

Ch 17 lecture_outline
- 1. 17 Blood
- 2. Blood Composition Blood: a fluid connective tissue composed of Plasma Formed elements Erythrocytes (red blood cells, or RBCs) Leukocytes (white blood cells, or WBCs) Platelets
- 3. Blood Composition Hematocrit Percent of blood volume that is RBCs 47% Âą 5% for males 42% Âą 5% for females
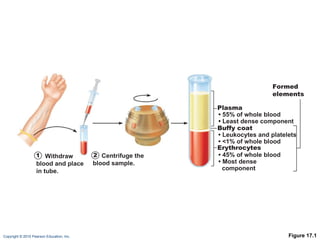
- 4. Figure 17.1 1 Withdraw blood and place in tube. 2 Centrifuge the blood sample. Plasma âĒ 55% of whole blood âĒ Least dense component Buffy coat âĒ Leukocytes and platelets âĒ <1% of whole blood Erythrocytes âĒ 45% of whole blood âĒ Most dense component Formed elements
- 5. Physical Characteristics and Volume Sticky, opaque fluid Color scarlet to dark red pH 7.35â7.45 38 ï° C ~8% of body weight Average volume: 5â6 L for males, and 4â5 LĖýfor females
- 6. Functions of Blood Distribution of O 2 and nutrients to body cells Metabolic wastes to the lungs and kidneys for elimination Hormones from endocrine organs to target organs
- 7. Functions of Blood Regulation of Body temperature by absorbing and distributing heat Normal pH using buffers Adequate fluid volume in the circulatory system
- 8. Functions of Blood Protection against Blood loss Plasma proteins and platelets initiate clot formation Infection Antibodies Complement proteins WBCs defend against foreign invaders
- 9. Blood Plasma 90% water Proteins are mostly produced by the liver 60% albumin 36% globulins 4% fibrinogen
- 10. Blood Plasma Nitrogenous by-products of metabolismâlactic acid, urea, creatinine Nutrientsâglucose, carbohydrates, amino acids ElectrolytesâNa + , K + , Ca 2+ , Cl â , HCO 3 â Respiratory gasesâO 2 and CO 2 Hormones
- 11. Formed Elements Only WBCs are complete cells RBCs have no nuclei or organelles Platelets are cell fragments Most formed elements survive in the bloodstream for only a few days Most blood cells originate in bone marrow and do not divide
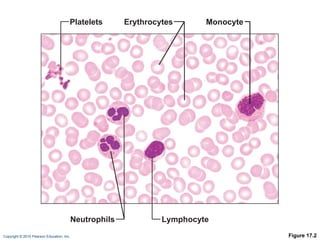
- 12. Figure 17.2 Platelets Neutrophils Lymphocyte Erythrocytes Monocyte
- 13. Erythrocytes Biconcave discs, anucleate, essentially no organelles Filled with hemoglobin (Hb) for gas transport Contain the plasma membrane protein spectrin and other proteins Provide flexibility to change shape as necessary Are the major factor contributing to blood viscosity
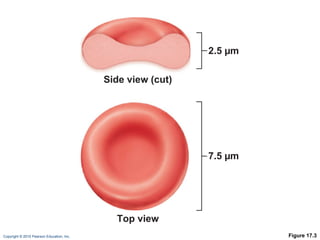
- 14. Figure 17.3 2.5 Âĩm 7.5 Âĩm Side view (cut) Top view
- 15. Erythrocytes Structural characteristics contribute to gas transport Biconcave shapeâhuge surface area relative to volume >97% hemoglobin (not counting water) No mitochondria; ATP production is anaerobic; no O 2 is used in generation of ATP A superb example of complementarity of structure and function!
