






















































More Related Content
Similar to edema @ ppt 2212weerwqrqwr3eqrewrerrrrrrrrer (20)
More from MSrujanaDevi (20)


















Recently uploaded (20)




















edema @ ppt 2212weerwqrqwr3eqrewrerrrrrrrrer
- 4. FLUID OVERLOAD (HYPERVOLEMIA) It is excessive accumulation of fluid in the body, due to: 1Excessive parenteral infusion 2Deficiencies in cardiovascular or renal fluid volume regulation
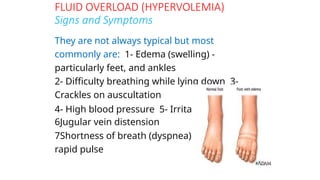
- 5. FLUID OVERLOAD (HYPERVOLEMIA) Signs and Symptoms They are not always typical but most commonly are: 1- Edema (swelling) - particularly feet, and ankles 2- Difficulty breathing while lying down 3- Crackles on auscultation 4- High blood pressure 5- Irritated cough 6Jugular vein distension 7Shortness of breath (dyspnea) 8- Strong, rapid pulse
- 7. EFFECTS OF FLUID OVERLOAD âž” Interstitial oedema Effusions Prolonged ventilator therapy âž” âž” âž” Oedema of the gut Delayed enteral feeding Translocation of bacteria âž” âž” âž” Prolonged ICU & hospital stay âž” Reduced tissue oxygen tension Impaired wound healing âž”
- 8. FLUID OVERLOAD (HYPERVOLEMIA) Management of Hypervolemia 1- Prevention is the best way 2- Sodium restriction 3Fluid restriction 4Diuretics 5Dialysis
- 9. EDEMA Edema refers to the presence of excess fluid in the body tissues. In most instances, edema occurs mainly in the extracellular fluid compartment, but it can involve intracellular fluid as well.
- 10. INTRACELLULAR EDEMA (1) Depression of the metabolic systems of the tissues (2) Lack of adequate nutrition to the cells When blood flow to a tissue is decreased, the delivery of oxygen and nutrients is reduced. If the blood flow becomes too low to maintain normal tissue metabolism, the cell membrane ionic pumps become depressed - osmosis Sometimes this can increase intracellular volume of a tissue area to two to three times normal. Intracellular edema can also occur in inflamed tissues. Inflammation usually has a direct effect on the cell membranes to increase their permeability, allowing sodium and other ions to diffuse into the interior of the cell, with subsequent osmosis of water into the cells.
- 11. fluid EXTRACELLULAR EDEMA Extracellular fluid edema occurs when there is excess accumulation in the extracellular spaces. There are two general causes of extracellular edema: (1)abnormal leakage of fluid from the plasma to the interstitial spaces across the capillaries, and (2)Failure of the lymphatics to return fluid from the interstitium back into the blood. The most common clinical cause of interstitial fluid accumulation is excessive capillary fluid filtration. -Increased capillary hydrostatic pressure. -Decreased plasma colloid osmotic pressure.
- 12. MPHATIC BLOCKAGE CAUSES EDEMA When lymphatic blockage occurs, edema can become severe because plasma proteins that leak into the interstitium have no other way to be removed. The rise in protein concentration raises the colloid osmotic pressure of the interstitial fluid, which draws even more fluid out of the capillaries. Blockage of lymph flow can be severe with infections of the lymph nodes, such as occurs with infection by filaria nematodes. Blockage of the lymph vessels can occur in certain types of cancer or after surgery in which lymph vessels are removed or obstructed. For example, large numbers of lymph vessels are removed during radical mastectomy, impairing removal of fluid from the breast and arm areas and causing edema and swelling of the tissue spaces - temporary
- 13. EDEMA CAUSED BY HEART FAILURE In heart failure, the heart fails to pump blood normally from the veins into the arteries; this raises venous pressure and capillary pressure, causing increased capillary filtration. In addition, the arterial pressure tends to fall, causing decreased excretion of salt and water by the kidneys, which increases blood volume and further raises capillary hydrostatic pressure to cause still more edema. Also, diminished blood flow to the kidneys stimulates secretion of renin, causing increased formation of angiotensin II and increased secretion of aldosterone, both of which cause additional salt and water retention by the kidneys.
- 14. EDEMA CAUSED BY HEART FAILURE In patients with left-sided heart failure, blood is pumped into the lungs normally by the right side of the heart but cannot escape easily from the pulmonary veins to the left side of the heart because this part of the heart has been greatly weakened. Consequently, all the pulmonary vascular pressures, including pulmonary capillary pressure, rise far above normal, causing serious and life-threatening pulmonary edema. When untreated, fluid accumulation in the lungs can rapidly progress, causing death within a few hours. Right sided heart failure – systemic edema
- 15. EDEMA CAUSED BY DECREASED KIDNEY EXCRETION OF SALT AND WATER  Most sodium chloride added to the blood remains in the extracellular compartment, and only small amounts enter the cells.  Therefore, in kidney diseases that compromise urinary excretion of salt and water, large amounts of sodium chloride and water are added to the extracellular fluid.  Most of this salt and water leaks from the blood into the interstitial spaces, but some remains in the blood.  The main effects of this are to cause  (1) widespread increases in interstitial fluid volume (extracellular edema)  (2) hypertension
- 16. EDEMA CAUSED BY DECREASED PLASMA PROTEINS  One of the most important causes of decreased plasma protein concentration is loss of proteins in the urine in certain kidney diseases, a condition referred to as nephrotic syndrome.  Multiple types of renal diseases can damage the membranes of the renal glomeruli, causing the membranes to become leaky to the plasma proteins and often allowing large quantities of these proteins to pass into the urine.  When this loss exceeds the ability of the body to synthesize proteins, a reduction in plasma protein concentration occurs.  Serious generalized edema occurs when the plasma protein concentration falls below 2.5 g/100 ml.
