Hemibody and total body radiation
Download as PPTX, PDF7 likes1,250 views

This document discusses hemi-body and total body irradiation techniques. Total body irradiation (TBI) delivers a uniform whole body radiation dose and is used as a conditioning regimen before bone marrow transplantation. It was developed in the early 1900s and is now used to treat various cancers and blood disorders. TBI can be delivered using dedicated or modified conventional irradiators. Dosimetry and compensators are used to ensure uniform dose delivery. Adverse effects include nausea, vomiting, pneumonitis and cataracts. Hemi-body irradiation treats only the upper or lower half of the body and has fewer side effects than total body irradiation.


















































![Rrecent advances in linear accelerators [MR linac]](https://cdn.slidesharecdn.com/ss_thumbnails/icroproadvance2021-recentadvancesinlinearaccelerators-211201040416-thumbnail.jpg?width=560&fit=bounds)















More Related Content
What's hot (20)
Similar to Hemibody and total body radiation (20)


















Recently uploaded (20)




















Hemibody and total body radiation
- 1. HEMIBODY & TOTAL BODY IRRADIATION Dr. Dhiman Das 2nd year resident. Dept. of Radiotherapy Medical College & Hospital kolkata
- 2. Total Body Irradiation ŌĆó TBI is a special radiotherapy technique that delivers to a patients whole body a dose uniform to within +/- 10% of the prescribed dose. ŌĆó It is performed as conditioning regime
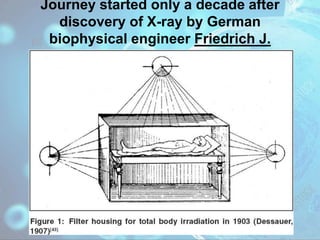
- 3. Journey started only a decade after discovery of X-ray by German biophysical engineer Friedrich J. Dessauer
- 4. ŌĆó In 1907, Alad├Īr Elfer,a medical professor in Hungary, reported his experience using a TBI technique . ŌĆó Arthur C. Heublein, in collaboration with Gioacchino Failla, is credited with the development of the first TBI unit in North America, located at Memorial Hospital in New York City.
- 5. ŌĆó In 1959, a kidney was successfully transplanted between dizygotic twins after TBI at exposures of up to 450 R. ŌĆó In 1957, Nobel laureate E. Donnall Thomas first reported the use of bone marrow infusion in humans following whole body irradiation or chemotherapy, and less than 1 year later he published his experience in using TBI with exposures up to 600 R followed by bone marrow transplantation.
- 6. Diseases treated with TBI ŌĆó Malignant ŌĆō Leukaemia. ŌĆō Aplastic anaemia. ŌĆō Lymphoma. ŌĆō Multiple Myeloma. ŌĆó Non Malignant ŌĆō Autoimmune Diseases. ŌĆō Inborn errors of metabolism. ŌĆō Aplastic anaemia
- 7. Mode of Action 1. Cytotoxicity-Destroy the bone marrow & tumour cells of the recipient. 2. Immunosuppression-Immunosuppress the patient sufficiently.
- 8. ŌĆó auto-SCT ŌĆō cytotoxicity ŌĆó allo-SCT ŌĆō cytotoxicity ŌĆō immunosuppression
- 9. Types of allo-SCT Myeloablative a) immunosuppression b) To create space in bone marrow for donor cells. c) To provide further cytoreduction. ŌĆó Example- total dose of 12- 15Gy Nonmyeloablative ŌĆó Mainly a) & b) ŌĆó c) to a much lesser degree. ŌĆó Example- 2Gy single #
- 10. Types of TBI TOTAL DOSE NO. OF # 1.HIGH DOSE TBI 12Gy 1-6 2.LOW DOSE TBI 10-15cGy/# 10-15 3.TOTAL NODAL IRRADIATION 40Gy 20
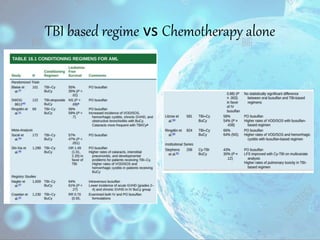
- 11. TBI based regime vs Chemotherapy alone
- 12. To conclude.. ŌĆó TBI ŌĆó Pros. ’āś Access to sanctuary sites ’āś Controllable dose delivery. ŌĆó Cons. ’āś Interstitial pneumonitis. ’āś Catarct. ’āś Endocrine deficiency ŌĆó Chemotherapy. ŌĆó Pros. ’āś No special arrangements needed like TBI ŌĆó Cons. ’āś Hepatic VOD/SOS.(BuCy) ’āś Haemorrhagic cystitis.(BuCy) ’āś Seizures.(oral busalphan)
- 13. Mode of Delivery A. Dedicated irradiator. B. Modified conventional irradiator.
