The document discusses congenital anomalies, detailing their definitions, prevalence, causes (including genetic and environmental factors), and specific types of defects. It highlights the importance of genetic counseling and preventive measures, such as avoiding late pregnancies, consanguinity, and promoting maternal health. Various congenital conditions are listed, emphasizing the need for early detection and management strategies.
This document discusses congenital anomalies, including definitions, global incidence rates, common types, causes, risk factors, diagnostic methods, and preventive measures. It notes that congenital anomalies can be caused by genetic or environmental factors and include defects of the central nervous system, heart, gastrointestinal system, genitourinary system, limbs, and metabolic disorders. The document also outlines methods for genetic counseling and strategies to prevent congenital anomalies, such as promoting prenatal health, avoiding teratogens, and utilizing screening and diagnostic tests.
Maternal prenatal and genetic influence on defects and diseases (Unit -II)BHAVESH SINGH
╠²
This document discusses maternal and genetic influences on birth defects and diseases. It defines key terms and classifications of birth defects. The main causes of congenital anomalies are described as genetic factors like chromosomal/single-gene defects, environmental teratogens, and multifactorial origins. Specific genetic conditions, teratogens (such as alcohol, thalidomide), infections, and maternal disorders that can cause birth defects are explained. Prevention strategies include preconception counseling and folic acid supplementation during pregnancy.
This document discusses maternal and genetic factors that can influence birth defects and diseases. It covers several key topics:
1) Causes of congenital anomalies include genetic factors like chromosomal abnormalities and single-gene defects, as well as environmental teratogens. Common teratogens discussed are alcohol, thalidomide, infections, and ionizing radiation.
2) Genetic factors that can cause birth defects are chromosomal abnormalities and single-gene mutations. Chromosomal defects can cause syndromes like Down syndrome.
3) Other influences discussed are maternal age, nutrition, and consanguinity. Advanced maternal age increases risks of genetic defects, while good prenatal nutrition may lower risks of allergies and atopic
Congenital anomalies include structural, functional, and biochemical disorders present at birth. The global incidence is 30-70 per 1000 live births, and in India it is 2.5-4%. Genetic and environmental factors can cause congenital anomalies. Genetic counseling provides information to families about genetic disorders and helps prevent transmission of hereditary conditions. Measures to prevent congenital anomalies include promoting pre-pregnancy health, immunizations, avoiding teratogens and infections during pregnancy, and prenatal screening and diagnosis.
The document discusses congenital anomalies, including their types, causes, and incidence rates, highlighting structural defects prevalent at birth. It identifies genetic and environmental factors contributing to these anomalies and emphasizes the importance of prenatal screening and genetic counseling. Recommendations for prevention involve addressing maternal health, discouraging consanguineous marriages, and raising public awareness about risk factors.
The document discusses maternal prenatal and genetic influences on congenital anomalies, detailing the definitions and classifications of defects, their causesŌĆöincluding genetic, environmental, and multifactorial originsŌĆöand factors such as maternal infections and age. It outlines prevention strategies including preconception visits, lifestyle modifications, and the importance of folic acid during pregnancy. Additionally, it touches on how dietary choices during pregnancy can impact allergy risks in offspring.
The document discusses various birth defects including:
1. Atavism, polydactyly, syndactyly, gigantism, and cleft lip which are abnormalities in development.
2. Terms used to describe diseases such as signs, symptoms, and etiology.
3. Types of anomalies including malformations, disruptions, deformations, and syndromes.
4. Various congenital defects and birth defects are discussed such as clubfoot, torticollis, Down syndrome, fetal alcohol syndrome, muscular dystrophy, spina bifida, and cerebral palsy. Environmental factors that can influence birth defects are also summarized.
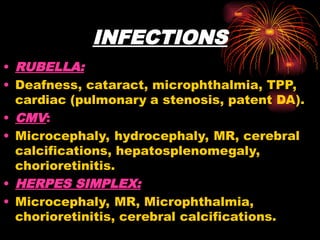
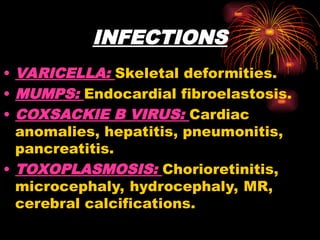
This document discusses congenital anomalies (structural abnormalities present at birth) including their causes, types, and examples. It notes that around 3% of liveborn infants have major anomalies, which can be genetic, environmental, or multifactorial in origin. During the first two weeks after conception, teratogens usually have no effect, but between weeks 3-8 (organogenesis period) they can cause major anomalies, and after week 9 functional abnormalities. Causes discussed include genetic factors, infections like rubella and toxoplasmosis, radiation, chemicals/drugs, maternal diseases, and nutritional deficiencies. The document provides examples of syndromes and specific anomalies affecting various body systems. Prevention emphasizes good prenatal care, iod
Congenital anomalies are defects present at birth that are caused by genetic and environmental factors. Some anomalies are obvious at birth like cleft lip, while others manifest later. Major anomalies require surgery, while minor ones have no functional implications. The most common anomalies in India are central nervous system and musculoskeletal abnormalities. Risk factors include advanced maternal age, consanguinity, and malnutrition. Nurses play an important role in educating families on prevention, screening, and caring for children with congenital anomalies.