- 17. EDEMA CAUSED BY DECREASED PLASMA PROTEINS  Cirrhosis of the liver is another condition that causes a reduction in plasma protein concentration.  Cirrhosis means development of large amounts of fibrous tissue among the liver parenchymal cells. One result is failure of these cells to produce sufficient plasma proteins.  The liver fibrosis sometimes compresses the abdominal portal venous drainage vessels as they pass through the liver before emptying back into the general circulation.  Blockage of this portal venous outflow raises capillary hydrostatic pressure throughout the gastrointestinal area and further increases filtration of fluid out of the plasma into the intra- abdominal areas.  When this occurs, the combined effects of decreased plasma protein concentration and high portal capillary pressures cause transudation of large amounts of fluid and protein into the abdominal cavity, a condition referred to as ascites.
- 18. I. Increased capillary pressure A. Excessive kidney retention of salt and water 1. Acute or chronic kidney failure 2. Mineralocorticoid excess B. High venous pressure and venous constriction 3. Heart failure 4. Venous obstruction 5. Failure of venous pumps (a) Paralysis of muscles (b) Immobilization of parts of the body (c) Failure of venous valves C. Decreased arteriolar resistance 1. Excessive body heat 2. Insufficiency of sympathetic nervous system 3. Vasodilator drugs
- 19. II. Decreased plasma proteins A. Loss of proteins in urine (nephrotic syndrome) B. Loss of protein from shed skin areas 1. Burns 2. Wounds C. Failure to produce proteins 3. Liver disease (e.g., cirrhosis) 4. Serious protein or caloric malnutrition
- 20. III. Increased capillary permeability A.Immune reactions that cause release of histamine and other immune products B.Toxins C.Bacterial infections D.Vitamin deficiency, especially vitamin C E.Prolonged ischemia F.Burns
- 21. IV. Blockage of lymph return A. Cancer B. Infections (e.g., filaria nematodes) C. Surgery D. Congenital absence or abnormality of lymphatic vessels
- 22. Failure to reduce edema by increasing capillary colloid oncotic pressure. • Hypoalbuminemia is well recognized as a marker of disease severity in critical illness. • Administering exogenous albumin or other colloids to increase capillary COP does not reduce peripheral or pulmonary edema, nor improve overall outcomes in sepsis. • The no-absorption rule can provide a partial explanation, because even increasing COP gradient across the capillary wall by administration of albumin will not lead to reabsorption of fluid from edematous tissues. • Apparent shifts of fluid from the interstitial to the intravascular compartment based on a reduced hematocrit after albumin infusion do not account for the potential role of compaction of the glycocalyx layer and transfer of fluid from the SGL to the plasma volume. • Finally, the importance of the endothelial glycocalyx is highlighted by studies showing that its degradation significantly impairs endothelial barrier function.
- 23. • A range of physiologic insults may lead to glycocalyx injury and shedding, with the subsequent appearance of free heparin, chondroitin, and hyaluronic acid in the plasma. • These include natriuretic peptides (which may be released in acute excessive increased intravascular volume),hyperglycemia, and inflammatory mediators released during surgery, trauma, and sepsis, such as C-reactive protein, bradykinin, and tumor necrosis factor (TNF). • Glycocalyx degradation may make an important contribution to the already well-characterized endothelial dysfunction seen in inflammation, in which phenotypic changes occur in endothelial cells • An increase in the number of large pores, and a reduction in interstitial hydrostatic pressure favor Jv, with an increase in edema in compliant tissues such as the lung, muscles, and loose connective tissue. • Impaired glycocalyx function will further favor Jv and lead to endothelial platelet aggregation and leukocyte adhesion. Maintenance of glycocalyx integrity is a therapeutic target in perioperative fluid management.
- 24. PITTING – NONPITTING EDEMA  Most of the extra fluid that accumulates is “free fluid” because it pushes the brush pile of proteoglycan filaments apart.  Therefore, the fluid can flow freely through the tissue spaces because it is not in gel form.  When this occurs, the edema is said to be pitting edema because one can press the thumb against the tissue area and push the fluid out of the area.  When the thumb is removed, a pit is left in the skin for a few seconds until the fluid flows back from the surrounding tissues.  Nonpitting edema, which occurs when the tissue cells swell instead of the interstitium or when the fluid in the interstitium becomes clotted with fibrinogen so that it cannot move freely within the tissue spaces.
- 26. SAFETY FACTOR  1. The safety factor caused by low tissue compliance in the negative pressure range is about 3 mm Hg.  2. The safety factor caused by increased lymph flow is about 7 mm Hg.  3. The safety factor caused by wash-down of proteins from the interstitial spaces is about 7 mm Hg.  Therefore, the total safety factor against edema is about 17 mm Hg.  This means that the capillary pressure in a peripheral tissue could theoretically rise by 17 mm Hg, or approximately double the normal value, before marked edema would occur.
- 27. EDEMA FLUID IN THE POTENTIAL SPACES Effusion Pericardial effusion Plural effusion Abdominal cavity, peritoneal cavity – ascites Synovial cavities, including both the joint cavities and the bursa – synovial effusion, bursitis