The document discusses the physiological and hormonal changes during pregnancy, focusing on the roles of progesterone, estrogen, and relaxin. It outlines the effects of these hormones on various systems, including reproductive, cardiovascular, respiratory, gastrointestinal, and musculoskeletal systems. Additionally, it details physical changes, symptoms experienced by pregnant women, and the impact on posture and balance throughout the trimesters.
physiological effects on different systems of body during pregnancyshifanoor4
╠²
The document summarizes various physiological changes that occur during pregnancy across multiple body systems. Key changes include:
- Increased blood volume, cardiac output, and respiratory rate to support growth of the fetus and placenta.
- Softening of ligaments and joints due to relaxin to accommodate birth.
- Enlargement and changes in position of organs like the uterus, kidneys, and breasts to make room for the growing fetus.
- Increased progesterone and estrogen levels impacting muscles, metabolism, and other functions to sustain pregnancy.
- Common symptoms like nausea and back pain emerge from these systemic adaptations during each trimester.
Hormonal changes during pregnancy cause physiological changes in multiple body systems. Progesterone, estrogen, and relaxin are the three main hormones. They cause increased blood volume, uterine growth accommodating the fetus, softening of tissues, and postural changes. Specific effects include relaxation of smooth muscles, increased temperature and breathing rate, breast growth in preparation for lactation, skin pigmentation, and softening of joints. These changes help support the developing fetus and prepare the mother's body for childbirth and nursing.
Physiological changes during pregnancy.pptHudeifyAhmed
╠²
The document discusses the physiological changes that occur during pregnancy, covering systemic adaptations, cardiovascular alterations, respiratory adjustments, and changes in endocrine function. It details significant developments such as increased blood volume, changes in oxygen consumption, alterations in renal function, and adaptations of the reproductive organs. Additionally, it addresses symptoms and signs of pregnancy and methods for diagnosis through tests and examinations.
Physiological changes in pregnancy include increased blood volume, cardiac output, and kidney function to support the developing fetus. The uterus grows dramatically throughout pregnancy. Hormonal changes like increased estrogen, progesterone, and HCG levels from the placenta help prepare the body for pregnancy and childbirth. Diagnosis of pregnancy is suggested by missed periods and confirmed by tests detecting HCG in urine or blood within 4-5 weeks of conception.
Phsiology Of Pregnancy, Female Pelvic Anatomy Mob: 7289915430, www.drpradeepgargPradeep Garg
╠²
The document discusses diagnosis and physiology of pregnancy. It covers signs and symptoms of pregnancy in each trimester. Physiological changes include enlargement of the uterus, breast changes, weight gain, increased blood volume and cardiac output. Hormones produced by the placenta like HCG, HPL and progesterone help maintain pregnancy and influence maternal physiology. The kidneys and thyroid also undergo changes to accommodate the demands of pregnancy.
Physiological changes during pregnancy allow the mother's body to support fetal growth and development. The cardiovascular, respiratory, gastrointestinal, urinary, and endocrine systems undergo remodeling. The cardiovascular system increases blood volume and cardiac output by 40% by the third trimester. Respiration increases to meet higher oxygen needs. Hormonal changes, like increased progesterone and estrogen, prepare the uterus and breasts for birth. Overall, the adaptations sustain a healthy environment for the fetus throughout pregnancy.
Physiological changes during pregnancy allow the mother's body to support fetal growth and development. The cardiovascular, respiratory, gastrointestinal, urinary, and endocrine systems undergo remodeling. The cardiovascular system increases blood volume and cardiac output by 40% by the third trimester. The respiratory system compensates for increased oxygen needs through hyperventilation. Hormonal changes, like increased estrogen and progesterone, prepare the breasts, uterus, and other organs for childbirth. These adaptations maintain a healthy environment for the developing fetus.
Physiological changes in pregnancy include increased blood volume, cardiac output, and respiration. The uterus grows significantly to accommodate the fetus, while other systems like renal and endocrine adapt to support the demands of pregnancy. Diagnosis involves tests to detect hCG in urine or blood from very early pregnancy, and ultrasound to visualize the developing fetus.
The document provides an overview of the physiological changes that occur throughout the maternal body during pregnancy. Key changes discussed include:
- Uterine growth and changes to support fetal development.
- Increased cardiac output, blood volume, and vascular changes to support nutrient/waste exchange between mother and fetus.
- Respiratory changes like increased tidal volume to support oxygen demands.
- Renal changes like increased GFR and kidney size to excrete wastes and support calcium/electrolyte balance.
- Metabolic changes to support fetal growth including increased lipids, proteins, and iron.
- Skin changes like line striae and pigmentation due to hormonal influences.
- Central nervous
The document summarizes various physiological changes that occur in a woman's body during pregnancy. The reproductive system undergoes significant changes like increased vascularity of the vulva, vagina and cervix. The uterus enlarges dramatically from 50g to 900g at term. The cardiovascular system works harder with increased cardiac output and blood volume. Respiration is also impacted with increased oxygen demands. Common complaints include nausea, backaches, leg cramps and frequent urination. Hormone levels like HCG, estrogen, progesterone and prolactin rise substantially. Overall weight gain of 10-12kg occurs to support fetal growth and changes in maternal tissues.
This document discusses the extensive physiological and anatomical changes that occur during normal human pregnancy. It provides details on adaptations in multiple organ systems to support the growth and development of the fetus. The main changes include increased blood volume and cardiac output, anatomical changes to the uterus and cervix, hormonal changes involving hCG and estrogen, and metabolic adaptations to provide optimal nutrition for the fetus. All major body systems are impacted in ways that precisely meet the needs of pregnancy.
Physiological changes during pregnancy include:
1. Enlargement of the uterus, cervix, breasts, and other reproductive organs.
2. Increased blood volume, heart rate, and respiration to support the growing fetus and maternal organs.
3. Hormonal changes like increased progesterone and estrogen from the placenta lead to changes in metabolism, immune function, and other systems throughout the body.