The document discusses the maternal prenatal and genetic influences on congenital anomalies, detailing the definitions, classifications, and causes of birth defects, including genetic and environmental factors. It highlights the role of teratogens, maternal infections, and genetic disorders in the development of congenital anomalies and provides prevention strategies, such as prenatal nutrition and reducing exposure to harmful substances. Additionally, it addresses factors influencing infertility in both males and females and emphasizes the importance of maternal age and genetic counseling.
Common congenital anomalies by Dr Amber MushtaqAmberMushtaq4
╠²
The document discusses congenital anomalies, defining them as biochemical, structural, and functional disorders present at birth, with a focus on structural defects. It outlines the global and Indian incidence rates, the most common types such as CNS abnormalities, and various risk factors including genetic and environmental causes. Additionally, it covers diagnostic approaches, common congenital anomalies across different systems, prevention strategies, and the role of genetic counseling.
Congenital anomalies, or birth defects, can be caused by genetic or environmental factors and may affect structures formed at birth. The document discusses the causes, prevalence, types and diagnosis of congenital anomalies. Genetic factors include chromosomal abnormalities and gene mutations, while environmental factors comprise infectious agents, radiation, chemicals, and maternal diseases. Common anomalies include Down syndrome and spina bifida. Prenatal screening and diagnosis methods help detect anomalies during pregnancy.
Approach to a newborn with multiple congenital anomalyNitin Das
╠²
This document discusses the approach to evaluating a newborn with multiple congenital anomalies. It defines different types of anomalies and lists common syndromes. It emphasizes obtaining a thorough history of the pregnancy, birth and physical exam findings. A workup may include imaging, labs, genetic testing and specialty referrals to identify a diagnosis and prognosis. The case presented has unilateral anotia, facial palsy, congenital heart disease, scoliosis and absent rib, consistent with possible Goldenhar or cardiofacial syndrome.
Congenital anomalies are conditions present at birth, often due to genetic, environmental, or unknown factors. These disorders may manifest as structural deformities and can range from minor to severe, impacting various body systems. Prevention and early screening are crucial for improving outcomes, and some congenital disorders can be effectively treated with medical or surgical interventions.
This document provides an overview of congenital malformations, including definitions of key terms like malformation, disruption, and deformation. It discusses the etiology and pathogenesis of malformations, highlighting factors like genetics, environment, and timing of insults during development. Selected organ malformations and chromosomal disorders are reviewed, like Down syndrome, Edward syndrome, Patau syndrome, and Turner syndrome. The document aims to enhance understanding of the processes that can result in structural defects present at birth or later in life.
Congenital abnormalities are significant contributors to neonatal and childhood mortality, with about 240,000 newborns dying annually from birth defects. These abnormalities can arise from genetic, environmental, and socio-economic factors, with many cases remaining unexplained. Prevention strategies include discouraging consanguinity, promoting maternal health, and ensuring proper antenatal care.
Teratology is the study of congenital abnormalities and other developmental disorders in both humans and other organisms, emphasizing the impact of environmental agents, known as teratogens, which can cause birth defects. The document outlines the types of teratogens, their mechanisms, and the principles of teratology, including factors like genotype, developmental stage, and exposure duration. It also discusses classification, incidence, causative factors, diagnostic methods, and preventive measures for congenital anomalies.
The document discusses dysmorphology, its definition, the impact of birth defects on health, and the classification and causes of congenital anomalies. It emphasizes the importance of a systematic examination and genetic counseling to aid diagnosis and management of patients with dysmorphic features. Key concepts include types of morphogenesis errors, identification of syndromes and associations, and the role of family history in assessing genetic risks.
The document discusses several congenital malformations including anencephaly, microcephaly, megalencephaly, septo-optic dysplasia, diastomatomyelia, polymicrogyria, encephalocele, and spina bifida. It provides details on causes, clinical presentations, diagnostic evaluations, and management for each condition. Anencephaly is a neural tube defect where the brain and skull are absent. Microcephaly is a small head size due to abnormal brain development. Megalencephaly is an abnormally large brain. Septo-optic dysplasia involves optic nerve and pituitary abnormalities. Spina bifida is an incomplete closing of the spine that can range from mild
Congenital anomalies are structural defects present at birth, which can stem from intrinsic errors in development (malformations) or extrinsic factors (disruptions, deformations). Their etiologies can be genetic, environmental, or multifactorial, and the timing of prenatal exposure to harmful agents significantly influences the type and extent of anomalies. Understanding these factors is crucial, as the consequences can vary based on when the insult occurs during gestation.
