe around a deflated endotracheal tube cuff, or cuff leak >130 ml
during volume cycled ventilation - to predict an adequate airway diameter.
o In those patients at risk, corticosteroids can be used
o Post-extubation stridor may be ameliorated by epinephrine nebulizers
11. 11
General preconditions for commencement of weaning:
o Reversal of primary problem causing need for ventilation
o Patient awake and responsive
o Good analgesia, ability to cough
o Reducing or minimal doses of inotropic support
o IdeallyĪ¬functioning bowels, absence of abdominal distension
o Normalizing metabolic status
o Adequate hemoglobin concentration
12. 14
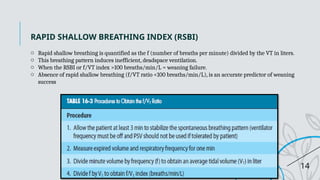
RAPID SHALLOW BREATHING INDEX (RSBI)
o Rapid shallow breathing is quantified as the f (number of breaths per minute) divided by the VT in liters.
o This breathing pattern induces inefficient, deadspace ventilation.
o When the RSBI or f/VT index >100 breaths/min/L = weaning failure.
o Absence of rapid shallow breathing (f/VT ratio <100 breaths/min/L), is an accurate predictor of weaning
success
13. 15
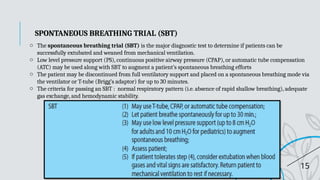
o The spontaneous breathing trial (SBT) is the major diagnostic test to determine if patients can be
successfully extubated and weaned from mechanical ventilation.
o Low level pressure support (PS), continuous positive airway pressure (CPAP), or automatic tube compensation
(ATC) may be used along with SBT to augment a patientĪ»s spontaneous breathing efforts
o The patient may be discontinued from full ventilatory support and placed on a spontaneous breathing mode via
the ventilator or T-tube (BriggĪ»s adaptor) for up to 30 minutes.
o The criteria for passing an SBT : normal respiratory pattern (i.e. absence of rapid shallow breathing), adequate
gas exchange, and hemodynamic stability.
SPONTANEOUS BREATHING TRIAL (SBT)
14. 16
Patients failing the spontaneous breathing trial
The ventilatory choices for these patients include the following:
(i) T-piece trials
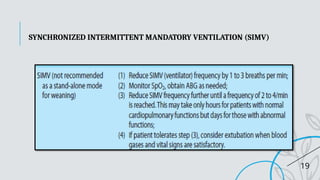
(ii) synchronized intermittent mandatory ventilation (SIMV)
(iii) pressure support ventilation (PSV).
15. 17
PRESSURE SUPPORT VENTILATION
Weaning with PSV is done by starting the pressure support level at 5 to 15 cmH2O and
adjusting it gradually (up to 40 cm H2O) until a desired spontaneous VT (10 to 15 mL/kg) is
obtained
16. 18
AUTOMATIC TUBE COMPENSATION.
o Automatic tube compensation (ATC) is a mode in the Evita 4 ventilator (Dr?ger Medical) that reduces
the airflow resistance imposed by artificial airway (endotracheal or tracheostomy tube).
o It allows the patient to have a breathing pattern as if breathing spontaneously without an artificial
airway
o This type of compensation may facilitate breathing efficacy and reduce the work of breathing
throughout the weaning process.
18. 20
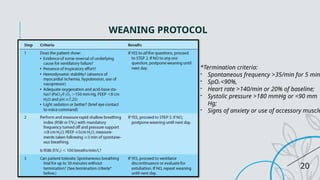
WEANING PROTOCOL
*Termination criteria:
- Spontaneous frequency >35/min for 5 min
- SpO2 <90%,
- Heart rate >140/min or 20% of baseline;
- Systolic pressure >180 mmHg or <90 mm
Hg;
- Signs of anxiety or use of accessory muscle
19. 21
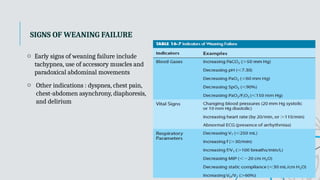
SIGNS OF WEANING FAILURE
o Early signs of weaning failure include
tachypnea, use of accessory muscles and
paradoxical abdominal movements
o Other indications : dyspnea, chest pain,
chest-abdomen asynchrony, diaphoresis,
and delirium
20. 22
TERMINAL WEANING
o Terminal weaning is defined as withdrawal of mechanical ventilation that results in the death
of a patient
o four concerns must be evaluated and discussed, where appropriate, with the patient and family
members: (1) patientĪ»s informed request, (2) medical futility, (3) reduction of pain and
suffering, and (4) fear and distress
o Analgesics and sedatives should be provided in sufficient quantity for patient comfort and
relief of anxiety.
o The ventilator settings may be adjusted to provide minimal support