- 16. Erythrocyte Function RBCs are dedicated to respiratory gas transport Hemoglobin binds reversibly with oxygen
- 17. Erythrocyte Function Hemoglobin structure Protein globin: two alpha and two beta chains Heme pigment bonded to each globin chain Iron atom in each heme can bind to one O 2 molecule Each Hb molecule can transport four O 2
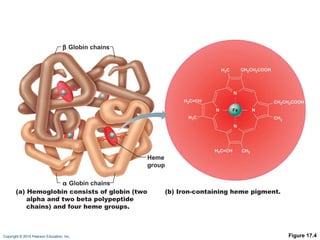
- 18. Figure 17.4 Heme group (a) Hemoglobin consists of globin (two alpha and two beta polypeptide chains) and four heme groups. (b) Iron-containing heme pigment. ïĄ Globin chains ïĒ Globin chains
- 19. Hemoglobin (Hb) O 2 loading in the lungs Produces oxyhemoglobin (ruby red) O 2 unloading in the tissues Produces deoxyhemoglobin or reduced hemoglobin (dark red) CO 2 loading in the tissues Produces carbaminohemoglobin (carries 20% of CO 2 in the blood)
- 20. Hematopoiesis Hematopoiesis (hemopoiesis): blood cell formation Occurs in red bone marrow of axial skeleton, girdles and proximal epiphyses of humerus and femur
- 21. Hematopoiesis Hemocytoblasts (hematopoietic stem cells) Give rise to all formed elements Hormones and growth factors push the cell toward a specific pathway of blood cell development New blood cells enter blood sinusoids
- 22. Erythropoiesis Erythropoiesis: red blood cell production A hemocytoblast is transformed into a proerythroblast Proerythroblasts develop into early erythroblasts
- 23. Erythropoiesis Phases in development Ribosome synthesis Hemoglobin accumulation Ejection of the nucleus and formation of reticulocytes Reticulocytes then become mature erythrocytes
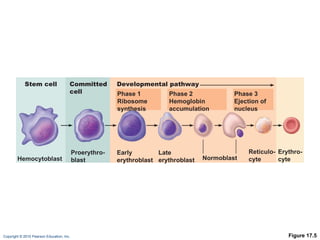
- 24. Figure 17.5 Stem cell Hemocytoblast Proerythro- blast Early erythroblast Late erythroblast Normoblast Phase 1 Ribosome synthesis Phase 2 Hemoglobin accumulation Phase 3 Ejection of nucleus Reticulo- cyte Erythro- cyte Committed cell Developmental pathway
- 25. Regulation of Erythropoiesis Too few RBCs leads to tissue hypoxia Too many RBCs increases blood viscosity Balance between RBC production and destruction depends on Hormonal controls Adequate supplies of iron, amino acids, and B vitamins
- 26. Hormonal Control of Erythropoiesis Erythropoietin (EPO) Direct stimulus for erythropoiesis Released by the kidneys in response to hypoxia
- 27. Hormonal Control of Erythropoiesis Causes of hypoxia Hemorrhage or increased RBC destruction reduces RBC numbers Insufficient hemoglobin (e.g., iron deficiency) Reduced availability of O 2 (e.g., high altitudes)
- 28. Hormonal Control of Erythropoiesis Effects of EPO More rapid maturation of committed bone marrow cells Increased circulating reticulocyte count in 1â2Ėýdays Testosterone also enhances EPO production, resulting in higher RBC counts in males
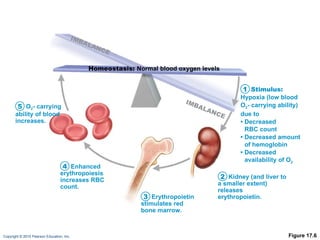
- 29. Figure 17.6 Kidney (and liver to a smaller extent) releases erythropoietin. Erythropoietin stimulates red bone marrow. Enhanced erythropoiesis increases RBC count. O 2 - carrying ability of blood increases. Homeostasis: Normal blood oxygen levels Stimulus: Hypoxia (low blood O 2 - carrying ability) due to âĒ Decreased RBC count âĒ Decreased amount of hemoglobin âĒ Decreased availability of O 2 1 2 3 4 5 IMBALANCE IMBALANCE
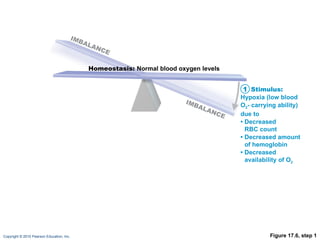
- 30. Figure 17.6, step 1 Homeostasis: Normal blood oxygen levels Stimulus: Hypoxia (low blood O 2 - carrying ability) due to âĒ Decreased RBC count âĒ Decreased amount of hemoglobin âĒ Decreased availability of O 2 1 IMBALANCE IMBALANCE