Prevalence of Congenital Malformations in Newborns Delivered in a Rural Medic...iosrjce
╠²
A study conducted at B.S. Medical College in West Bengal found that the prevalence of congenital malformations among 14,079 newborns was 2.3%, with cardiovascular, musculoskeletal, and genitourinary systems being most affected. The research identified various maternal risk factors, such as age and consanguinity, and highlighted the importance of early prevention and intervention strategies. This data adds to the understanding of congenital abnormalities in the region and underlines the need for improved healthcare planning and education.
This document provides information on medical genetics and genetic diseases. It discusses what medical genetics is, including the study of inheritance of diseases and mapping disease genes. It also discusses why medical genetics is important, covering topics like genetic diseases making up a large percentage of pediatric diseases. The document then discusses principles of dysmorphology, including definitions of anomalies, syndromes, sequences, and factors that can affect the expression of disease-causing genes. Overall, the document provides a high-level overview of key concepts in medical genetics.
Perinatal mortality encompasses late fetal deaths and early neonatal deaths, with significant disparities between developed (under 10 per 1000) and developing countries like India (36 per 1000). Key factors for increased perinatal mortality include maternal age, socioeconomic status, and obstetric complications, while solutions lie in comprehensive prenatal care and early detection of at-risk pregnancies. Congenital malformations, as well as birth trauma, play substantial roles in mortality, with essential preventive measures focusing on education and effective healthcare access.
An approach to a child with microcephaly involves obtaining a thorough history and physical examination to help identify potential genetic or acquired causes. Key parts of the evaluation include measuring head circumference, examining for dysmorphic features, assessing growth, and looking for signs of an underlying condition like a genetic syndrome or intrauterine infection. Investigations like chromosomal analysis, metabolic testing, imaging and infectious workup aim to establish a diagnosis to guide prognosis and management.
The document discusses congenital malformations, including:
- Types of congenital anomalies like major anomalies that interfere with normal functioning and minor anomalies that have only cosmetic significance.
- Causes of congenital anomalies which can be genetic like chromosomal or single gene defects, or non-genetic like drugs, infections, or maternal illness.
- Stages of normal morphogenesis and how abnormalities can occur if stages are incomplete, take an aberrant form, or functional defects develop. Timing of different malformations is outlined.
- Specific genetic syndromes are mentioned as causes for different malformation patterns. Deletion 22q11 syndrome is discussed in detail as a common microdeletion syndrome.
The document discusses various birth defects including:
1. Atavism, polydactyly, syndactyly, gigantism, and cleft lip which are abnormalities in development.
2. Terms used to describe diseases such as signs, symptoms, and etiology.
3. Types of anomalies including malformations, disruptions, deformations, and syndromes.
4. Various congenital defects and birth defects are discussed such as clubfoot, torticollis, Down syndrome, fetal alcohol syndrome, muscular dystrophy, spina bifida, and cerebral palsy. Environmental factors that can influence birth defects are also summarized.
This document discusses congenital anomalies (structural abnormalities present at birth) including their causes, types, and examples. It notes that around 3% of liveborn infants have major anomalies, which can be genetic, environmental, or multifactorial in origin. During the first two weeks after conception, teratogens usually have no effect, but between weeks 3-8 (organogenesis period) they can cause major anomalies, and after week 9 functional abnormalities. Causes discussed include genetic factors, infections like rubella and toxoplasmosis, radiation, chemicals/drugs, maternal diseases, and nutritional deficiencies. The document provides examples of syndromes and specific anomalies affecting various body systems. Prevention emphasizes good prenatal care, iod
Congenital anomalies are defects present at birth that are caused by genetic and environmental factors. Some anomalies are obvious at birth like cleft lip, while others manifest later. Major anomalies require surgery, while minor ones have no functional implications. The most common anomalies in India are central nervous system and musculoskeletal abnormalities. Risk factors include advanced maternal age, consanguinity, and malnutrition. Nurses play an important role in educating families on prevention, screening, and caring for children with congenital anomalies.
The document discusses the maternal prenatal and genetic influences on congenital anomalies, detailing the definitions, classifications, and causes of birth defects, including genetic and environmental factors. It highlights the role of teratogens, maternal infections, and genetic disorders in the development of congenital anomalies and provides prevention strategies, such as prenatal nutrition and reducing exposure to harmful substances. Additionally, it addresses factors influencing infertility in both males and females and emphasizes the importance of maternal age and genetic counseling.