3.physiolosical changes during pregnancyKHUSHBU PATEL
╠²
During pregnancy, the woman's body undergoes many physiological changes to support the growing fetus. The reproductive system changes include increased blood flow and size of the vagina, cervix, and uterus. The uterus grows enormously from about the size of a fist to over 1000 times larger by term. Other systems affected are cardiovascular (increased heart rate and blood volume), respiratory, digestive, urinary, endocrine, and musculoskeletal. Hormonal changes produced by the placenta, such as human chorionic gonadotropin, estrogen, progesterone, prolactin, and human placental lactogen, cause these adaptations to pregnancy.
The document describes several physiological changes that occur in pregnancy. The uterus grows enormously from about 70g to over 1kg by term. This displaces other organs and alters the body's shape and center of gravity. Hormonal changes lead to increased blood volume, cardiac output, and kidney function to support the demands of the fetus. The lungs take on a higher ventilation rate. The digestive system slows while the liver works to support the added metabolic load. Overall, the body undergoes extensive adaptations to accommodate the growing fetus.
Physiological changes during pregnancy can be extensive. The document summarizes several key changes:
1) The uterus grows enormously in size and weight to accommodate the growing fetus. Other genital organs like the cervix and breasts also see significant changes to support pregnancy and birth.
2) Extensive changes occur in many body systems like the cardiovascular, respiratory, urinary and endocrine systems to support the nutritional and oxygen needs of the mother and fetus. This includes increases in blood volume, cardiac output, kidney size and lung capacity.
3) Hormonal changes are also profound, with high levels of progesterone, estrogen and other placental hormones influencing many processes and organs across the body to sustain the pregnancy.
The document outlines the physiological, endocrine, and anatomical changes that occur during pregnancy as adaptations to support fetal development. Key adaptations include increased blood volume, changes in cardiovascular and respiratory function, alterations in renal and gastrointestinal systems, and various hormonal shifts. Understanding these changes is crucial for appropriate management of obstetric clinical problems.
PHYSIOLOGICAL CHANGES IN PREGNANCY.pptxKamauNDavid
╠²
Physiological changes occur throughout pregnancy to support the growth and development of the fetus. The uterus enlarges significantly, increasing in size from about the size of a fist to filling most of the abdomen. Other organs like the breasts and cervix undergo changes to prepare for lactation and birth. There are increases in blood volume and cardiac output to meet the higher demands of the mother and fetus. Hormonal changes influence metabolism and fluid balance. The kidneys increase in size and function to filter wastes and regulate fluid levels despite rising blood pressure. Respiration is also impacted as the growing uterus displaces the diaphragm upwards.
IRH - Physiology of Pregnancy Obstetric.pdfGadzika Gunda
╠²
The document provides an extensive overview of the physiology of pregnancy, discussing the physiological changes that occur in various body systems including the endocrine, cardiovascular, respiratory, urinary, gastrointestinal, and integumentary systems as the body adapts to support a developing fetus. It details hormonal changes, organ adaptations, and the importance of these changes in maintaining pregnancy, nourishing the fetus, and preparing the body for labor and lactation. Additionally, it outlines signs and symptoms of pregnancy, both subjective and objective, along with diagnostic indicators that can confirm pregnancy.
Systemic changes during antenatal period by tanoj patidar msc nursingTanoj Patidar
╠²
Pregnancy induces significant respiratory and gastrointestinal changes due to the enlarging uterus and hormonal effects, leading to altered lung volumes, increased oxygen consumption, and changes in gastrointestinal motility, with common symptoms like dyspnea and heartburn. The endocrine system adapts as the placenta becomes the primary hormone producer, impacting thyroid and adrenal functions, and altering metabolic processes including protein, carbohydrate, and fat metabolism to support fetal growth. Overall, pregnancy results in a complex interplay of anatomical and physiological changes essential for maternal and fetal health.
Physiological changes during pregnancy by Harrison MboheHarrisonMbohe
╠²
The document summarizes many of the physiological changes that occur in a woman's body during pregnancy. Key changes include enlargement and increased blood flow to the uterus, breasts, kidneys and other organs. The cardiovascular system adapts with increased blood volume and heart rate. Hormonal changes impact metabolism, thyroid and cortisol levels. Other changes involve the skin, respiratory and musculoskeletal systems to accommodate the growing fetus.
Physiology of Pregnancy for Undergraduatesthezaira
╠²
The document summarizes the physiological changes that occur throughout a woman's body during pregnancy. Key changes include enlargement and increased blood flow to the uterus, breasts, and major organs. Other changes are weight gain and fluid retention, increased blood volume and altered metabolism to support the growing fetus. The various body systems also adapt to pregnancy through respiratory alkalosis, circulatory adjustments and neurological/hormonal responses.
The document discusses various physiological changes that occur in pregnancy across multiple body systems. The uterus increases dramatically in size from 70g and 10mL non-pregnant to approximately 1100g and 5L by the end of pregnancy. Hormonal changes include increased estrogen, progesterone, hCG, hPL, prolactin, IGF, and decreased hGH levels. This leads to adaptations in various organ systems like increased blood volume by 45%, enlarged heart and increased cardiac output, mild anemia and thrombocytopenia, immunosuppression to tolerate the fetus, and metabolic changes in carbohydrate and fat metabolism. Respiration is also altered to support higher oxygen demands.
Physiological changes during pregnancy include changes in the genital organs, breasts, skin, abdomen, blood, metabolism, cardiovascular and urinary systems. The genital organs like the uterus, cervix and breasts enlarge and the blood volume increases significantly. Metabolism increases to support the growth of the fetus. The heart enlarges and cardiac output increases. Kidney function is enhanced and urinary frequency rises, especially later in pregnancy. Respiration is also impacted with higher oxygen needs.