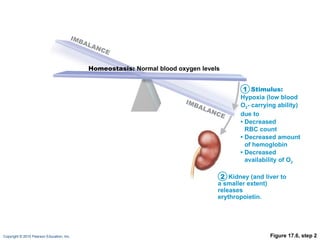
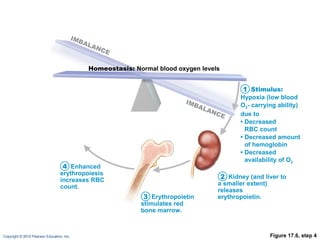
- 31. Figure 17.6, step 2 Kidney (and liver to a smaller extent) releases erythropoietin. Homeostasis: Normal blood oxygen levels Stimulus: Hypoxia (low blood O 2 - carrying ability) due to âĒ Decreased RBC count âĒ Decreased amount of hemoglobin âĒ Decreased availability of O 2 1 2 IMBALANCE IMBALANCE
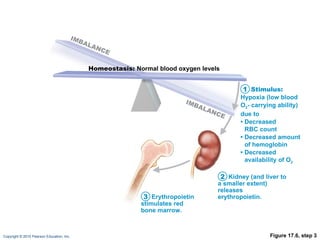
- 32. Figure 17.6, step 3 Kidney (and liver to a smaller extent) releases erythropoietin. Erythropoietin stimulates red bone marrow. Homeostasis: Normal blood oxygen levels Stimulus: Hypoxia (low blood O 2 - carrying ability) due to âĒ Decreased RBC count âĒ Decreased amount of hemoglobin âĒ Decreased availability of O 2 1 2 3 IMBALANCE IMBALANCE
- 33. Figure 17.6, step 4 Kidney (and liver to a smaller extent) releases erythropoietin. Erythropoietin stimulates red bone marrow. Enhanced erythropoiesis increases RBC count. Homeostasis: Normal blood oxygen levels Stimulus: Hypoxia (low blood O 2 - carrying ability) due to âĒ Decreased RBC count âĒ Decreased amount of hemoglobin âĒ Decreased availability of O 2 1 2 3 4 IMBALANCE IMBALANCE
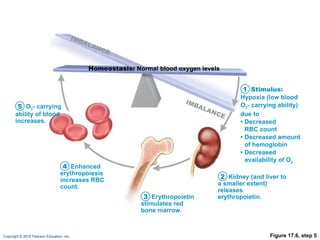
- 34. Figure 17.6, step 5 Kidney (and liver to a smaller extent) releases erythropoietin. Erythropoietin stimulates red bone marrow. Enhanced erythropoiesis increases RBC count. O 2 - carrying ability of blood increases. Homeostasis: Normal blood oxygen levels Stimulus: Hypoxia (low blood O 2 - carrying ability) due to âĒ Decreased RBC count âĒ Decreased amount of hemoglobin âĒ Decreased availability of O 2 1 2 3 4 5 IMBALANCE IMBALANCE
- 35. Dietary Requirements for Erythropoiesis Nutrientsâamino acids, lipids, and carbohydrates Iron Stored in Hb (65%), the liver, spleen, and bone marrow Stored in cells as ferritin and hemosiderin Transported loosely bound to the protein transferrin Vitamin B 12 and folic acidânecessary for DNA synthesis for cell division
- 36. Fate and Destruction of Erythrocytes Life span: 100â120 days Old RBCs become fragile, and Hb begins to degenerate Macrophages engulf dying RBCs in the spleen
- 37. Fate and Destruction of Erythrocytes Heme and globin are separated Iron is salvaged for reuse Heme is degraded to yellow the pigment bilirubin Liver secretes bilirubin (in bile)) into the intestines Degraded pigment leaves the body in feces as stercobilin Globin is metabolized into amino acids
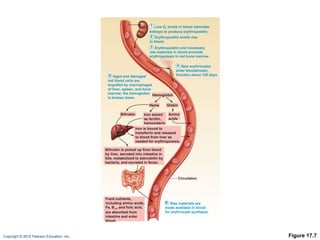
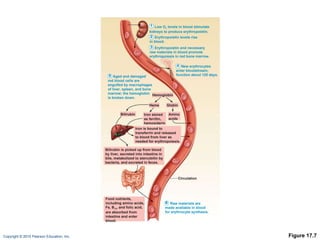
- 38. Figure 17.7 Low O 2 levels in blood stimulate kidneys to produce erythropoietin. 1 Erythropoietin levels rise in blood. 2 Erythropoietin and necessary raw materials in blood promote erythropoiesis in red bone marrow. 3 Aged and damaged red blood cells are engulfed by macrophages of liver, spleen, and bone marrow; the hemoglobin is broken down. 5 New erythrocytes enter bloodstream; function about 120 days. 4 Raw materials are made available in blood for erythrocyte synthesis. 6 Hemoglobin Amino acids Globin Iron is bound to transferrin and released to blood from liver as needed for erythropoiesis. Food nutrients, including amino acids, Fe, B 12 , and folic acid, are absorbed from intestine and enter blood. Heme Circulation Iron stored as ferritin, hemosiderin Bilirubin Bilirubin is picked up from blood by liver, secreted into intestine in bile, metabolized to stercobilin by bacteria, and excreted in feces.