Common congenital anomalies by Dr Amber MushtaqAmberMushtaq4
╠²
The document discusses congenital anomalies, defining them as biochemical, structural, and functional disorders present at birth, with a focus on structural defects. It outlines the global and Indian incidence rates, the most common types such as CNS abnormalities, and various risk factors including genetic and environmental causes. Additionally, it covers diagnostic approaches, common congenital anomalies across different systems, prevention strategies, and the role of genetic counseling.
Congenital anomalies, or birth defects, can be caused by genetic or environmental factors and may affect structures formed at birth. The document discusses the causes, prevalence, types and diagnosis of congenital anomalies. Genetic factors include chromosomal abnormalities and gene mutations, while environmental factors comprise infectious agents, radiation, chemicals, and maternal diseases. Common anomalies include Down syndrome and spina bifida. Prenatal screening and diagnosis methods help detect anomalies during pregnancy.
Approach to a newborn with multiple congenital anomalyNitin Das
╠²
This document discusses the approach to evaluating a newborn with multiple congenital anomalies. It defines different types of anomalies and lists common syndromes. It emphasizes obtaining a thorough history of the pregnancy, birth and physical exam findings. A workup may include imaging, labs, genetic testing and specialty referrals to identify a diagnosis and prognosis. The case presented has unilateral anotia, facial palsy, congenital heart disease, scoliosis and absent rib, consistent with possible Goldenhar or cardiofacial syndrome.
Congenital anomalies are conditions present at birth, often due to genetic, environmental, or unknown factors. These disorders may manifest as structural deformities and can range from minor to severe, impacting various body systems. Prevention and early screening are crucial for improving outcomes, and some congenital disorders can be effectively treated with medical or surgical interventions.
This document provides an overview of congenital malformations, including definitions of key terms like malformation, disruption, and deformation. It discusses the etiology and pathogenesis of malformations, highlighting factors like genetics, environment, and timing of insults during development. Selected organ malformations and chromosomal disorders are reviewed, like Down syndrome, Edward syndrome, Patau syndrome, and Turner syndrome. The document aims to enhance understanding of the processes that can result in structural defects present at birth or later in life.
Congenital abnormalities are significant contributors to neonatal and childhood mortality, with about 240,000 newborns dying annually from birth defects. These abnormalities can arise from genetic, environmental, and socio-economic factors, with many cases remaining unexplained. Prevention strategies include discouraging consanguinity, promoting maternal health, and ensuring proper antenatal care.
Teratology is the study of congenital abnormalities and other developmental disorders in both humans and other organisms, emphasizing the impact of environmental agents, known as teratogens, which can cause birth defects. The document outlines the types of teratogens, their mechanisms, and the principles of teratology, including factors like genotype, developmental stage, and exposure duration. It also discusses classification, incidence, causative factors, diagnostic methods, and preventive measures for congenital anomalies.
The document discusses dysmorphology, its definition, the impact of birth defects on health, and the classification and causes of congenital anomalies. It emphasizes the importance of a systematic examination and genetic counseling to aid diagnosis and management of patients with dysmorphic features. Key concepts include types of morphogenesis errors, identification of syndromes and associations, and the role of family history in assessing genetic risks.
The document discusses several congenital malformations including anencephaly, microcephaly, megalencephaly, septo-optic dysplasia, diastomatomyelia, polymicrogyria, encephalocele, and spina bifida. It provides details on causes, clinical presentations, diagnostic evaluations, and management for each condition. Anencephaly is a neural tube defect where the brain and skull are absent. Microcephaly is a small head size due to abnormal brain development. Megalencephaly is an abnormally large brain. Septo-optic dysplasia involves optic nerve and pituitary abnormalities. Spina bifida is an incomplete closing of the spine that can range from mild
Congenital anomalies are structural defects present at birth, which can stem from intrinsic errors in development (malformations) or extrinsic factors (disruptions, deformations). Their etiologies can be genetic, environmental, or multifactorial, and the timing of prenatal exposure to harmful agents significantly influences the type and extent of anomalies. Understanding these factors is crucial, as the consequences can vary based on when the insult occurs during gestation.
Prevalence of Congenital Malformations in Newborns Delivered in a Rural Medic...iosrjce
╠²
A study conducted at B.S. Medical College in West Bengal found that the prevalence of congenital malformations among 14,079 newborns was 2.3%, with cardiovascular, musculoskeletal, and genitourinary systems being most affected. The research identified various maternal risk factors, such as age and consanguinity, and highlighted the importance of early prevention and intervention strategies. This data adds to the understanding of congenital abnormalities in the region and underlines the need for improved healthcare planning and education.
This document provides information on medical genetics and genetic diseases. It discusses what medical genetics is, including the study of inheritance of diseases and mapping disease genes. It also discusses why medical genetics is important, covering topics like genetic diseases making up a large percentage of pediatric diseases. The document then discusses principles of dysmorphology, including definitions of anomalies, syndromes, sequences, and factors that can affect the expression of disease-causing genes. Overall, the document provides a high-level overview of key concepts in medical genetics.