The document discusses the hormonal regulation of pregnancy. It describes the key hormones produced by the placenta and fetal adrenal gland, including human chorionic gonadotropin, human placental lactogen, progesterone, and estrogen. It explains how these hormones facilitate adaptations in various maternal systems and are responsible for the physiological symptoms of pregnancy. The document also outlines the hormones involved in labor and lactation, including oxytocin and prolactin.
Physiological changes in pregnancy (2).pptsamuellamaryk
╠²
This document summarizes the major physiological adaptations that occur during pregnancy. It discusses changes to volume homeostasis and the cardiovascular, respiratory, urinary, digestive and endocrine systems. Key adaptations include a 30% increase in blood volume, decreased systemic vascular resistance, and increased cardiac output. Hormonal changes like increased progesterone and estrogen help prepare the uterus for growth and childbirth. Pregnancy can be diagnosed through missed periods, physical exams signs, and tests like urine/blood tests to detect hCG and ultrasound exams.
Pregnancy causes many anatomical, physiological, and biomechanical changes in the body to support fetal development and birth. The uterus grows enormously over the course of pregnancy. Other systems like cardiovascular, respiratory, and renal systems also adapt to support increased demands on the mother. Hormonal changes induce physical changes in breasts, skin, ligaments and other tissues. Proper understanding of normal pregnancy changes helps healthcare providers manage common issues and risks.
Physiological changes during pregnancy allow the mother's body to support fetal growth and development. The cardiovascular, respiratory, gastrointestinal, urinary, and endocrine systems undergo remodeling. The cardiovascular system increases blood volume and cardiac output by 40% by the third trimester. The respiratory system compensates for increased oxygen needs through hyperventilation. Hormonal changes, like increased estrogen and progesterone, prepare the breasts, uterus, and other organs for childbirth. These adaptations maintain a healthy environment for the developing fetus.
Physiological changes in pregnancy include increased blood volume, cardiac output, and respiration. The uterus grows significantly to accommodate the fetus, while other systems like renal and endocrine adapt to support the demands of pregnancy. Diagnosis involves tests to detect hCG in urine or blood from very early pregnancy, and ultrasound to visualize the developing fetus.
The document provides an overview of the physiological changes that occur throughout the maternal body during pregnancy. Key changes discussed include:
- Uterine growth and changes to support fetal development.
- Increased cardiac output, blood volume, and vascular changes to support nutrient/waste exchange between mother and fetus.
- Respiratory changes like increased tidal volume to support oxygen demands.
- Renal changes like increased GFR and kidney size to excrete wastes and support calcium/electrolyte balance.
- Metabolic changes to support fetal growth including increased lipids, proteins, and iron.
- Skin changes like line striae and pigmentation due to hormonal influences.
- Central nervous
The document summarizes various physiological changes that occur in a woman's body during pregnancy. The reproductive system undergoes significant changes like increased vascularity of the vulva, vagina and cervix. The uterus enlarges dramatically from 50g to 900g at term. The cardiovascular system works harder with increased cardiac output and blood volume. Respiration is also impacted with increased oxygen demands. Common complaints include nausea, backaches, leg cramps and frequent urination. Hormone levels like HCG, estrogen, progesterone and prolactin rise substantially. Overall weight gain of 10-12kg occurs to support fetal growth and changes in maternal tissues.
This document discusses the extensive physiological and anatomical changes that occur during normal human pregnancy. It provides details on adaptations in multiple organ systems to support the growth and development of the fetus. The main changes include increased blood volume and cardiac output, anatomical changes to the uterus and cervix, hormonal changes involving hCG and estrogen, and metabolic adaptations to provide optimal nutrition for the fetus. All major body systems are impacted in ways that precisely meet the needs of pregnancy.
Physiological changes during pregnancy include:
1. Enlargement of the uterus, cervix, breasts, and other reproductive organs.
2. Increased blood volume, heart rate, and respiration to support the growing fetus and maternal organs.
3. Hormonal changes like increased progesterone and estrogen from the placenta lead to changes in metabolism, immune function, and other systems throughout the body.
3.physiolosical changes during pregnancyKHUSHBU PATEL
╠²
During pregnancy, the woman's body undergoes many physiological changes to support the growing fetus. The reproductive system changes include increased blood flow and size of the vagina, cervix, and uterus. The uterus grows enormously from about the size of a fist to over 1000 times larger by term. Other systems affected are cardiovascular (increased heart rate and blood volume), respiratory, digestive, urinary, endocrine, and musculoskeletal. Hormonal changes produced by the placenta, such as human chorionic gonadotropin, estrogen, progesterone, prolactin, and human placental lactogen, cause these adaptations to pregnancy.
The document describes several physiological changes that occur in pregnancy. The uterus grows enormously from about 70g to over 1kg by term. This displaces other organs and alters the body's shape and center of gravity. Hormonal changes lead to increased blood volume, cardiac output, and kidney function to support the demands of the fetus. The lungs take on a higher ventilation rate. The digestive system slows while the liver works to support the added metabolic load. Overall, the body undergoes extensive adaptations to accommodate the growing fetus.
Physiological changes during pregnancy can be extensive. The document summarizes several key changes:
1) The uterus grows enormously in size and weight to accommodate the growing fetus. Other genital organs like the cervix and breasts also see significant changes to support pregnancy and birth.
2) Extensive changes occur in many body systems like the cardiovascular, respiratory, urinary and endocrine systems to support the nutritional and oxygen needs of the mother and fetus. This includes increases in blood volume, cardiac output, kidney size and lung capacity.
3) Hormonal changes are also profound, with high levels of progesterone, estrogen and other placental hormones influencing many processes and organs across the body to sustain the pregnancy.