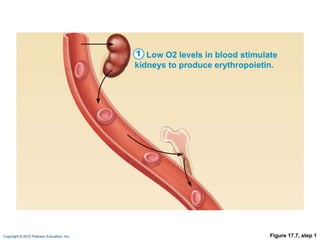
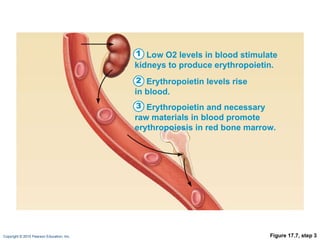
- 39. Figure 17.7, step 1 Low O2 levels in blood stimulate kidneys to produce erythropoietin. 1
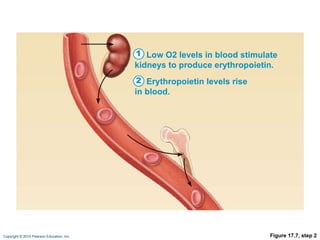
- 40. Figure 17.7, step 2 Low O2 levels in blood stimulate kidneys to produce erythropoietin. 1 Erythropoietin levels rise in blood. 2
- 41. Figure 17.7, step 3 Low O2 levels in blood stimulate kidneys to produce erythropoietin. 1 Erythropoietin levels rise in blood. 2 Erythropoietin and necessary raw materials in blood promote erythropoiesis in red bone marrow. 3
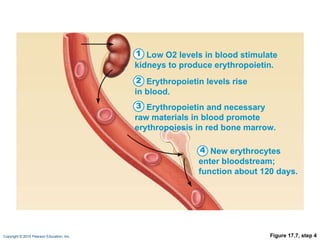
- 42. Figure 17.7, step 4 Low O2 levels in blood stimulate kidneys to produce erythropoietin. 1 Erythropoietin levels rise in blood. 2 Erythropoietin and necessary raw materials in blood promote erythropoiesis in red bone marrow. 3 New erythrocytes enter bloodstream; function about 120 days. 4
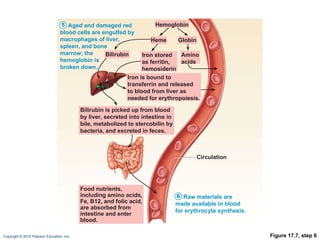
- 43. Figure 17.7, step 5 Aged and damaged red blood cells are engulfed by macrophages of liver, spleen, and bone marrow; the hemoglobin is broken down. 5 Hemoglobin Amino acids Globin Heme Circulation Iron stored as ferritin, hemosiderin Bilirubin Bilirubin is picked up from blood by liver, secreted into intestine in bile, metabolized to stercobilin by bacteria, and excreted in feces.
- 44. Figure 17.7, step 6 Aged and damaged red blood cells are engulfed by macrophages of liver, spleen, and bone marrow; the hemoglobin is broken down. 5 Raw materials are made available in blood for erythrocyte synthesis. 6 Hemoglobin Amino acids Globin Iron is bound to transferrin and released to blood from liver as needed for erythropoiesis. Food nutrients, including amino acids, Fe, B12, and folic acid, are absorbed from intestine and enter blood. Heme Circulation Iron stored as ferritin, hemosiderin Bilirubin Bilirubin is picked up from blood by liver, secreted into intestine in bile, metabolized to stercobilin by bacteria, and excreted in feces.
- 45. Figure 17.7 Low O 2 levels in blood stimulate kidneys to produce erythropoietin. 1 Erythropoietin levels rise in blood. 2 Erythropoietin and necessary raw materials in blood promote erythropoiesis in red bone marrow. 3 Aged and damaged red blood cells are engulfed by macrophages of liver, spleen, and bone marrow; the hemoglobin is broken down. 5 New erythrocytes enter bloodstream; function about 120 days. 4 Raw materials are made available in blood for erythrocyte synthesis. 6 Hemoglobin Amino acids Globin Iron is bound to transferrin and released to blood from liver as needed for erythropoiesis. Food nutrients, including amino acids, Fe, B 12 , and folic acid, are absorbed from intestine and enter blood. Heme Circulation Iron stored as ferritin, hemosiderin Bilirubin Bilirubin is picked up from blood by liver, secreted into intestine in bile, metabolized to stercobilin by bacteria, and excreted in feces.
- 46. Erythrocyte Disorders Anemia: blood has abnormally low O 2 -carrying capacity A sign rather than a disease itself Blood O 2 levels cannot support normal metabolism Accompanied by fatigue, paleness, shortness of breath, and chills
- 47. Causes of Anemia Insufficient erythrocytes Hemorrhagic anemia: acute or chronic loss of blood Hemolytic anemia: RBCs rupture prematurely Aplastic anemia: destruction or inhibition of red bone marrow
- 48. Causes of Anemia Low hemoglobin content Iron-deficiency anemia Secondary result of hemorrhagic anemia or Inadequate intake of iron-containing foods or Impaired iron absorption
- 49. Causes of Anemia Pernicious anemia Deficiency of vitamin B 12 Lack of intrinsic factor needed for absorption of B 12 Treated by intramuscular injection of B 12 or application of Nascobal
- 50. Causes of Anemia Abnormal hemoglobin Thalassemias Absent or faulty globin chain RBCs are thin, delicate, and deficient in hemoglobin
- 51. Causes of Anemia Sickle-cell anemia Defective gene codes for abnormal hemoglobin (HbS) Causes RBCs to become sickle shaped in low-oxygen situations
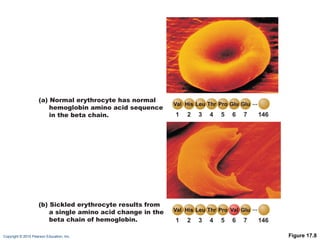
- 52. Figure 17.8 1 2 3 4 5 6 7 146 1 2 3 4 5 6 7 146 (a) Normal erythrocyte has normal hemoglobin amino acid sequence in the beta chain. (b) Sickled erythrocyte results from a single amino acid change in the beta chain of hemoglobin.