Perinatal mortality encompasses late fetal deaths and early neonatal deaths, with significant disparities between developed (under 10 per 1000) and developing countries like India (36 per 1000). Key factors for increased perinatal mortality include maternal age, socioeconomic status, and obstetric complications, while solutions lie in comprehensive prenatal care and early detection of at-risk pregnancies. Congenital malformations, as well as birth trauma, play substantial roles in mortality, with essential preventive measures focusing on education and effective healthcare access.
An approach to a child with microcephaly involves obtaining a thorough history and physical examination to help identify potential genetic or acquired causes. Key parts of the evaluation include measuring head circumference, examining for dysmorphic features, assessing growth, and looking for signs of an underlying condition like a genetic syndrome or intrauterine infection. Investigations like chromosomal analysis, metabolic testing, imaging and infectious workup aim to establish a diagnosis to guide prognosis and management.
The document discusses congenital malformations, including:
- Types of congenital anomalies like major anomalies that interfere with normal functioning and minor anomalies that have only cosmetic significance.
- Causes of congenital anomalies which can be genetic like chromosomal or single gene defects, or non-genetic like drugs, infections, or maternal illness.
- Stages of normal morphogenesis and how abnormalities can occur if stages are incomplete, take an aberrant form, or functional defects develop. Timing of different malformations is outlined.
- Specific genetic syndromes are mentioned as causes for different malformation patterns. Deletion 22q11 syndrome is discussed in detail as a common microdeletion syndrome.
The document provides an overview of colposcopy and its significance in diagnosing cervical abnormalities such as cervical intraepithelial neoplasia (CIN) and squamous intraepithelial lesion (SIL). It details the history, techniques, necessary equipment, and diagnostic criteria involved in colposcopy, highlighting its advantages and limitations. Recent recommendations and guidelines for managing abnormal cervical smears are also discussed.
The document discusses updates on colposcopy related to HPV and associated conditions, emphasizing the differences in colposcopic features and the complexities encountered during examinations, particularly in the vagina due to multifocal disease. It highlights the importance of proper diagnostic protocols, trained personnel, and future research directions in improving colposcopic practices and patient care. Challenges including misinterpretation of findings and technical issues are addressed, along with the need for advancements in technology for better diagnostic efficiency.
Colposcopy, established in gynecologic practice since 1925, is essential for examining cytologically detected lesions of the cervix, vagina, and vulva, with a growing global presence and training programs. Technological advancements have improved diagnostic capabilities, making colposcopy a preferred screening method for cervical cancer and other conditions. Future research aims to enhance computerized documentation and address the clinical significance of lesions related to HPV, while the demand for quality control and cost-effectiveness in patient care continues to rise.
The document discusses various types of vaginitis and related conditions, detailing specific characteristics and associated pathogens for each type. It covers red punctate vaginitis, white punctate vaginitis, focal vaginitis, follicular cervicitis, and atrophic vaginitis, along with classifications of polyps and HPV-related conditions. The text emphasizes the clinical and pathological distinctions among these conditions, highlighting diagnostic approaches and the significance of HPV infections.
Whooping cough for BSC 5th sem community health nursing..
This includes
Introduction
Definition
Incidence
Incubation period
Causes
Clinical manifestations
Diagnostic evaluation
Treatment
Prevention
Complications
Of whooping cough....
Cell Injuri. pathophpysiology sem- II B PharmacypptxUmeshMali25
╠²
This presentation provides a comprehensive overview of cell injury, a fundamental concept in pathology. It covers the causes, types (reversible and irreversible), mechanisms of injury (including hypoxia, free radicals, and chemical agents), and the morphological and biochemical changes that occur during cell injury. The slides are ideal for medical, pharmacy, and life sciences students preparing for pathology coursework or exams.
Ratricharya according to ayurveda along with day and night pattern in various...DR DHARMENDRA BINJHWAR
╠²
This slide are more importents for ayurveda students and teachers because i have mentioned in this slide night time routine in ayurveda the ancient science of India along with day and night pattern in various counteries within in one ppt. thanks for watching i will be greatful for your suggestion and feedback... please like share and suppourt
HEALTH CARE PLANNING AND ORGANIZATION OF HEALTH CAREnawaabaquib
╠²
This PowerPoint presentation covers Unit II: Health Care Planning and Organization of Health Care at Various Levels in a simple and easy-to-understand format. It explains importance of health planning in India. The PPT also includes the structure of the health care system at central, state, and local levels. It is useful for GNM ,BSc And Msc Nursing students. This presentation is also helpful for exam preparation .
