
















































More Related Content
Viewers also liked (8)
More from Erik StĂĄlberg (18)




EDX Facialis
- 1. Neurofysiologiska tester vidNeurofysiologiska tester vid facialisparesfacialispares Nervsignaler genom lesionen •EMG •Blinkreflex •Magnetstimulering •F-respons Nervsignaler distalt om lesionen •Excitabilitetstest •Elektroneurografi (ENeG) Stålberg
- 2. Engström -98 reg stim Elektrodplacering vidElektrodplacering vid neurografi av facialisnervenneurografi av facialisnerven
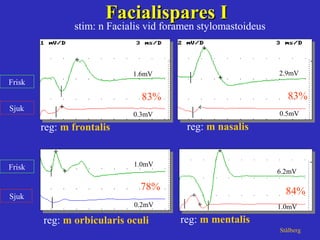
- 3. reg: m orbicularis oculi reg: m frontalis Sjuk Frisk Sjuk Frisk Facialispares IFacialispares I StĂĄlberg 1.6mV 0.3mV 83% 1.0mV 0.2mV 78% stim: n Facialis vid foramen stylomastoideus reg: m nasalis 2.9mV 0.5mV 83% 6.2mV 1.0mV 84% reg: m mentalis
- 4. Neurografi vid facialispares avNeurografi vid facialispares av lätt, måttlig och uttalad svårighetsgradlätt, måttlig och uttalad svårighetsgrad Days Ampl asym mean % Thomander-91
- 5. Days Thomander-91 Ampl asym range (I,III) % Neurografi vid facialis paresNeurografi vid facialis pares Skillnaden vid lätt och uttalad svårighetsgradSkillnaden vid lätt och uttalad svårighetsgrad 0 - - - - - - - - - - - 50 75 100 I III 1 2 3 4 5 10 20 50 100 200 500 1000 I I I I I I I I I I I I
- 6. Principer för läkning Neurapraxi Konduktionsblocket släpper funktion inom 1-3 veckor Axonal degeneration Partiell skada, distal nervutväxt funktion inom 3-6 mån Total skada, nyutväxt av axon function efter > 6mån Vid kombinerad patofysiologi alltså förbättring i 2 steg; jonkanaler, regeneration
- 7. Trigeminal nerve stim left side
- 8. BlinkreflexenBlinkreflexen n Trigeminus (V) och n Facialis (VII)n Trigeminus (V) och n Facialis (VII)
- 9. Normal blinkreflexNormal blinkreflex stim: n trigeminus supraorbitalis reg: m orbicularis oculi bilat StĂĄlberg
- 10. Patologisk blinkreflex paralys (sin)Patologisk blinkreflex paralys (sin) stim: n trigeminus supraorbitalis reg: m orbicularis oculi bilat StĂĄlberg sjuk sida
- 11. stim: n trigeminus supraorbitalis reg: m orbicularis oculi bilat Patologisk blinkreflex partiell pares (dx)Patologisk blinkreflex partiell pares (dx) StĂĄlberg sjuk sida
- 13. EMG vid facialisparesEMG vid facialispares beskriver: •Denervation = axonal degeneration •Reinnervation (pågående/avslutad) •Grad av aktivitetsförlust •Tecken på synkinesi •Tecken på kontralateral överinnervation Stålberg
- 14. Reinnervation i orb. oculi efterReinnervation i orb. oculi efter Facialispares, 3 mĂĄnFacialispares, 3 mĂĄn normalnormal reinnervationreinnervation StĂĄlberg
- 15. Andra frågeställningar för neurofysiologi i ansiktet 1. Är trigeminus intakt? 2. Nervgraftets funtion 3. Överinnervation från kontralaterala sidan
- 16. Ansiktstrauma för 5 mån sedan. Facialis u.a. men domningar ENeG normal
- 17. Trig stim sjuk sida; inget ipsi-eller contralateralt facialis-svar ( ) Stim frisk sida; normalt facialissvar från frisk och sjuk sida Inget facialissvar på grund av trig patologi Här finns facialissvar efter kontralateral trig stimulering sjuk sjuk frisk frisk
- 18. ENeG nervgraft Symmetrisk, normal Tydlig asymmetri, lĂĄgt svar pĂĄ sjuk sida dvs graftet har endast MĂĄttlig effekt
- 19. Innervation från frisk sida över meddellinjen några cm
- 20. Right sided posttraumatic facial palsy Some voluntary activity near the midline but no response on ipsilateral nerve stimulation Reinnervation from healthy side no activity no activity frisk sida sjuk sida
- 21. Konklusion • Preoperativ neurofysiologi ej relaterad till postoperativa komplikationer • Post-operativ neurofysiologi (ENeG, blinkreflex, EMG) ger prognostisk vägledning Edfeldt et al 2003