- 53. Erythrocyte Disorders Polycythemia: excess of RBCs that increase blood viscosity Results from: Polycythemia veraâbone marrow cancer Secondary polycythemiaâwhen less O 2 is available (high altitude) or when EPO production increases Blood doping
- 54. Leukocytes Make up <1% of total blood volume Can leave capillaries via diapedesis Move through tissue spaces by ameboid motion and positive chemotaxis Leukocytosis: WBC count over 11,000/mm 3 Normal response to bacterial or viral invasion
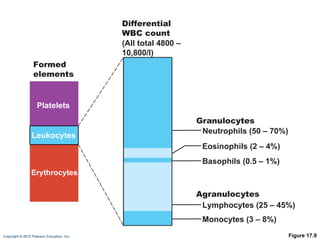
- 55. Figure 17.9 Formed elements Platelets Leukocytes Erythrocytes Differential WBC count (All total 4800 â 10,800/l) Neutrophils (50 â 70%) Lymphocytes (25 â 45%) Eosinophils (2 â 4%) Basophils (0.5 â 1%) Monocytes (3 â 8%) Agranulocytes Granulocytes
- 56. Granulocytes Granulocytes: neutrophils, eosinophils, and basophils Cytoplasmic granules stain specifically with Wrightâs stain Larger and shorter-lived than RBCs Lobed nuclei Phagocytic
- 57. Neutrophils Most numerous WBCs Polymorphonuclear leukocytes (PMNs) Fine granules take up both acidic and basic dyes Give the cytoplasm a lilac color Granules contain hydrolytic enzymes or defensins Very phagocyticââbacteria slayersâ
- 58. Eosinophils Red-staining, bilobed nuclei Red to crimson (acidophilic) coarse, lysosome-like granules Digest parasitic worms that are too large to be phagocytized Modulators of the immune response
- 59. Basophils Rarest WBCs Large, purplish-black (basophilic) granules contain histamine Histamine: an inflammatory chemical that acts as a vasodilator and attracts other WBCs to inflamed sites Are functionally similar to mast cells
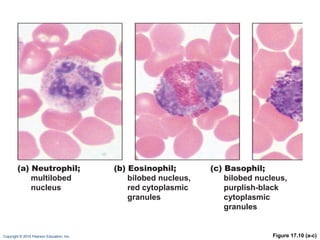
- 60. Figure 17.10 (a-c) (a) Neutrophil; multilobed nucleus (b) Eosinophil; bilobed nucleus, red cytoplasmic granules (c) Basophil; bilobed nucleus, purplish-black cytoplasmic granules
- 61. Agranulocytes Agranulocytes: lymphocytes and monocytes Lack visible cytoplasmic granules Have spherical or kidney-shaped nuclei
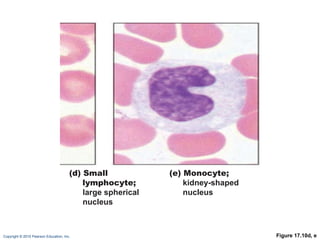
- 62. Lymphocytes Large, dark-purple, circular nuclei with a thin rim of blue cytoplasm Mostly in lymphoid tissue; few circulate in the blood Crucial to immunity
- 63. Lymphocytes Two types T cells act against virus-infected cells and tumor cells B cells give rise to plasma cells, which produce antibodies
- 64. Monocytes The largest leukocytes Abundant pale-blue cytoplasm Dark purple-staining, U- or kidney-shaped nuclei
- 65. Monocytes Leave circulation, enter tissues, and differentiate into macrophages Actively phagocytic cells; crucial against viruses, intracellular bacterial parasites, and chronic infections Activate lymphocytes to mount an immune response
- 66. Figure 17.10d, e (d) Small lymphocyte; large spherical nucleus (e) Monocyte; kidney-shaped nucleus
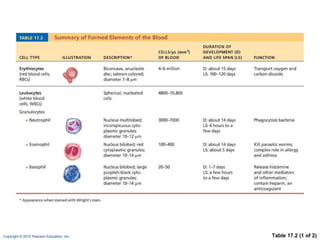
- 67. Table 17.2 (1 of 2)
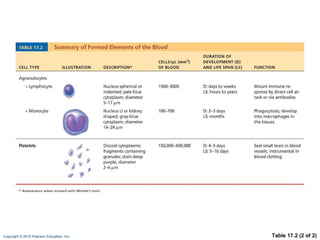
- 68. Table 17.2 (2 of 2)
- 69. Leukopoiesis Production of WBCs Stimulated by chemical messengers from bone marrow and mature WBCs Interleukins (e.g., IL-1, IL-2) Colony-stimulating factors (CSFs) named for the WBC type they stimulate (e.g., granulocyte-CSF stimulates granulocytes) All leukocytes originate from hemocytoblasts
- 70. Figure 17.11 Hemocytoblast Myeloid stem cell Lymphoid stem cell Myeloblast Myeloblast Monoblast Myeloblast Lymphoblast Stem cells Committed cells Promyelocyte Promyelocyte Promyelocyte Promonocyte Prolymphocyte Eosinophilic myelocyte Neutrophilic myelocyte Basophilic myelocyte Eosinophilic band cells Neutrophilic band cells Basophilic band cells Developmental pathway Eosinophils Neutrophils Basophils Granular leukocytes (a) (b) (c) (d) (e) Monocytes Lymphocytes Agranular leukocytes Some become Some become
- 71. Leukocyte Disorders Leukopenia Abnormally low WBC countâdrug induced Leukemias Cancerous conditions involving WBCs Named according to the abnormal WBC clone involved Myelocytic leukemia involves myeloblasts Lymphocytic leukemia involves lymphocytes Acute leukemia involves blast-type cells and primarily affects children Chronic leukemia is more prevalent in older people
