Yellowregistrationform
âĒ
0 likesâĒ88 views

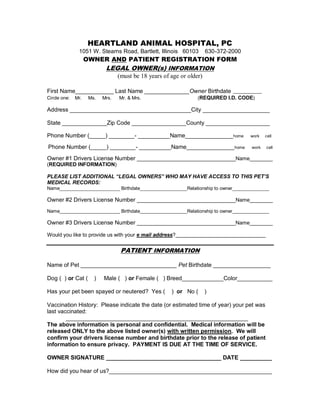
This document is an owner and patient registration form for Heartland Animal Hospital. It requests information such as the legal owner's name, address, phone number, driver's license number and date of birth. It also requests the pet's name, date of birth, sex, breed, color, spay/neuter status and vaccination history. The form states that medical information will only be released to listed owners after confirming their identity with a driver's license and birthdate, and that payment is due at the time of service.
Yellowregistrationform
- 1. HEARTLAND ANIMAL HOSPITAL, PC 1051 W. Stearns Road, Bartlett, Illinois 60103 630-372-2000 OWNER AND PATIENT REGISTRATION FORM LEGAL OWNER(s) INFORMATION (must be 18 years of age or older) First Name____________ Last Name ______________Owner Birthdate __________ Circle one: Mr. Ms. Mrs. Mr. & Mrs. (REQUIRED I.D. CODE) Address ______________________________________City _____________________ State ______________Zip Code _________________County ____________________ Phone Number (_____) ________- __________Name_______________ home Phone Number (_____) ________- __________Name_______________ home work cell work cell Owner #1 Drivers License Number __________________________________Name________ (REQUIRED INFORMATION) PLEASE LIST ADDITIONAL âLEGAL OWNERSâ WHO MAY HAVE ACCESS TO THIS PETâS MEDICAL RECORDS: Name_______________________ Birthdate__________________Relationship to owner______________ Owner #2 Drivers License Number __________________________________Name________ Name_______________________ Birthdate__________________Relationship to owner______________ Owner #3 Drivers License Number __________________________________Name________ Would you like to provide us with your e mail address?_______________________________ PATIENT INFORMATION Name of Pet ______________________________ Pet Birthdate __________________ Dog ( ) or Cat ( ) Male ( ) or Female ( ) Breed_____________Color___________ Has your pet been spayed or neutered? Yes ( ) or No ( ) Vaccination History: Please indicate the date (or estimated time of year) your pet was last vaccinated: _________________________________________________________ The above information is personal and confidential. Medical information will be released ONLY to the above listed owner(s) with written permission. We will confirm your drivers license number and birthdate prior to the release of patient information to ensure privacy. PAYMENT IS DUE AT THE TIME OF SERVICE. OWNER SIGNATURE ____________________________________ DATE __________ How did you hear of us?___________________________________________________