This presentation by Dr. Bishal Sapkota provides a detailed clinical overview of anaphylaxis, a life-threatening allergic reaction. It covers historical background, clinical criteria for diagnosis, time course, common causes, and multi-system clinical manifestations. Special emphasis is placed on emergency management, including the use of epinephrine, second-line treatments like corticosteroids and antihistamines, and approaches for refractory cases. Ideal for medical professionals, emergency responders, and students in healthcare, this resource draws from authoritative texts such as TintinalliŌĆÖs Emergency Medicine (9th edition) and UpToDate (2025).
Biomechamnics of Wrist and Hand complex.Preet Mehta
╠²
This file includes the basic and important features on the topic of biomechanics of wrist joint includes wrist and hand complex anatomy and kinematics of each motion making it simple and understandable for physiotherapy students. Along with biomechanics it also covers an important functional part that is Prehension : Types, muscles and uses of each grips.
Growth hormone (GH) secretion from anterior pituitary is regulated by the hypothalamus and the mediators of GH actions. Major regulatory factors include GH releasing hormone (GHRH), somatostatin (SRIF), GH releasing peptide (ghrerin) and insulin-like growth factor (IGF-I).
Electromyography is basically the study of motor unit activity.
In electromyography, the study of the electrical activity of contracting muscle provides information concerning the structure and function of the motor units.
Definition of Teaching:
ŌĆ£Teaching is a form of interpersonal influence aim at changing the behavior potential of another personŌĆØ.
Nature and Characteristics of Teaching:
’āś Teaching is giving information.
’āś Teaching is causing to learn.
’āś Teaching is a matter of helping the child to respond to his environment in an effective manner.
’āś Teaching is helping a child to adjust himself to his environment.
’āś Teaching is stimulation and encouragement.
’āś Teaching is guidance.
’āś Teaching is Training the emotions of the child.
’āś Teaching is a mean of preparation.
’āś Teaching is an art and science.
General Theory of Teaching:
The General Theory of Teaching, also known as the "Theory of Teaching" or "General Theory of Instruction," is a comprehensive framework that outlines the fundamental principles and processes of teaching.
Benefits of the General Theory of Teaching:
ŌĆó Improved Student Learning
ŌĆó Increased Teacher Efficacy
ŌĆó Enhanced Teacher Professional Development
ŌĆó Better Student Engagement
CONCLUSION
ŌĆó Teaching theory is prescriptive.
ŌĆó Teachers and pupils are the major variables of teaching theory.
ŌĆó It is narrow and specific.
ŌĆó It is based upon learning theory, learning conditions and learning components.
ŌĆó While learning theory are formulated by conducting experiments on animals teaching theory is developed by dealing with human subjects in normal situations.
ŌĆó It is concerned with effective learning and development of pupils.
Learning is a complex and multifaceted process that involves the acquisition, processing, and retention of knowledge, skills, and attitudes.
The relatively permanent change in a person's knowledge or behavior due to experience.
Characteristics of Learning:
ŌĆó Learning is Growth.
ŌĆó Learning is adjustment.
ŌĆó Learning is purposeful.
ŌĆó Learning is intelligent.
ŌĆó Learning is active.
ŌĆó Learning is both individual and social.
ŌĆó Learning is the product of the environment.
ŌĆó Learning is experience.
Learning Theory: Learning theory refers to the body of knowledge that explains how people learn and acquire new knowledge, skills, and attitudes.
Types of Teaching Theory:
1.Formal Theory of Teaching
ŌĆó Meutic Theory of teaching.
ŌĆó Communication theory of teaching.
ŌĆó Moulding theory of teaching.
ŌĆó The mutual enquiry theory.
2.Descriptive theory of teaching
ŌĆó Theories of instruction
ŌĆó Prescriptive theory of teaching
3.Normative theory of teaching
ŌĆó Cognitive theory of teaching
ŌĆó Theory of teacher behaviour
ŌĆó Psychological theory of teaching
ŌĆó General theory of teaching
FORMAL THEORY OF TEACHING
Formal theory of teaching is also known as philosophical theory. The theory which is based upon certain logic, certain metaphysical, epistemological assumptions and propositions is known as formal theory of teaching.
1.Meutic Theory of Teaching:
ŌĆó This theory conceives that teaching process helps to recollect or unfold that knowledge with questioning techniques.
ŌĆó The SocraticŌĆÖs method is an essential for this theory.
ŌĆó The heredity plays an import
3. TERMINOLOGY
ŌĆó Congenital: exists since birth.
ŌĆó Malformation: faulty development.
ŌĆó Anomaly: deviation from normal.
ŌĆó Deformity: alteration in structure or
shape of previous normally formed
part.
ŌĆó Syndrome: pattern of malformations of
the same cause.
ŌĆó Association: anomalies occurring
together more frequently than
expected by chance.
8. GENETIC CAUSES
ŌĆó 2-POLYGENIC INHERITANCE:
’āśThe inheritance of single phenotypic
feature as result of the effects of
many genes.
’āśThere are racial variations.
’āśEnvironmental factors play a role.