- 72. Leukemia Bone marrow totally occupied with cancerous leukocytes Immature nonfunctional WBCs in the bloodstream Death caused by internal hemorrhage and overwhelming infections Treatments include irradiation, antileukemic drugs, and stem cell transplants
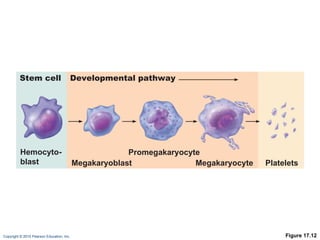
- 73. Platelets Small fragments of megakaryocytes Formation is regulated by thrombopoietin Blue-staining outer region, purple granules Granules contain serotonin, Ca 2+ , enzymes, ADP, and platelet-derived growth factor (PDGF)
- 74. Platelets Form a temporary platelet plug that helps seal breaks in blood vessels Circulating platelets are kept inactive and mobile by NO and prostacyclin from endothelial cells of blood vessels
- 75. Figure 17.12 Stem cell Developmental pathway Hemocyto- blast Megakaryoblast Promegakaryocyte Megakaryocyte Platelets
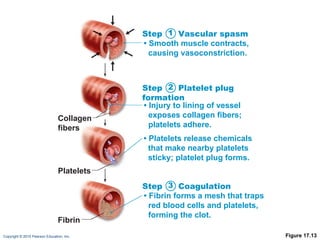
- 76. Hemostasis Fast series of reactions for stoppage of bleeding Vascular spasm Platelet plug formation Coagulation (blood clotting)
- 77. Vascular Spasm Vasoconstriction of damaged blood vessel Triggers Direct injury Chemicals released by endothelial cells and platelets Pain reflexes
- 78. Platelet Plug Formation Positive feedback cycle At site of blood vessel injury, platelets Stick to exposed collagen fibers with the help of von Willebrand factor, a plasma protein Swell, become spiked and sticky, and release chemical messengers ADP causes more platelets to stick and release their contents Serotonin and thromboxane A 2 enhance vascular spasm and more platelet aggregation
- 79. Figure 17.13 Collagen fibers Platelets Fibrin Step Vascular spasm âĒ Smooth muscle contracts, causing vasoconstriction. Step Platelet plug formation âĒ Injury to lining of vessel exposes collagen fibers; platelets adhere. âĒ Platelets release chemicals that make nearby platelets sticky; platelet plug forms. Step Coagulation âĒ Fibrin forms a mesh that traps red blood cells and platelets, forming the clot. 1 2 3
- 80. Coagulation A set of reactions in which blood is transformed from a liquid to a gel Reinforces the platelet plug with fibrin threads
- 81. Coagulation Three phases of coagulation Prothrombin activator is formed (intrinsic and extrinsic pathways) Prothrombin is converted into thrombin Thrombin catalyzes the joining of fibrinogen to form a fibrin mesh
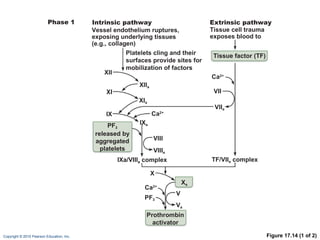
- 82. Figure 17.14 (1 of 2) Vessel endothelium ruptures, exposing underlying tissues (e.g., collagen) PF 3 released by aggregated platelets XII XI IX XII a Ca 2+ Ca 2+ XI a IX a Intrinsic pathway Phase 1 Tissue cell trauma exposes blood to Platelets cling and their surfaces provide sites for mobilization of factors Extrinsic pathway Tissue factor (TF) VII VII a VIII VIII a Ca 2+ X X a Prothrombin activator PF 3 TF/VII a complex IXa/VIII a complex V V a
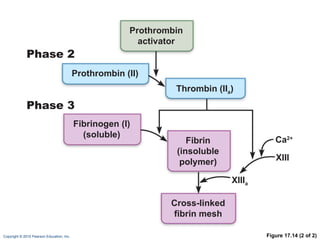
- 83. Figure 17.14 (2 of 2) Ca 2+ Phase 2 Phase 3 Prothrombin activator Prothrombin (II) Thrombin (II a ) Fibrinogen (I) (soluble) Fibrin (insoluble polymer) XIII XIII a Cross-linked fibrin mesh
- 84. Coagulation Phase 1: Two Pathways to Prothrombin Activator Initiated by either the intrinsic or extrinsic pathway (usually both) Triggered by tissue-damaging events Involves a series of procoagulants Each pathway cascades toward factorĖýX FactorĖýX complexes with Ca 2+ , PF 3 , and factorĖýV to form prothrombin activator
- 85. Coagulation Phase 1: Two Pathways to Prothrombin Activator Intrinsic pathway Is triggered by negatively charged surfaces (activated platelets, collagen, glass) Uses factors present within the blood (intrinsic) Extrinsic pathway Is triggered by exposure to tissue factor (TF) or factorĖýIII (an extrinsic factor) Bypasses several steps of the intrinsic pathway, so is faster