The document outlines the physiological, endocrine, and anatomical changes that occur during pregnancy as adaptations to support fetal development. Key adaptations include increased blood volume, changes in cardiovascular and respiratory function, alterations in renal and gastrointestinal systems, and various hormonal shifts. Understanding these changes is crucial for appropriate management of obstetric clinical problems.
PHYSIOLOGICAL CHANGES IN PREGNANCY.pptxKamauNDavid
╠²
Physiological changes occur throughout pregnancy to support the growth and development of the fetus. The uterus enlarges significantly, increasing in size from about the size of a fist to filling most of the abdomen. Other organs like the breasts and cervix undergo changes to prepare for lactation and birth. There are increases in blood volume and cardiac output to meet the higher demands of the mother and fetus. Hormonal changes influence metabolism and fluid balance. The kidneys increase in size and function to filter wastes and regulate fluid levels despite rising blood pressure. Respiration is also impacted as the growing uterus displaces the diaphragm upwards.
IRH - Physiology of Pregnancy Obstetric.pdfGadzika Gunda
╠²
The document provides an extensive overview of the physiology of pregnancy, discussing the physiological changes that occur in various body systems including the endocrine, cardiovascular, respiratory, urinary, gastrointestinal, and integumentary systems as the body adapts to support a developing fetus. It details hormonal changes, organ adaptations, and the importance of these changes in maintaining pregnancy, nourishing the fetus, and preparing the body for labor and lactation. Additionally, it outlines signs and symptoms of pregnancy, both subjective and objective, along with diagnostic indicators that can confirm pregnancy.
Systemic changes during antenatal period by tanoj patidar msc nursingTanoj Patidar
╠²
Pregnancy induces significant respiratory and gastrointestinal changes due to the enlarging uterus and hormonal effects, leading to altered lung volumes, increased oxygen consumption, and changes in gastrointestinal motility, with common symptoms like dyspnea and heartburn. The endocrine system adapts as the placenta becomes the primary hormone producer, impacting thyroid and adrenal functions, and altering metabolic processes including protein, carbohydrate, and fat metabolism to support fetal growth. Overall, pregnancy results in a complex interplay of anatomical and physiological changes essential for maternal and fetal health.
Physiological changes during pregnancy by Harrison MboheHarrisonMbohe
╠²
The document summarizes many of the physiological changes that occur in a woman's body during pregnancy. Key changes include enlargement and increased blood flow to the uterus, breasts, kidneys and other organs. The cardiovascular system adapts with increased blood volume and heart rate. Hormonal changes impact metabolism, thyroid and cortisol levels. Other changes involve the skin, respiratory and musculoskeletal systems to accommodate the growing fetus.
Physiology of Pregnancy for Undergraduatesthezaira
╠²
The document summarizes the physiological changes that occur throughout a woman's body during pregnancy. Key changes include enlargement and increased blood flow to the uterus, breasts, and major organs. Other changes are weight gain and fluid retention, increased blood volume and altered metabolism to support the growing fetus. The various body systems also adapt to pregnancy through respiratory alkalosis, circulatory adjustments and neurological/hormonal responses.
The document discusses various physiological changes that occur in pregnancy across multiple body systems. The uterus increases dramatically in size from 70g and 10mL non-pregnant to approximately 1100g and 5L by the end of pregnancy. Hormonal changes include increased estrogen, progesterone, hCG, hPL, prolactin, IGF, and decreased hGH levels. This leads to adaptations in various organ systems like increased blood volume by 45%, enlarged heart and increased cardiac output, mild anemia and thrombocytopenia, immunosuppression to tolerate the fetus, and metabolic changes in carbohydrate and fat metabolism. Respiration is also altered to support higher oxygen demands.
Physiological changes during pregnancy include changes in the genital organs, breasts, skin, abdomen, blood, metabolism, cardiovascular and urinary systems. The genital organs like the uterus, cervix and breasts enlarge and the blood volume increases significantly. Metabolism increases to support the growth of the fetus. The heart enlarges and cardiac output increases. Kidney function is enhanced and urinary frequency rises, especially later in pregnancy. Respiration is also impacted with higher oxygen needs.
The document discusses the hormonal regulation of pregnancy. It describes the key hormones produced by the placenta and fetal adrenal gland, including human chorionic gonadotropin, human placental lactogen, progesterone, and estrogen. It explains how these hormones facilitate adaptations in various maternal systems and are responsible for the physiological symptoms of pregnancy. The document also outlines the hormones involved in labor and lactation, including oxytocin and prolactin.
Physiological changes in pregnancy (2).pptsamuellamaryk
╠²
This document summarizes the major physiological adaptations that occur during pregnancy. It discusses changes to volume homeostasis and the cardiovascular, respiratory, urinary, digestive and endocrine systems. Key adaptations include a 30% increase in blood volume, decreased systemic vascular resistance, and increased cardiac output. Hormonal changes like increased progesterone and estrogen help prepare the uterus for growth and childbirth. Pregnancy can be diagnosed through missed periods, physical exams signs, and tests like urine/blood tests to detect hCG and ultrasound exams.
Pregnancy causes many anatomical, physiological, and biomechanical changes in the body to support fetal development and birth. The uterus grows enormously over the course of pregnancy. Other systems like cardiovascular, respiratory, and renal systems also adapt to support increased demands on the mother. Hormonal changes induce physical changes in breasts, skin, ligaments and other tissues. Proper understanding of normal pregnancy changes helps healthcare providers manage common issues and risks.
The document provides an overview of colposcopy and its significance in diagnosing cervical abnormalities such as cervical intraepithelial neoplasia (CIN) and squamous intraepithelial lesion (SIL). It details the history, techniques, necessary equipment, and diagnostic criteria involved in colposcopy, highlighting its advantages and limitations. Recent recommendations and guidelines for managing abnormal cervical smears are also discussed.