’āśFor example, cleft lip and plate,
anencephaly, meningomyelocele.
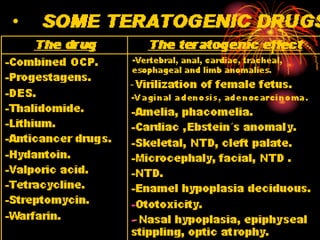
10. NON GENETIC CAUSES
EXPOSURE TO TERATOGENICS
ŌĆó TERATOGENIC AGENT: Any agent which
can alter fetal morphology or subsequent
function if the fetus is exposed during
critical stage of development( chemical,
physical, metabolic or infections).
ŌĆó Factors affecting teratogenicity
’āśGenetic predisposition.
’āśDevelopmental stage at exposure.
’āśThe route & length of administration.
11. NON GENETIC CAUSES
DEVELOPMENTAL STAGE OF EXPOSURE
1. Zygote(D0 to D7): Resistant period
(All or none phenomenon).
2. Embryogenesis (D7 to D57):
Maximum susceptibility.
3. Fetal stage (> D 57): Lowest
susceptibility
’āś IUFGR.
’āś Functional impairment of organ
systems.
12. MECHANISM OF
TERATOGENICITY
ŌĆó Causing mutations.
ŌĆó Altering differentiation.
ŌĆó Inhibiting structural protein
synthesis.
ŌĆó Inhibiting tissue interaction.
ŌĆó Altering morphogenesis (selective
cell death).
ŌĆó Reacting with DNA, enzymes and
structural proteins.
24. PREVENTIVE MEASURES
ŌĆó 1- Control of drug intake, abuse, smoking.
ŌĆó 2- Detection & control of medical diseases.
ŌĆó 3- Non exposure to irradiation.
ŌĆó 4- Control of pollution & occupational
hazards.
ŌĆó 5- Genetic counseling.
ŌĆó 6- Antenatal diagnosis & management of
genetic diseases.
ŌĆó 7- Discourage consanguineous marriage.
25. GENETIC COUNSELING
It is the process by which the
patient who at risk of disorder that
may be hereditary, are advised of
the consequences of the disorder,
the probability of developing and
transmitting it and of the ways in
which this may be prevented.
26. Indications of genetic
procedure work up
.
IN HIGH RISK PATIENTS
WHO CAN GIVE CONGENITALLY
MALFORMED BABY.
1- Maternal age more than 35 years.
2- History of congenitally malformed
baby.
3- Family history of congenital
malformation.
4- Hereditary disease in parents.
31. ANENCEPHALY
ŌĆó Lethal, may be recurrent.
ŌĆó Biochemical markers: AFP, ACE.
ŌĆó Common in DM, PP.
ŌĆó Obstetric complications: abortion
polyhydramnios, prematurity, post maturity,
IUFD, NND, increased face presentation,
shoulder dystochia.
ŌĆó P/V during labor: soft tissues, bony rim all
around, no sutures nor
fontanelles( misdiagnosed as face or frank
breech).
ŌĆó Treatment: Elective abortion, induction of
labor.
38. HYDROCEPHALUS
ŌĆó Definition: It is excessive accumulation
of CSF within the ventricles, and
subarachnoid space.
ŌĆó Associations: commonly associated with
other malformations e.g., spina bifida.
ŌĆó Etiology:
1. Congenital: cerebral malformations.
2. Infections: CMV, toxoplasmosis.
3. Chromosomal: Triploidy, Trisomy 18, X-
linked trait.
4. Hemorrhage and tumors: intracerebral.
ŌĆó U/S value: - Diagnosis. - Prognosis.
41. SPINA BIFIDA
ŌĆó Definition: Defect in the spine due to
failure of fusion of the two halves of
vertebral arch.
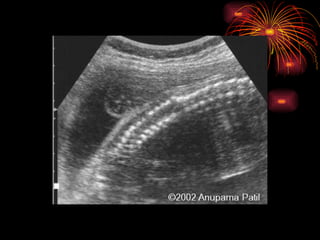
ŌĆó U/S: -diagnosed at 18th
week of gestation.
ŌĆō wide spacing of posterior ossification
centers of the spine. ŌĆō U- shaped vertebral
segment. ŌĆō defect. ŌĆōsac.
ŌĆó Prognosis: related to:-
1. Neurological involvement.
2. Associated anomalies.
3. Chromosomal defects: e.g., trisomy 18.
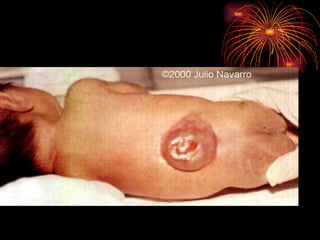
42. SPINA BIFIDA
ŌĆó TYPES:
1. Occulta
2. Overta (Cystica) : meningocele,
meningomyelocele, myelocele .
