




















![Reproduction+work+sheet+isn[1]](https://cdn.slidesharecdn.com/ss_thumbnails/reproductionworksheetisn1-121003141732-phpapp02-thumbnail.jpg?width=560&fit=bounds)










More Related Content
Similar to Child Case History Form.pdfasdsaﺣ ssasfgg (20)
Recently uploaded (20)






Child Case History Form.pdfasdsaﺣ ssasfgg
- 1. Page 1 of 4 _____/____/____ Client No: ________ CHILD CASE HISTORY FORM All questions contained in this questionnaire are strictly confidential and will become part of the childﻗs record. Name: ____________________________________________________ DOB _____/______/_________ (Last, First, MI) Address: _______________________________________________ Home/cell phone: ___________________ City, State, ZIP __________________________________________Work phone: ________________________ Best time to phone: _____________________________ Previous or Referring Doctor: __________________________________________________________________ FAMILY INFORMATION Parents Name Age Occupation Highest Education Level Name of person completing this questionnaire: _____________________________________________________ Relationship to child:__________________________________________________________________________ If the address of either parent is different from that of the child, please indicate below. ___________________________________________________________________________________________ Other children in the family: Name Gender Age Any speech, language or hearing problems? Please explain. Who referred you to the Speech, Language and Hearing Clinic? ________________________________________ Has your child received speech or language therapy in the past? ________________________________________ If so, who was the childﻗs speech-language pathologist? ______________________________________________ Is the child currently enrolled in therapy? ______ If so, where? _______________________________________ Childﻗs doctor(s) _____________________________________________________________________________ ___________________________________________________________________________________________ Why are you seeking our services at this time?______________________________________________________ ___________________________________________________________________________________________ What do you expect to achieve from our services?___________________________________________________ ___________________________________________________________________________________________ When was the speech or language difficulty first noticed? ____________________________________________ Who noticed it? ______________________________________________________________________________
- 2. Page 2 of 4 PRE-NATAL /BIRTH HISTORY Biological motherﻗs age at time of pregnancy: ______________________________________________________ Any medical problems before this pregnancy: Yes ﻗ۰ No ﻗ۰ If yes, please explain. ________________________ ___________________________________________________________________________________________ Did the mother have any of the following during the pregnancy? German Measles ﻗ۰ Toxemia ﻗ۰ Accidents/Injuries ﻗ۰ Anemia ﻗ۰ Hospitalization ﻗ۰ Other ﻗ۰ Please explain above complications:______________________________________________________________ ___________________________________________________________________________________________ Please check and explain all that apply: ﻗ۰ Mother took medication during pregnancy _______________________________________________________ ﻗ۰ Child was born prematurely___________________________________________________________________ ﻗ۰ Prolonged labor ____________________________________________________________________________ ﻗ۰ Forceps used ______________________________________________________________________________ ﻗ۰ Caesarean Section __________________________________________________________________________ ﻗ۰ Breech birth _______________________________________________________________________________ ﻗ۰ Mother given drugs during labor/delivery _______________________________________________________ ﻗ۰ Low birth weight ___________________________________________________________________________ ﻗ۰ Small for gestational age _____________________________________________________________________ ﻗ۰ Rh Factor _________________________________________________________________________________ ﻗ۰ Child received oxygen at birth ________________________________________________________________ ﻗ۰ Other complications ________________________________________________________________________ ________________________________________________________________________________________ DEVELOPMENTAL HISTORY Please give ages which the following first occurred: MILESTONE AGE FIRST OCCURRED MILESTONE AGE FIRST OCCURRED Held up head Sat up unsupported Crawled Reached for an object