The document discusses updates on colposcopy related to HPV and associated conditions, emphasizing the differences in colposcopic features and the complexities encountered during examinations, particularly in the vagina due to multifocal disease. It highlights the importance of proper diagnostic protocols, trained personnel, and future research directions in improving colposcopic practices and patient care. Challenges including misinterpretation of findings and technical issues are addressed, along with the need for advancements in technology for better diagnostic efficiency.
Colposcopy, established in gynecologic practice since 1925, is essential for examining cytologically detected lesions of the cervix, vagina, and vulva, with a growing global presence and training programs. Technological advancements have improved diagnostic capabilities, making colposcopy a preferred screening method for cervical cancer and other conditions. Future research aims to enhance computerized documentation and address the clinical significance of lesions related to HPV, while the demand for quality control and cost-effectiveness in patient care continues to rise.
The document discusses various types of vaginitis and related conditions, detailing specific characteristics and associated pathogens for each type. It covers red punctate vaginitis, white punctate vaginitis, focal vaginitis, follicular cervicitis, and atrophic vaginitis, along with classifications of polyps and HPV-related conditions. The text emphasizes the clinical and pathological distinctions among these conditions, highlighting diagnostic approaches and the significance of HPV infections.
HEALTH CARE PLANNING AND ORGANIZATION OF HEALTH CAREnawaabaquib
╠²
This PowerPoint presentation covers Unit II: Health Care Planning and Organization of Health Care at Various Levels in a simple and easy-to-understand format. It explains importance of health planning in India. The PPT also includes the structure of the health care system at central, state, and local levels. It is useful for GNM ,BSc And Msc Nursing students. This presentation is also helpful for exam preparation .
This presentation covers various classes of anti-infective agents including antifungal, antiviral, antitubercular, antimalarial, urinary tract anti-infectives, and sulphonamides. It provides classification, properties, storage conditions, uses, brand names, and pharmaceutical formulations of each drug. Ideal for pharmacy, nursing, and medical students preparing for pharmacology and medici
The Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC) collaborate closely to produce the globally recognized TNM Classification of Malignant Tumours. Therefore, when discussing the "9th edition of UICC head and neck staging," it's largely in alignment with the updates introduced by the AJCC's Version 9. The UICC's TNM Core Committee finalized the 9th edition of the TNM Classification, with publication anticipated in August 2025.
The key updates for head and neck cancers in the 9th edition (or Version 9) reflect an ongoing effort to improve prognostic accuracy and align staging with contemporary clinical understanding and treatment outcomes. Here are the significant changes, particularly those relevant to head and neck:
* Emphasis on Personalized Care and Prognostic Refinements: The 9th edition reflects a greater focus on personalized care, incorporating refinements that aim to better predict patient outcomes.
* Revised Criteria for Specific Head and Neck Cancers:
* Nasopharyngeal Carcinoma (NPC): This site has seen substantial revisions, as highlighted in the previous response on AJCC updates. Key changes include:
* More precise definition of T3 disease (unequivocal evidence of bone involvement).
* Introduction of advanced radiologic extranodal extension (ENE) as an N3 criterion. This acknowledges the prognostic impact of ENE seen on imaging.
* Subclassification of M1 disease into M1a (3 or fewer metastatic lesions) and M1b (more than 3 lesions) to better stratify prognosis in metastatic settings.
* Redefined Stage Groups for NPC, with T1-2N0-1 now often falling into Stage I, and Stage IV being exclusively for metastatic disease, further subdivided by the M1a/M1b categories.
* Salivary Gland Cancers: Revised criteria based on updated imaging and anatomical features are being incorporated.
* HPV-Related Oropharyngeal Cancers: New staging is introduced for HPV-associated oropharyngeal cancers to better reflect their distinct biological behavior and prognosis, which is generally more favorable than HPV-negative oropharyngeal cancers. This often involves specific considerations for nodal burden.
* Integration of Imaging and Anatomical Features: The updates are grounded in recent evidence, incorporating insights from advanced imaging techniques and a deeper understanding of anatomical spread.
* International Collaboration: These updates are the result of collaborative efforts between the AJCC and UICC, involving input from cancer registries, clinical outcomes data, and disease-specific experts worldwide. The goal is to provide a unified and globally applicable staging system.
* Dynamic Update Process: Similar to the AJCC's shift from "Editions" to "Versions" for specific sites, the UICC is also exploring more flexible ways to share future TNM updates.
In essence, the 9th edition of the UICC staging system for head and neck cancers, particularly in areas like NPC and HPV
Electromyography is basically the study of motor unit activity.
In electromyography, the study of the electrical activity of contracting muscle provides information concerning the structure and function of the motor units.
This presentation by Dr. Bishal Sapkota provides a detailed clinical overview of anaphylaxis, a life-threatening allergic reaction. It covers historical background, clinical criteria for diagnosis, time course, common causes, and multi-system clinical manifestations. Special emphasis is placed on emergency management, including the use of epinephrine, second-line treatments like corticosteroids and antihistamines, and approaches for refractory cases. Ideal for medical professionals, emergency responders, and students in healthcare, this resource draws from authoritative texts such as TintinalliŌĆÖs Emergency Medicine (9th edition) and UpToDate (2025).
Ophthalmic Techniques HSSC-1 | Federal Board Past Paper | 2025 Preparation.pdfazkaimran130
╠²
¤ōś HSSC-1 Ophthalmic Technology | Federal Board Past Paper Solved ¤æü’ĖÅ
Welcome to our channel! In this video, we cover the Federal Board Ophthalmic Techniques Past Paper for HSSC-1, including:
Ō£ģ Multiple Choice Questions (MCQs) ŌĆō Section A (20 Marks)
Ō£ģ Short Questions ŌĆō Section B (50 Marks)
Ō£ģ Long Questions ŌĆō Section C (30 Marks)
¤ōģ Latest Exam Pattern | 2025 Preparation Guide
ŌÅ░ Time Management Tips Included!
