Normal anatomical variants
•Download as PPT, PDF•
1 like•1,862 views

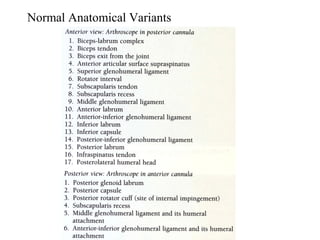
This document discusses several normal anatomical variants in the shoulder. It describes variations that can commonly occur in the superior labrum and biceps, including SLAP tears (types I-IV), vincula biceps, and bifid or absent biceps. Sublabral foramina are present in 14-60% of shoulders. The middle glenohumeral ligament is most variable with origins sometimes folded or cord-like. Small variations can also occur in the subscapularis, inferior labrum, inferior glenohumeral ligament, bare area, and posterior labrum. Distinguishing normal variants from pathologies is important for accurate diagnosis.
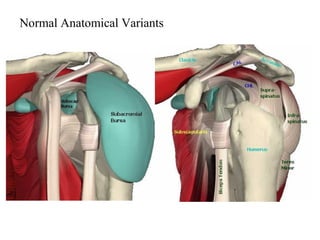

























Normal anatomical variants
- 1. Normal Anatomical Variants Steve Corbett Guys and St Thomas’ NHS Foundation Trust
- 5. Normal Anatomical Variants • Superior labrum / Biceps • Biceps • Anterosuperior Quadrant • AS head • AI Quadrant • Superior Cuff / Head • PI Quadrant • Posterior Cuff / Head • PS Quadrant • GHJ Surfaces • Bursa
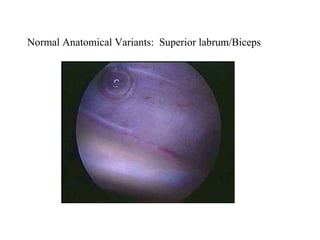
- 6. Normal Anatomical Variants: Superior labrum/Biceps
- 7. Normal Anatomical Variants: Superior labrum/Biceps
- 8. Normal Anatomical Variants: Superior labrum/Biceps • 15% loosely attached meniscal type labrum • 1-5mm width
- 9. Normal Anatomical Variants: Superior labrum/Biceps
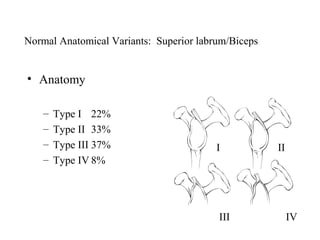
- 11. Normal Anatomical Variants: Superior labrum/Biceps • Anatomy – Type I 22% – Type II 33% – Type III 37% I II – Type IV 8% III IV
- 12. Normal Anatomical Variants: Superior labrum/Biceps • Vincula Biceps • Bifid Biceps – Small strands of – 1 part attached to cable mesentry – 2nd part attached to – Pass from biceps to tubercle surrounding capsule • Complete absence
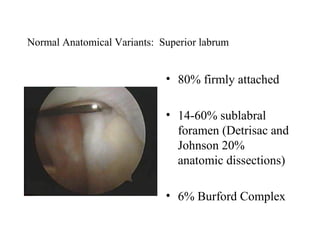
- 13. Normal Anatomical Variants: Superior labrum • 80% firmly attached • 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections) • 6% Burford Complex
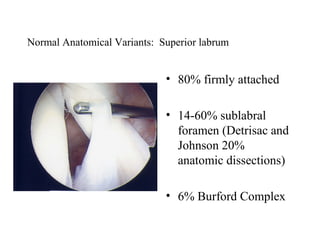
- 14. Normal Anatomical Variants: Superior labrum • 80% firmly attached • 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections) • 6% Burford Complex
- 15. Normal Anatomical Variants: Superior labrum • 80% firmly attached • 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections) • 6% Burford Complex
- 16. Normal Anatomical Variants: Superior labrum • 80% firmly attached • 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections) • 6% Burford Complex
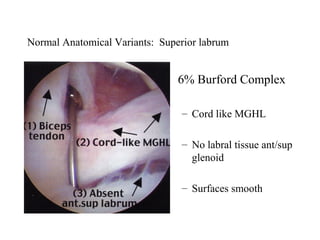
- 17. Normal Anatomical Variants: Superior labrum • 6% Burford Complex – Cord like MGHL – No labral tissue ant/sup glenoid – Surfaces smooth
- 18. Normal Anatomical Variants: Superior labrum • 6% Burford Complex – Cord like MGHL – No labral tissue ant/sup glenoid – Surfaces smooth
- 19. Normal Anatomical Variants: Superior labrum • 6% Burford Complex – Cord like MGHL – No labral tissue ant/sup glenoid – Surfaces smooth
- 20. Normal Anatomical Variants: Superior labrum • Divides sup. 2/5 and inf. 3/5. • Variable in depth
- 21. Normal Anatomical Variants: Subscapularis / SGHL • Leading edge may be split or bifid • 3% • SGHL present in nearly 100%, Occassionally frayed
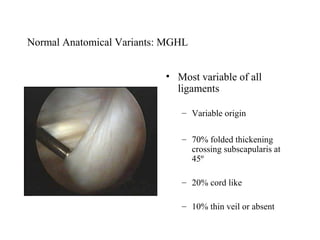
- 22. Normal Anatomical Variants: MGHL • Most variable of all ligaments – Variable origin – 70% folded thickening crossing subscapularis at 45º – 20% cord like – 10% thin veil or absent
- 23. Normal Anatomical Variants: MGHL • Most variable of all ligaments – Variable origin – 70% folded thickening crossing subscapularis at 45º – 20% cord like – 10% thin veil or absent
- 24. Normal Anatomical Variants: MGHL • Most variable of all ligaments – Variable origin – 70% folded thickening crossing subscapularis at 45º – 20% cord like – 10% thin veil or absent
- 26. Normal Anatomical Variants: Anterior Inferior Labrum • 95% smooth attachment • 5% meniscoid – Probe can be inserted but labrum not detached
- 27. Normal Anatomical Variants: Anterior Inferior Labrum • 95% smooth attachment • 5% meniscoid – Probe can be inserted but labrum not detached
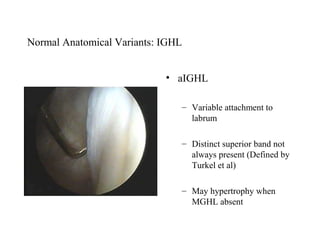
- 28. Normal Anatomical Variants: IGHL • aIGHL – Variable attachment to labrum – Distinct superior band not always present (Defined by Turkel et al) – May hypertrophy when MGHL absent
- 29. Normal Anatomical Variants: Inferior capsular recess • Normally smooth • Delicate synovial covering • Small fenestrations • Post. Sup. Band pIGHL not always well visualised (Schwartz et al)
- 30. Normal Anatomical Variants: Bare area • Bare area – 2-3 mm – 2-3 cm – Frequent indentations, deep holes – Size varies with age (De Palma)
- 31. Normal Anatomical Variants: Bare area • Must distinguish from Hill Sachs
- 32. Normal Anatomical Variants: Superior cuff • Layer of capsule and synovium • Rotator cable
- 33. Normal Anatomical Variants: Posterosuperior cuff • May have fenestrations in superficial layers
- 34. Normal Anatomical Variants: Posterior labrum / Capsule • 95% firmly attached • 5% meniscoid, firmly attached at periphery
- 35. Normal Anatomical Variants: Posterior labrum / Capsule • Normal to have a deep cleft in capsule posterior to labrum
- 36. Thank you