- 14. A. Dedicated Irradiators. 1. Treatment at extended SSD.
- 16. 2.Treatment at standard SSD after the CoŌüČ┬░collimator is removed.
- 17. B.Modified Conventional Irradiator. 1.Treatment with a translational beam
- 18. 2.Treatment with a sweeping beam.
- 20. Choice of Technique ŌĆó Depends on- ’āśAvailable equipment ’āśPhoton beam energy ’āśMaximum possible field size ’āśTreatment distance ’āśDose rate ’āśPatient dimension
- 21. Choice of Beam Energy
- 22. Choice of Portals 1. AP/PA. o Pros ŌĆō a) Better dose uniformity along the longitudinal body axis. b) Convenient for treating small children. o Cons-patient positioning (other than standing upright) may pose problem. ’āś Developed in Memorial Sloan Kattering hospital,New York. ’āś Shielding (Dusenbery & Gerbi)- Lung,kidney, Brain.
- 24. 2.Bilateral TBI ŌĆó Pros- ŌĆō More comfortable to the patient. ŌĆó Cons- ŌĆō Greater variation in body thickness along the path of the beam.
- 26. Patient positioning ŌĆó Semifetal position(khan et al.) ŌĆó Arms are positioned laterally to follow the body contour. ŌĆó Arms should shadow the lungs, not the Spinal Column. ŌĆó Pt set-up. ŌĆó SAD
- 27. ŌĆó Compensators are designed for H&N ,lungs,legs. ŌĆó Reference thickness for compensator is the lateral diameter of the body at the level
- 28. Compensator Design ŌĆó Challenges ŌĆō ŌĆō Large variation in body thickness. ŌĆō Lack of complete body immobilisation. ŌĆō Internal tissue heterogeneities.
- 29. Compensator Thickness along a ray line a) Tissue deficit, compared to the reference depth at the prescription point. b) Material(density). c) Distance from the point of compensation. d) Depth of the point of compensation. e) Field size. f) Beam energy.
- 30. Thickness Ratio(Žä) ŌĆó The required thickness of a tissue equivalent compensator that gives the same dose at the point of interest as would a bolus of thickness equal to the tissue deficit. ŌĆó For TBI an average value of 0.7 provides good approximation of all beam energies & compensation conditions.
- 31. Formulae to obtain compensator thickness 1. ŌĆó Tc=comp thickness ŌĆó TD=tissue deficit ŌĆó ╬Īc=density of comp 2. ŌĆó I/I╠ź=doses before & after comp added. ŌĆó T(Aß┤┐dß┤┐) &T(A d)=TPR for ref body section & sectn to be compensated.
- 33. Dosimetry A.Directly ŌĆó By using a 0.6cmߥī Farmer- type ionisation chamber placed in a 40cmߥī water phantom. ŌĆó By placing TLD capsule/chips in strategic locations in body.(in-vivo dosimetry) B.Indirectly ŌĆó By using this formula.
- 34. Adverse effects In nonmyeloablative regimen Acute ’ā╝Nausea ’ā╝Vomiting Long term ’ā╝cataract
- 35. Adverse effects In myeloablative regimens Acute ’ā╝ Nausea, Vomiting ’ā╝ mucositis ’ā╝ Diarrhoea ’ā╝ Xerostomia ’ā╝ Headache ’ā╝ Fever ’ā╝ HTN ’ā╝ Reversible alopecia ’ā╝ Parotiditis Long-term ’ā╝ Lung-interstitial pneumonitis. ’ā╝ Lens-cataract. ’ā╝ Growth & gonadal & Endocrine effects. ’ā╝ Liver-VOD & SOS ’ā╝ Kidney. ’ā╝ 2┬░ cancers.
- 36. HEMI BODY IRRADIATION ŌĆó INDICATIONS- ŌĆō To alleviate symptoms in metastatic diseases. ŌĆō Delaying progression of existing asymptomatic mets. ŌĆō Defers development of new mets.
- 37. Difference with TBI ŌĆó Different therapeutic goal. ŌĆó Smaller field size. ŌĆó Lesser side effects
- 38. Technique ŌĆó Bottom of L4 separates uper & lower half. ŌĆó A/P parallal opposed fields. ŌĆó Patients positioned with vertical beam allowing coverage of hemibody. ŌĆó Necessary shielding. ŌĆó Dose prescribed to mid-plane of the patient at the central axis of the beam.
- 39. Dose ŌĆó Upper HBI-6Gy ŌĆó Lower HBI-8Gy Rx for other half ŌĆó Wait for 6-8 weeks.
- 40. Side effects ’āśNausea ,vomiting(M/C) ’āśFatigue. ’āśCough, breathlessness. ’āśInterstitial pneumonitis. ’āśReversible alopecia ’āśDry mouth, stomatitis. ’āśParotid swelling.