This video is perfect for students preparing for HSSC-1 Ophthalmic Technology exams under the Federal Board of Intermediate and Secondary Education (FBISE).
¤öö DonŌĆÖt forget to like, share, and subscribe for more solved papers and exam tips!
#OphthalmicTechnology #FBISE #HSSC1 #PastPaper #MedicalTechnology #OphthalmicTechniques #FederalBoard #MCQs #ShortQuestions #LongQuestions #BoardExam2025
Exomind in General Aesthetics - with June 10, 2025 updateslcadymd1
╠²
Hi. This is Dr. Cady writing. This is the updated presentation compared to the original one given in Hong Kong on June 3rd. The rationale behind the update is my further reflection on the interesting concept of "mental wellness" which has been identified as a treatment target with a modified TMS protocol developed by BTL. It should be clearly noted that this device is definitely approved in the USA for the treatment of depression according to old TMS protocols. The "depression protocol" involves a minimum of 30 treatments, administered over 5 - 6 weeks, with one treatment typically on every weekday (M-F).
In contrast, the "wellness protocol" developed by BTL for this device has been successfully used in a study on "mental wellness" with just FOUR treatments administered, and in the study for food cravings and self control with just SIX treatments administered. Additionally, I demonstrate in this presentation the remarkable power of this TMS device to eliminate depression and anxiety in two patients presented after just two back to back treatments.
It should be clearly noted that this is not an official BTL protocol, nor the position of the company, and the use of this device for mental wellness is not "FDA approved." It is also not FDA approved for the aggressive treatment protocol I share in this presentation. Given that this device is used per physician discretion, and given that the scientific literature supports the idea that the more pulses or treatments delivered in a day increase the effectiveness of the treatment and the rapidity of onset, this aggressive treatment seemed to me to be scientifically valid, and safe. Scrupulous informed consent was obtained from the patients prior to administering the treatments in the manner I have illustrated herein. I am not necessasrily recommending tretments in this manner. But I include them and note them because they reveal, dramatically, the capability of this device to change people's lives with the most serious cases. The impact, therefore, on just "lack of mental wellness" or "food cravings and impulse control is very reasonable.
It is my belief that 4 - 6 treatments in a general aesthetic or "wellness" practice should be sufficient. For the harder cases that a psychiatrist would see, there is some argument that even six treatments, administered with three "couplet" or "paired" treatments, could be remarkably beneficial.
In this presentation, I review the epidemiology of depression, anxiety and the topic of simply being "mentally unwell" while not being necessarily diagnosed with depression or anxiety. It is the lack of mental wellness and addressing it with this helpful modality that is so tremendously exciting.
A rough comparison of the relative treatment potency and effects of the Exomind versus older technology is included, pointing the way toward the logical assumption that, indeed, merely a few treatments (4 - 6) could have significant benefits in our patients.
3. Estogens
ŌĆó Estrone (E1) weak, estrogen of menopause
(type made by peripheral conversion)
ŌĆó Estradiol (E2) strongest, most important (from
Graafian follicles)
ŌĆó Estriol (E3) weakest, produced in large
amounts in pregnancy (x1000).
ŌĆó (E1 = 1OH, E2 =2OH, E3 =3OH)
5. Estrogen Actions - General
Bone:
ŌĆó Stimulates osteoblastic activity
ŌĆó Growth spurt then closure of the epiphysis.
ŌĆó Protects against osteoporosis.
7. Estrogen actions
ŌĆó Coagulation factors increase
ŌĆó Increases binding globulins (SHBG, TBG, CBG)
ŌĆó Breasts: Stimulates duct system , vascularity , fat
ŌĆó In pregnancy stimulates prolactin release but
blocks its action
ŌĆó Endocrinal system
’é¦ Pituitary gland: -ve feedback on FSH, +ve on LH for
ovulation
8. Local effects
ŌĆó Vulva & vagina:
ŌĆō Increase vascularity, size & deposition of fat
ŌĆō More deposition of glycogen: DoderleinŌĆÖs bacilli
forms lactic acid
ŌĆó Cervix: secretion becomes fluid, alkaline +ve
Spinnbarkeit & Fern
ŌĆó Uterus: proliferation & hyperplasia + increased
vascularity
13. Progesterone
ŌĆó Natural hormone
ŌĆó Source:
ŌĆō Corpus luteum
ŌĆō Placenta
ŌĆō Suprarenal glands
ŌĆó Metabolism:
ŌĆ×
ŌĆō bound to SHBG
ŌĆō metabolized in liver
14. Progesterone - actions
ŌĆó Thermogenic (increased BBT)
ŌĆó Stimulates respiration (esp in pregnancy)
ŌĆó Relaxes smooth muscles (e.g. GIT & ureter)
ŌĆó Salt & water loss
ŌĆó Breast: stimulates alveolar system
development in breast
ŌĆó Pituitary: -ve feedback on FSH & LH (inhibition
of ovulation)
15. Progesterone actions
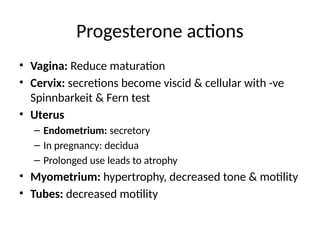
ŌĆó Vagina: Reduce maturation
ŌĆó Cervix: secretions become viscid & cellular with -ve
Spinnbarkeit & Fern test
ŌĆó Uterus
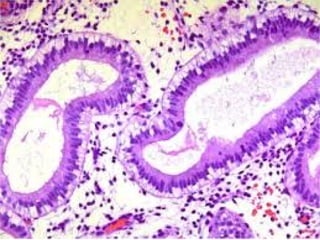
ŌĆō Endometrium: secretory
ŌĆō In pregnancy: decidua
ŌĆō Prolonged use leads to atrophy
ŌĆó Myometrium: hypertrophy, decreased tone & motility
ŌĆó Tubes: decreased motility
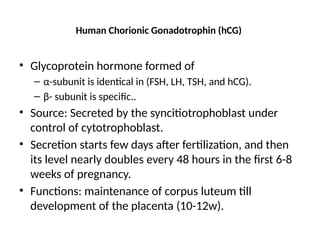
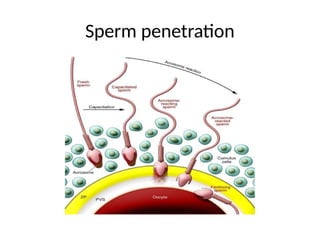
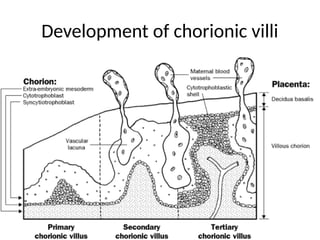
18. Human Chorionic Gonadotrophin (hCG)
ŌĆó Glycoprotein hormone formed of
ŌĆō ╬▒-subunit is identical in (FSH, LH, TSH, and hCG).
