

























































![Heart failure ŌĆō an update [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/heartfailureanupdateautosaved-110321012825-phpapp02-thumbnail.jpg?width=560&fit=bounds)









More Related Content
Similar to emphasis_HF_trial.ppt (20)
More from biplave karki (15)













Recently uploaded (20)




















emphasis_HF_trial.ppt
- 1. Journal club Dr Biplave Karki
- 2. Eplerenone in Patients with Systolic Heart Failure and Mild Symptoms Faiez Zannad, M.D., Ph.D., John J.V. McMurray, M.D., Henry Krum, M.B., Ph.D., Dirk J. van Veldhuisen, M.D., Ph.D., Karl Swedberg, M.D., Ph.D., Harry Shi, M.S., John Vincent, M.B., Ph.D., Stuart J. Pocock, Ph.D., Bertram Pitt, M.D., for the EMPHASIS-HF Study Group Original Article N Engl J Med Volume 364(1):11-21 January 6, 2011
- 3. EMPHASIS-HF ’ü« Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure
- 4. Definition of Heart Failure ’ü« The current American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) guidelines define HF as ’é© ŌĆ£a complex clinical syndrome that results from structural or functional impairment of ventricular filling or ejection of blood, which in turn leads to the cardinal clinical symptoms of dyspnea and fatigue and signs of HF, namely edema and rales. ’ü« Because many patients present without signs or symptoms of volume overload, the term ŌĆ£heart failureŌĆØ is preferred over the older term ŌĆ£congestive heart failure.ŌĆØ
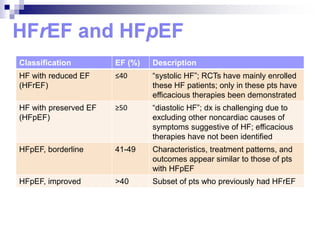
- 5. Classification EF (%) Description HF with reduced EF (HFrEF) Ōēż40 ŌĆ£systolic HFŌĆØ; RCTs have mainly enrolled these HF patients; only in these pts have efficacious therapies been demonstrated HF with preserved EF (HFpEF) Ōēź50 ŌĆ£diastolic HFŌĆØ; dx is challenging due to excluding other noncardiac causes of symptoms suggestive of HF; efficacious therapies have not been identified HFpEF, borderline 41-49 Characteristics, treatment patterns, and outcomes appear similar to those of pts with HFpEF HFpEF, improved >40 Subset of pts who previously had HFrEF
- 6. Rationale for Medications used in Heart Failure
- 7. Mortality benefit of drugs used in Heart failure
- 8. Aldosterone Antagonists Drugs Spironolactone Eplerenone MOA Non selective Selective Effect on androgen and progesterone +++ +/- S/E Increase K, Mg Decrease CO2, Metabolic acidosis Gynecomastia, hirsutism, Increase K, Mg Decrease CO2, Metabolic acidosis Dose 25 mg OD 25-50mg OD Use HF (IV) Post MI HF (II/III) Cost Cheaper Expensive
- 9. Disclosure Information ’ü« EMPHASIS-HF was funded by Pfizer.inc ’ü« Eplerenone is approved for treating heart failure after myocardial infarction.
- 10. Mineralocorticoid Receptor Antagonists in Heart Failure ’ü« Randomized Aldactone Evaluation Study (RALES) 1999 ’ü« Eplerenone PostŌĆōAcute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) 2003
- 11. RALES: Randomized Aldactone Evaluation Study ’ü« In patients with severe heart failure and left ventricular ejection fraction <35%, ’ü« Spironolactone reduced: ŌĆó All-cause mortality ŌĆó Sudden death and death due to progression of heart failure ’ü« Benefit was independent of age, ejection fraction, cause of heart failure and concurrent therapy
- 12. EPHESUS: Eplerenone PostŌĆōAcute Myocardial Infarction Heart Failure Efficacy and Survival Study ’ü« The addition of eplerenone to optimal medical therapy contributes to the continued improvement in survival and hospitalization rates among patients with acute myocardial infarction complicated by left ventricular dysfunction and heart failure
- 13. Aim of EMPHASIS-HF ’ü« to investigate the effects of eplerenone, added to evidence-based therapy, on clinical outcomes in patients with systolic heart failure and mild symptoms (i.e., NYHA functional class II symptoms.
- 14. Methods
- 15. Inclusion Criteria ’ü« >55 years of age ’ü« NYHA functional class II ’ü« Ejection fraction <30% (or, if betwn 30 to 35%, a QRS >130 msec) ’ü« Treated with the recommended or maximal tolerated dose of ACE inhibitor (or an ARB or both) and a beta- blocker (unless contraindicated) ’ü« Within 6 months of hospitalization for a cardiovascular reason (if no such hospitalization, BNP>250 pg/ml or N- pro-BNP>500 pg/ml in men and 750 pg/ml in women
- 16. Exclusion Criteria ’ü« Acute myocardial infarction ’ü« NYHA class III or IV heart failure ’ü« Serum potassium level >5.0 mmol/L ’ü« eGFR<30 ml/min/1.73 m2 ’ü« Need for a potassium sparing diuretic, and ’ü« Any other clinically significant coexisting condition
- 17. Study Design ’ü« Primary outcome: CV death or hospitalization for HF
- 18. Sample Size ’ü« The initial assumptions ’é© 2584 patients ’é© Annual event rate 18% in the placebo group ’é© 813 primary events in 48 months ’é© 80% power to detect an 18% risk reduction ’ü« June 2009 ’é© Overall blinded event rate lower than expected ’é© Sample size increased to 3100 patients
- 19. Early Stopping ’ü« May 6th 2010 ’é© DSMCŌĆÖs second interim analysis showed overwhelming benefit beyond the prespecified stopping boundary for benefit (2 sided P-value =0.000001in favour of eplerenone) ’ü« May 9th 2010 ’é© Agreed to stop patient enrollment ’ü« May 25th 2010 ’é© Trial cut off date
- 20. Results Median follow up time 21 months March 30, 2006, through May 25, 2010
- 23. Baseline Therapy
- 24. Patient Follow up and Dosing
- 25. Primary Endpoint CV Death or Hospitalization for HF- 37%
- 26. Mortality From Any Cause-24%
- 27. Hospitalization From Any Cause- 23%
- 29. Primary And Adjudicated Secondary Outcome
- 31. Other Outcomes
- 36. Safety
- 37. Summary ’ü« The addition of eplerenone to recommended treatment resulted in:
- 38. Conclusion ’ü« In patients with systolic heart failure and mild symptoms, addition of eplerenone to recommended medical therapy
- 39. TOPCAT 2014: Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist Trial ’ü« Addition of spironolactone for heart failure with preserved ejection fraction didnŌĆÖt reduce the primary outcome.
- 40. Thank you