Stood Walked unaided Ran First tooth erupted First word Put two words together Bladder trained Bowel trained Night trained Fed self Which hand does the child use most frequently? Right ﻗ۰ Left ﻗ۰ No preference ﻗ۰ Does your child have difficulty walking, running, or participating in other activities which require small or large muscle coordination? _________________________________________________________________________ Are there or have there ever been any feeding problems (e.g., problems with sucking, swallowing, drooling, chewing, etc.?) If yes, please describe. ____________________________________________________________ Describe the childﻗs response to sound (please check all that apply): Responds to all sounds ﻗ۰ Responds to loud sounds ﻗ۰ Inconsistently responds to sounds ﻗ۰ MEDICAL HISTORY
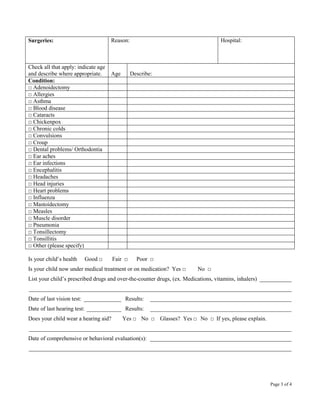
- 3. Page 3 of 4 Surgeries: Reason: Hospital: Check all that apply: indicate age and describe where appropriate. Age Describe: Condition: ﻗ۰ Adenoidectomy ﻗ۰ Allergies ﻗ۰ Asthma ﻗ۰ Blood disease ﻗ۰ Cataracts ﻗ۰ Chickenpox ﻗ۰ Chronic colds ﻗ۰ Convulsions ﻗ۰ Croup ﻗ۰ Dental problems/ Orthodontia ﻗ۰ Ear aches ﻗ۰ Ear infections ﻗ۰ Encephalitis ﻗ۰ Headaches ﻗ۰ Head injuries ﻗ۰ Heart problems ﻗ۰ Influenza ﻗ۰ Mastoidectomy ﻗ۰ Measles ﻗ۰ Muscle disorder ﻗ۰ Pneumonia ﻗ۰ Tonsillectomy ﻗ۰ Tonsillitis ﻗ۰ Other (please specify) Is your childﻗs health Good ﻗ۰ Fair ﻗ۰ Poor ﻗ۰ Is your child now under medical treatment or on medication? Yes ﻗ۰ No ﻗ۰ List your childﻗs prescribed drugs and over-the-counter drugs, (ex. Medications, vitamins, inhalers) ___________ ___________________________________________________________________________________________ Date of last vision test: _____________ Results: _________________________________________________ Date of last hearing test: ____________ Results: _________________________________________________ Does your child wear a hearing aid? Yes ﻗ۰ No ﻗ۰ Glasses? Yes ﻗ۰ No ﻗ۰ If yes, please explain. ___________________________________________________________________________________________ Date of comprehensive or behavioral evaluation(s): _________________________________________________ ___________________________________________________________________________________________
- 4. Page 4 of 4 EVERY DAY INFORMATION Is English the primary language in the home? Yes ﻗ۰ No ﻗ۰ If not, what is the primary language? _____________ Please describe how your child interacts with others? (e.g., shy, aggressive, uncooperative, etc.) ______________ ___________________________________________________________________________________________ How does your child get along with other children? _________________________________________________ ___________________________________________________________________________________________ Does your child prefer to play alone? _____________________________________________________________ Does your child have pretend play (pretends to go to work like mom/day, drinks pretend tea, etc.) ____________ ___________________________________________________________________________________________ What are your childﻗs favorite TV shows? _________________________________________________________ ___________________________________________________________________________________________ Does your child have a favorite stuffed animal or cartoon character? ____________________________________ ___________________________________________________________________________________________ How does the child get along with brothers and sisters?_______________________________________________ ___________________________________________________________________________________________ What kinds of activities are engaged in by the whole family? __________________________________________ ___________________________________________________________________________________________ What things does the child do particularly well? ____________________________________________________ EDUCATIONAL INFORMATION Childﻗs current grade level: ____________________________________________________________________ School:_____________________________________________________________________________________ Teacher(s):__________________________________________________________________________________ How is your child doing academically? ___________________________________________________________ If enrolled for special services, has an Individual Educational Plan (IEP) been developed? If yes, please describe your childﻗs goals or attach a copy of his/her IEP. ___________________________________________________ ___________________________________________________________________________________________ Please provide any additional information that may be helpful in the evaluation or treatment of your child. ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________