- 86. Coagulation Phase 2: Pathway to Thrombin Prothrombin activator catalyzes the transformation of prothrombin to the active enzyme thrombin
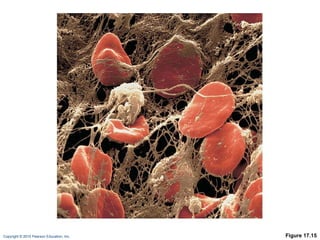
- 87. Coagulation Phase 3: Common Pathway to the Fibrin Mesh Thrombin converts soluble fibrinogen into fibrin Fibrin strands form the structural basis of a clot Fibrin causes plasma to become a gel-like trap for formed elements Thrombin (with Ca 2+ ) activates factor XIII which: Cross-links fibrin Strengthens and stabilizes the clot
- 88. Figure 17.15
- 89. Clot Retraction Actin and myosin in platelets contract within 30â60Ėýminutes Platelets pull on the fibrin strands, squeezing serum from the clot
- 90. Clot Repair Platelet-derived growth factor (PDGF) stimulates division of smooth muscle cells and fibroblasts to rebuild blood vessel wall Vascular endothelial growth factor (VEGF) stimulates endothelial cells to multiply and restore the endothelial lining
- 91. Fibrinolysis Begins within two days Plasminogen in clot is converted to plasmin by tissue plasminogen activator (tPA), factorĖýXII and thrombin Plasmin is a fibrin-digesting enzyme
- 92. Factors Limiting Clot Growth or Formation Two homeostatic mechanisms prevent clots from becoming large Swift removal and dilution of clotting factors Inhibition of activated clotting factors
- 93. Inhibition of Clotting Factors Most thrombin is bound to fibrin threads, and prevented from acting elsewhere Antithrombin III, protein C, and heparin inactivate thrombin and other procoagulants Heparin, another anticoagulant, also inhibits thrombin activity
- 94. Factors Preventing Undesirable Clotting Platelet adhesion is prevented by Smooth endothelial lining of blood vessels Antithrombic substances nitric oxide and prostacyclin secreted by endothelial cells Vitamin E quinine, which acts as a potent anticoagulant
- 95. Disorders of Hemostasis Thromboembolytic disorders: undesirable clot formation Bleeding disorders: abnormalities that prevent normal clot formation
- 96. Thromboembolytic Conditions Thrombus: clot that develops and persists in an unbroken blood vessel May block circulation, leading to tissue death Embolus: a thrombus freely floating in the blood stream Pulmonary emboli impair the ability of the body to obtain oxygen Cerebral emboli can cause strokes
- 97. Thromboembolytic Conditions Prevented by Aspirin Antiprostaglandin that inhibits thromboxane A2 Heparin Anticoagulant used clinically for pre- and postoperative cardiac care Warfarin Used for those prone to atrial fibrillation
- 98. Disseminated Intravascular Coagulation (DIC) Widespread clotting blocks intact blood vessels Severe bleeding occurs because residual blood unable to clot Most common in pregnancy, septicemia, or incompatible blood transfusions
- 99. Bleeding Disorders Thrombocytopenia: deficient number of circulating platelets Petechiae appear due to spontaneous, widespread hemorrhage Due to suppression or destruction of bone marrow (e.g., malignancy, radiation) Platelet count <50,000/mm 3 is diagnostic Treated with transfusion of concentrated platelets
- 100. Bleeding Disorders Impaired liver function Inability to synthesize procoagulants Causes include vitamin K deficiency, hepatitis, and cirrhosis Liver disease can also prevent the liver from producing bile, impairing fat and vitamin K absorption
- 101. Bleeding Disorders Hemophilias include several similar hereditary bleeding disorders Hemophilia A: most common type (77% of all cases); due to a deficiency of factor VIII Hemophilia B: deficiency of factor IX Hemophilia C: mild type; deficiency of factor XI Symptoms include prolonged bleeding, especially into joint cavities Treated with plasma transfusions and injection of missing factors
- 102. Transfusions Whole-blood transfusions are used when blood loss is substantial Packed red cells (plasma removed) are used to restore oxygen-carrying capacity Transfusion of incompatible blood can be fatal