ŌĆō ╬▓- subunit is specific..
ŌĆó Source: Secreted by the syncitiotrophoblast under
control of cytotrophoblast.
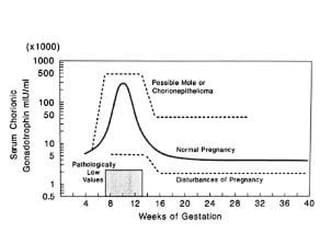
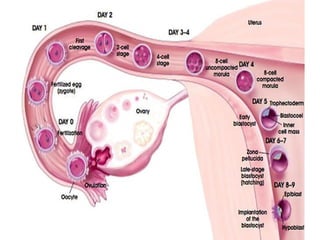
ŌĆó Secretion starts few days after fertilization, and then
its level nearly doubles every 48 hours in the first 6-8
weeks of pregnancy.
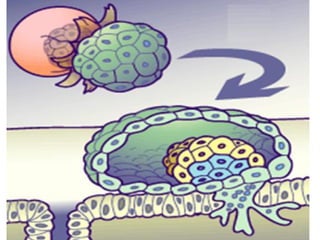
ŌĆó Functions: maintenance of corpus luteum till
development of the placenta (10-12w).
20. HCG levels
ŌĆó Abnormally high:
ŌĆō Vesicular mole, choriocarcinoma, multifetal
pregnancy, Rh isoimmunization, and Down
syndrome.
ŌĆó Abnormally low:
ŌĆō Impending abortion and ectopic pregnancy.
21. HCG measurement
ŌĆó 1) Diagnosis of pregnancy
ŌĆó 2) Differentiation between threatened and
missed abortion.
ŌĆó 3) Diagnosis of ectopic pregnancy.
ŌĆó 4) Trophoblastic tumours.
ŌĆó 5) Down syndrome.
ŌĆó 6) Some ovarian tumors.
22. Human placental lactogen (HPL)
ŌĆó Nature: Protein hormone formed of 191 amino acids. (90%
similarity to GH).
ŌĆó Source: secreted from the syncytiotrophobtasts. HPL starts to
appear since early pregnancy and steadily increases till before
labor.
ŌĆó Functions:
ŌĆō a. Somatotropic , mamotropic & Lactogenic, Leutotropic.
ŌĆō b. Anti-insulin
ŌĆō c. Lipolytic
ŌĆó Significance: HPL levels are high in twin gestation, Rh
isoimmunization, diabetes and prolonged fasting; while it is low
in all cases with placental insufficiency.
23. Maternal adaptation to pregnancy
ŌĆó Lower genital tract (vulva / vagina / cervix):
ŌĆō Increased vascularity (violet color of cervix, vagina, vulva
Chadwick's sign.
ŌĆō Softening of the vaginal portion of the cervix (Goodell's
sign.)
ŌĆō Increased glycogen of the vagina, vaginal acidity.
ŌĆó Mucous plug of cervix .
ŌĆó Cervical ripening: at the end of pregnancy due to
edema and decreased collagen caused by
prostaglandins.
24. Uterus
ŌĆó Size: weight increases from 50 grams to reach
1000 grams at term.
ŌĆó Shape: pyriform then globular till 16 weeks
then it becomes ovoid.
ŌĆó Position: Dextrorotation
ŌĆó Myometrium: Hypertrophy
25. Uterine activity
ŌĆó Painless contractions
ŌĆō Detected by bimanual examination early in
pregnancy = Palmer sign.
ŌĆō Detected by abdominal examination late in
pregnancy = Braxton Hicks contractions.
ŌĆó Painful intermittent contractions near term =
ŌĆÜ
False labor pains
26. -
Lower uterine segment (LUS)
ŌĆó Starts to be formed from the 4th month to
reach 10cm at term.
ŌĆó It is formed from isthmus & lower 1/2 inch of
the body due to enlargement of uterine
contents and contraction & retraction of UUS.
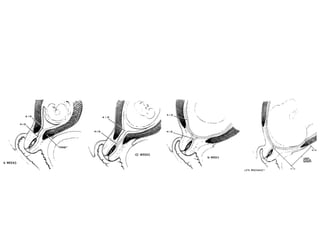
28. Urinary system
ŌĆó Urethra: Stress incontinence
ŌĆó Urinary bladder: Frequency due to; Pressure by
uterus & by head in late pregnancy and also
due to hyperemia & hyperplasia of the muscles
& epithelium.