ŌĆó RISK: Rupture, Injury, Infection.
ŌĆó IMMEDIATE CARE AFTER DELIVERY:
’āś Cover the lesion with sterile non
adhesive dressing.
’āś Searching for other malformation.
’āś Consulting neurosurgeon.
61. ENCEPHALOCELE
ŌĆó Sac containing neural tissues
continuous with the brain.
ŌĆó Skull defect should be present.
ŌĆó Usually occipital or parietal, rarely
frontal.
ŌĆó May be associated with Mackel┬┤s
syndrome:
* Enecephalocele.
* Polydactyly.
* Polycystic kidney.
63. MAJOR CONGENITAL
MALFORMATIONS
B-GIT ANOMALIES
ŌĆó Cleft lip and palate.
ŌĆó Tracheo-esophageal.
ŌĆó Pyloric stenosis.
ŌĆó GIT atresia: Esophageal, duodenal,
jejunal and ileal.
ŌĆó Exomphalus (Omphalocele). Major and
minor.
ŌĆó Imperforate anus (High, Low).
64. OMPHALOCELE (EXOMPHALUS)
ŌĆó Definition: congenital umbilical
hernia.
ŌĆó AN diagnosis: U/S.
ŌĆó Features: Semi translucent very
thin sac at site of umbilicus.
ŌĆó Layers of the sac:
1. amniotic membrane
2. Wharton┬┤ s jelly
3. peritoneum.
65. TYPES AND TREATMENT
MINOR
MAJOR
Characters:
-Small sac.
-Summit attached to cord.
-Contains intestine.
-Good peritoneal cavity.
Characters:
-large sac.
-Upper aspect attached to
cord.
-Contains intestine, liver.
-Small peritoneal cavity.
Treatment:
Reduction, twisting &
strapping.
Treatment:
Undermining creating
flaps, gastric
aspiration.
66. OMPHALOCELE
ŌĆó RISKS: Rupture of the sac, injury &
infection.
ŌĆó IMMEDIATE CARE AFTER LABOR:
’āś No clamping of the protruding mass.
’āś Clamping umbilical cord away from the
swelling.
’āś Using pads soaked with saline.
’āś Protecting the mass from irritation, trauma
or infection ( gentle handling).
’āś Emptying the stomach from air.
69. CLEFT LIP AND PALATE
ŌĆó Inheritance: Polygenic.
ŌĆó Diagnosis: U/S, fetoscopy.
ŌĆó Problems: Feeding, e.g.,
aspiration, infection.
ŌĆó Treatment: Surgical repair can
be done in first few days of
life.
75. IMPERFORATE ANUS
ŌĆó Antenatal diagnosis: U/S.
ŌĆó Postnatal diagnosis: Plain X-Ray.
ŌĆó Types and treatment:
HIGH
LOW
Characters: above
pelvic floor, may be
associated with
urinary fistula,
deficient pelvic floor,
bad prognosis.
Characters: below
pelvic floor, easy
diagnosis, simple
treatment, good
prognosis.
Treatment: rectal pull
Treatment: opening
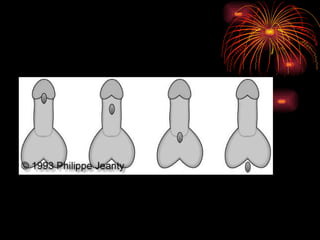
80. URETHERAL OPENING
ANOMALIES
ŌĆó Description: The urethral orifice opens
abnormally proximal to glans penis.
ŌĆó Types:
1. Epispadius.
2. Hypospadius.
ŌĆó Possible associations: intersex, XXY,
Trisomy 18.
ŌĆó Treatment: no circumcision, surgical
correction during 2nd
year of life.
84. CARDIOVASCULAR ANOMALIES
ŌĆó COMMON LESIONS: VSD, ASD, PDA,
pulmonary a stenosis, Fallot┬┤ s
tetralogy.
ŌĆó They may be minor or major,
commonly associated with other
anomalies.
ŌĆó ANTENATAL U/S DIAGNOSIS:
1. Four-chamber view.
2. M-mode.
3. Doppler color-view.
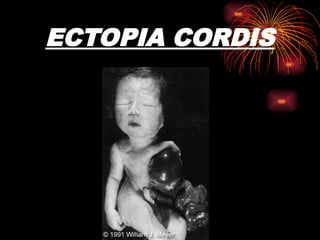
91. ECTOPIA CORDIS
ŌĆó Definition: Defect in fusion of anterior
wall of the chest and abdomen.
ŌĆó Etiology: Unknown etiology.
ŌĆó Pathogenesis: failure of mid line
fusion or early rupture.
ŌĆó Associations: Commonly associated
with CNS, cardiac, GIT anomalies.
ŌĆó Prognosis: Very poor prognosis.