- 103. Human Blood Groups RBC membranes bear 30 types glycoprotein antigens that are Perceived as foreign if transfused blood is mismatched Unique to each individual Promoters of agglutination and are called agglutinogens Presence or absence of each antigen is used to classify blood cells into different groups
- 104. Blood Groups Humans have 30 varieties of naturally occurring RBC antigens Antigens of the ABO and Rh blood groups cause vigorous transfusion reactions Other blood groups (MNS, Duffy, Kell, and Lewis) are usually weak agglutinogens
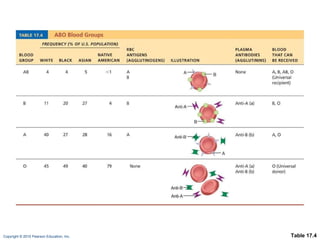
- 105. ABO Blood Groups Types A, B, AB, and O Based on the presence or absence of two agglutinogens (A and B) on the surface of the RBCs Blood may contain anti-A or anti-B antibodies (agglutinins) that act against transfused RBCs with ABO antigens not normally present Anti-A or anti-B form in the blood at about 2Ėýmonths of age
- 106. Table 17.4
- 107. Rh Blood Groups There are 45 different Rh agglutinogens (Rh factors) C, D, and E are most common Rh + indicates presence of D
- 108. Rh Blood Groups Anti-Rh antibodies are not spontaneously formed in Rh â individuals Anti-Rh antibodies form if an Rh â individual receives Rh + blood A second exposure to Rh + blood will result in a typical transfusion reaction
- 109. Homeostatic Imbalance: Hemolytic Disease of the Newborn Also called erythroblastosis fetalis Rh â mother becomes sensitized when exposure to Rh + blood causes her body to synthesize anti-Rh antibodies Anti-Rh antibodies cross the placenta and destroy the RBCs of an Rh + baby
- 110. Homeostatic Imbalance: Hemolytic Disease of the Newborn The baby can be treated with prebirth transfusions and exchange transfusions after birth RhoGAM serum containing anti-Rh can prevent the Rhâ mother from becoming sensitized
- 111. Transfusion Reactions Occur if mismatched blood is infused Donorâs cells Are attacked by the recipientâs plasma agglutinins Agglutinate and clog small vessels Rupture and release free hemoglobin into the bloodstream Result in Diminished oxygen-carrying capacity Hemoglobin in kidney tubules and renal failure
- 112. Blood Typing When serum containing anti-A or anti-B agglutinins is added to blood, agglutination will occur between the agglutinin and the corresponding agglutinogens Positive reactions indicate agglutination
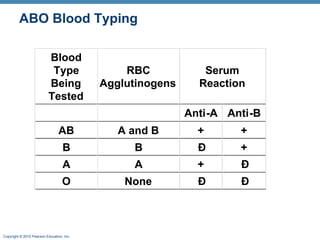
- 113. ABO Blood Typing
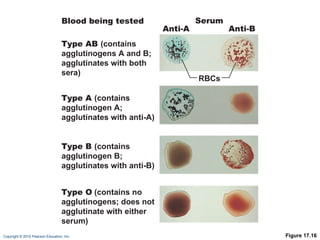
- 114. Figure 17.16 Serum Anti-A RBCs Anti-B Type AB (contains agglutinogens A and B; agglutinates with both sera) Blood being tested Type A (contains agglutinogen A; agglutinates with anti-A) Type B (contains agglutinogen B; agglutinates with anti-B) Type O (contains no agglutinogens; does not agglutinate with either serum)
- 115. Restoring Blood Volume Death from shock may result from low blood volume Volume must be replaced immediately with Normal saline or multiple-electrolyte solution that mimics plasma electrolyte composition Plasma expanders (e.g., purified human serum albumin, hetastarch, and dextran) Mimic osmotic properties of albumin More expensive and may cause significant complications
- 116. Diagnostic Blood Tests Hematocrit Blood glucose tests Microscopic examination reveals variations in size and shape of RBCs, indications of anemias
- 117. Diagnostic Blood Tests Differential WBC count Prothrombin time and platelet counts assess hemostasis SMAC, a blood chemistry profile Complete blood count (CBC)
- 118. Developmental Aspects Fetal blood cells form in the fetal yolk sac, liver, and spleen Red bone marrow is the primary hematopoietic area by the seventh month Blood cells develop from mesenchymal cells called blood islands The fetus forms HbF, which has a higher affinity for O 2 than hemoglobin A formed after birth
- 119. Developmental Aspects Blood diseases of aging Chronic leukemias, anemias, clotting disorders Usually precipitated by disorders of the heart, blood vessels, and immune system