




















![Club foot[1]](https://cdn.slidesharecdn.com/ss_thumbnails/clubfoot1-160908070000-thumbnail.jpg?width=560&fit=bounds)





















More Related Content
Similar to Club foot congenital disorders pediatrics (20)
More from Nitesh yadav (11)









Recently uploaded (20)




















Club foot congenital disorders pediatrics
- 2. ŌĆó Introduction ŌĆó Definition ŌĆó EPIDEMIOLOGY ŌĆó Cause ŌĆó Sign and symptoms ŌĆó Complications ŌĆó Diagnosis ŌĆó Treatment
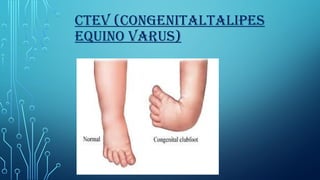
- 3. ŌĆó Clubfoot, also known as Congenital Talipes Equino varus, is a complex, congenital deformity of the foot. C ŌĆō Cavus (increased longitudinal arch of the feet) A ŌĆō Adduction (tarsal bones directed towards the median plane) V ŌĆō Varus (inversion and adduction of the calcaneal bones) ŌĆó E ŌĆō Equinus (increased plantar flexion of the ankles) Introduction
- 5. DEFINITION ŌĆó It is defined as a deformity characterized by complex, malalignment of the foot involving soft and bony structures in the hind foot, mid foot and forefoot. ŌĆó Clubfoot is a congenital foot deformity that affects the bones, muscles, tendons, and blood vessels in a childŌĆÖs foot ŌĆó It is usually present at birth and can range from mild to severe
- 6. ŌĆó It is the most common congenital malformation of the foot affecting 1-2 newborns per 1000. ŌĆó It is twice as common in males than females. ŌĆó Clubfoot may be unilateral (30%-40%) one or bilateral (60%-70%). ŌĆó A normally developing foot turns into a club foot during 2nd trimester of pregnancy. ŌĆó Rarely detect with USG before 16th week. EPIDEMIOLOGY
- 7. ETIOLOGY/ CAUSES Hereditary factor Fetal position Extra uterine compression Breech presentation ŌĆó Neurological disorder
- 8. SIGN AND SYMPTOMS ŌĆó The physical appearance of the clubfoot may also vary. One or both feet may be affected. ŌĆó Feet turning inwards ŌĆó Tightness in the calf muscles ŌĆó The foot has decreased joint range of the movement. ŌĆó Resting of the foot on its outer border ŌĆó Rigidity and other changes in the movement of the foot
- 9. COMPLICATIONS ŌĆó Clubfoot typically doesn't cause any problems until your child starts to stand and walk. If the clubfoot is treated, your child will most likely walk fairly normally. He or she may have some difficulty with: ŌĆó Movement. The affected foot may be slightly less flexible. ŌĆó Leg length. The affected leg may be slightly shorter, but generally does not cause significant problems with mobility. ŌĆó Calf size. The muscles of the calf on the affected side may always be smaller than those on the other side. ŌĆó Arthritis. Your child is likely to develop arthritis.
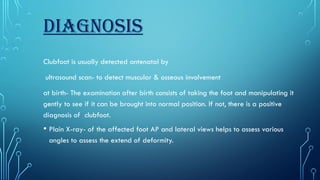
- 10. DIAGNOSIS Clubfoot is usually detected antenatal by ultrasound scan- to detect muscular & osseous involvement at birth- The examination after birth consists of taking the foot and manipulating it gently to see if it can be brought into normal position. If not, there is a positive diagnosis of clubfoot. ŌĆó Plain X-ray- of the affected foot AP and lateral views helps to assess various angles to assess the extend of deformity.
- 11. TREATMENT Clubfoot treatment includes several methods. Your care team will discuss the options with you and figure out which works best for your child. Treatments include: Ponseti method: Stretches and casts on your childŌĆÖs leg to correct the curve. French method: Stretches and splints on their leg to correct the curve. Bracing: Uses special shoes to keep their foot at the proper angle. ŌĆó Surgery: May be an option if other methods donŌĆÖt work.
- 12. PT TREATMENT Physical therapy for Club Foot will be used to stretch the structures of the foot including the tendons, ligaments, and muscles to adjust the foot and keep it in the proper position. If surgery is needed, physical therapy will be initiated after the procedure to ensure that the correction takes hold. ŌĆó Bracing will be a critical component of recovery from a fixed Club Foot. ŌĆóManual therapeutic technique (MTT) ŌĆóHands on care including soft tissue massage, stretching and joint mobilization by a physical therapist to improve alignment, mobility and range of motion of the foot. The use of mobilization techniques also helps to modulate pain.
- 13. ŌĆóTherapeutic Techniques ŌĆó Including stretching and strengthening exercises to regain range of motion and strengthen muscles of the foot and lower extremity to support. ŌĆóTaping Technique is Also Useful. ŌĆóTo restore stability, retrain the lower extremity and improve movement techniques and mechanics (for example, walking, gait training, running or jumping) of the involved lower extremity to reduce stress on the joint surfaces in daily activities. ŌĆóRhythmic and repeated gentle manipulation. ŌĆóStrapping and plaster of Paris (POP) cast. ŌĆóEducation and instructions to the mother and/or parents. ŌĆóModalities including the use of ultrasound, electrical stimulation, ice, cold, laser and others to decrease pain and inflammation of the involved joint.
- 14. Taping and cast method for CTEV
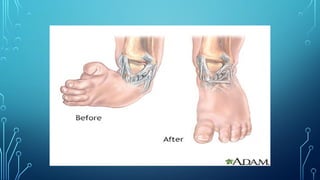
- 15. SURGICAL TREATMENT Sometimes, a child has severe clubfoot. Or youŌĆÖve tried nonsurgical methods, but they havenŌĆÖt worked. Surgery can correct the problem. ItŌĆÖs best if your child has the surgery before they start walking. During the procedure, the surgeon: Lengthens your babyŌĆÖs heel cord and fixes other problems with their foot or feet. Places pins in their foot to correct the position. ŌĆó Puts a cast on their foot after the surgery.
- 17. A few weeks after the surgery, the surgeon: Removes the cast and pins. Puts a new cast on your childŌĆÖs foot, which your child wears for about another four weeks. Removes the final cast. ŌĆó ThereŌĆÖs still a chance their foot could return to the clubfoot position. Your provider may recommend bracing or special shoes to keep their foot in the correct position.
- 18. TREATMENT BY EXTERNAL FIXATORS There are two types of external fixator frame- One is Designed by Ilizarov, a Russian orthopedic surgeon ŌĆó The second one is designed by an Indian orthopedic surgeon, BB Joshi. This frame is known as JoshiŌĆÖs external stabilization system popularly called JESS.
- 19. SPLINT ŌĆó Is a device used for holding a part of the body stable to decrease pain and prevent further injury.
- 20. CTEV SHOES