ŌĆó Ureters : Dilation (Atony by progesterone,
Hypertrophy of lower end, pressure of the
uterus on the ureter. (more on the right ureter
due to dextrorotation of the uterus)
29. ŌĆó Kidneys: GFR and renal blood flow rise. A
serum creatinine of 1.0 mg/dL in a pregnant
woman probably reflects significant renal
insufficiency.
ŌĆó Tubular reabsorption: of glucose, and amino
acids are decreased, which can lead to mild
glucosuria (Renal glycosuria) and
aminoaciduria.
30. GIT
ŌĆó Emesis gravidarum: "morning sicknessŌĆØ
ŌĆó Oropharyngeal changes: pregnancy epulis,
gingivitis, ptyalism, and changes in taste.
ŌĆó Stomach:
ŌĆō a) Gastrointestinal reflux
ŌĆō b) Gastric aspiration
ŌĆō c) Decreased gastric acidity: This may interfere with iron
absorption, leading to anemia.
ŌĆó Intestine
ŌĆō a) Abdominal bloating and constipation
ŌĆō b) Hemorrhoids: due to constipation and increased local
venous pressure.
31. Liver
ŌĆó Liver, Gallbladder, and Pancreas:
ŌĆō Liver function tests:
ŌĆó aminotransferase, bilirubin, and bile acid: normal
ŌĆō Serum albumin: reduced.
ŌĆō Lipids and alkaline phosphatase levels: increased.
ŌĆó Gallbladder: liable to gallstones
32. Blood
ŌĆó 1) Blood volume: Expansion 40 % above baseline.
ŌĆō a) Plasma volume: is increased 30 to 50 % (increased
plasma renin activity and reduced atrial natriuretic
peptide levels)
ŌĆō b) Red cell mass: increased 20 to 30 % with iron
supplements, 15 to 20 % without
ŌĆō c) Physiologic anemia
ŌĆó 2) WBCs: Leukocytosis esp in labour
ŌĆó 3) Platelet count: decrease (gestational
thrombocytopenia) - hemodilution
33. Coagulation
ŌĆó Hypercoagulable state due to:
a) Factors I, II, V, VII, VIII, X, and Xll: increase
(Increased fibrinogen (up to 600 mg %)).
b) Resistance to activated protein C: increases
c) Protein S: decreases
d) D-dimer levels: are increased
34. Heart
ŌĆó Lateral displacement of the apex
ŌĆó Functional systolic murmurs: due to
hyperdynamic circulation of the dilutional
anemia.
ŌĆó Cardiac output: rises to a peak at 28 to 34
weeks, which is 30-50 %
35. Vessels
ŌĆó Vascular resistance and blood pressure: blood pressure
(BP) typically fall early in gestation.
ŌĆō a) Uteroplacental circulation: high-flow, low-resistance circuit
ŌĆō b) Systemic vasodilatation: decreased vascular responsiveness
to the pressor effects of angiotensin II and norepinephrine.
ŌĆó Supine hypotension syndrome.
Veins: varicose veins, ankle edema, and piles due to:
pressure by the uterus on the pelvic veins, progesterone
effect and increased blood volume.
36. Respiratory
ŌĆó Increased blood flow to the nasopharynx may cause
congestion.
ŌĆó Functional changes: Progesterone increases depth not
rate. PaO2 increases and PaCO2 decreases during
pregnancy.
ŌĆó Dyspnea: Progesterone-induced hyperventilation and
limitation of movement of the diaphragm in late
pregnancy causes dyspnea.
37. Skin
ŌĆó Pigmentation: increase Melanocyte Stimulating
Hormone and estrogen, appears in the:
ŌĆō a) Chloasma gravidarum
ŌĆō b) Linea Nigra
ŌĆó 2) Striae gravidarum
ŌĆó 3) Increased vascularity of the skin & mucous
membranes: Sensation of heat, sweating, nasal
congestion and even epistaxis. Spidery veins on
abdominal wall and palmar erythema may occur.
ŌĆó 4) Loss of hair: is a common complaint that occurs
during pregnancy.
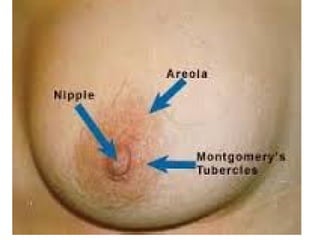
43. Breast
ŌĆó 1) Increased size and vascularity (warm, tense
and tender).
ŌĆó 2) Increased pigmentation of the nipple and
areola. 2ry areola appears (light pigmentation
around the 1ry areola).
ŌĆó 3) Montegomery tubercles (MT): appear on
the areola (dilated sebaceous glands).
ŌĆó 4) Colostrum-like fluid: is expressed at the end
of the 4th month.
46. Endocrine
ŌĆó 1) Pituitary:
ŌĆō Prolactin: increases throughout pregnancy, reaching
a peak at delivery.
ŌĆō FSH, LH decrease
ŌĆó 2) Thyroid :
ŌĆō TBG rises
ŌĆō Increase in total T4 and T3, but not free T4 and T3
concentrations.
ŌĆó 3) Supra renal :
ŌĆō a) Aldosterone: increases
ŌĆō b) Cortisol: increases
47. Metabolic
ŌĆó 1) Carbohydrate metabolism:
ŌĆō Decrease fasting glucose
ŌĆō Maternal insulin resistance
ŌĆō Maternal glucose homeostasis shows transient
maternal hyperglycemia after meals due to
increasing insulin resistance and transient
hypoglycemia between meals and at night due to
the continuous fetal draw.
48. ŌĆó Fat metabolism : increased Serum
triglycerides, cholesterol.
ŌĆó Protein Metabolism : anabolic state
ŌĆó Minerals & Vitamins: requirements of iron,
calcium, phosphorus, iodides and vitamins are
increased.
ŌĆó Water: Salt and water retention