



































More Related Content
Similar to HEMORRHOIDS- anatomy, pathophysiology, clinical features, diagnosis and management.pptx (20)
More from PhilemonChizororo (10)








Recently uploaded (20)




















HEMORRHOIDS- anatomy, pathophysiology, clinical features, diagnosis and management.pptx
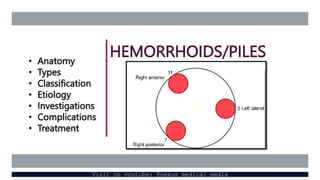
- 1. HEMORRHOIDS/PILES ŌĆó Anatomy ŌĆó Types ŌĆó Classification ŌĆó Etiology ŌĆó Investigations ŌĆó Complications ŌĆó Treatment Visit on youtube: @nexus medical media
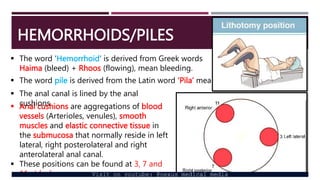
- 2. HEMORRHOIDS/PILES ’é¦ The word ŌĆśHemorrhoidŌĆÖ is derived from Greek words Haima (bleed) + Rhoos (flowing), mean bleeding. ’é¦ The word pile is derived from the Latin word ŌĆśPilaŌĆÖ means ball or a mass. ’é¦ Anal cushions are aggregations of blood vessels (Arterioles, venules), smooth muscles and elastic connective tissue in the submucosa that normally reside in left lateral, right posterolateral and right anterolateral anal canal. ’é¦ These positions can be found at 3, 7 and 11 oŌĆÖclock. ’é¦ The anal canal is lined by the anal cushions Visit on youtube: @nexus medical media
- 3. HEMORRHOIDS/PILES Hemorrhoids consist of dilated venous plexus, a small artery and areolar tissue. ŌĆó Piles can be mucosal or vascular. ’é¦ Vascular type is seen in young. ’é¦ Mucosal is seen in old. ŌĆó Present concept is weakening of ParkŌĆÖs ligament TYPES ŌĆó Hemorrhoids can either be: Ō×ó Internal- above the dentate (pectineal) line, covered with mucous membrane Ō×ó External- below the dentate (pectineal) line, covered with skin Ō×ó Interno-external- together occur. Visit on youtube: @nexus medical media
- 4. HEMORRHOIDS/PILES CLASSIFICATION Hemorrhoids can be classified according: Ō×ó Location Ō×ó Severity ACCORDING TO LOCATION Primary hemorrhoids: ŌĆó Located at 3, 7, 11 oŌĆÖclock positions related to the branches of the superior hemorrhoidal vessels which divides on the right side into 2, and on the left side it continues as 1 Secondary hemorrhoids: One which occur between the primary sites. Visit on youtube: @nexus medical media
- 5. HEMORRHOIDS/PILES ACCORDING TO SEVERTIY First degree: piles within that may bleed but does not come out Second degree: piles that prolapse during defecation but returns back spontaneously Third degree: piles prolapsed during defecation, can be replaced back only by manual help Fourth degree: pile that are permanently prolapsed.
- 6. HEMORRHOIDS/PILES ETIOLOGY ’é¦ Hereditary ’é¦ Idiopathic ’é¦ Morphologic: weight of the blood column without valves causes high pressure. ŌĆó Veins in the lower rectum are in loose submucosal plane but the veins above enter the muscular layer, which on contraction increases the venous congestion below (more prevalent in patients with constipation). ŌĆó Superior rectal veins have no valves (as they are tributaries of portal vein) and so more congestion. Other causes: Ō×ó Straining, diarrhea, constipation, hard stool, low fiber diet, over-purgation Ō×ó Carcinoma rectum, portal hypertension (rare cause) Ō×ó Pregnancy: during pregnancy raised progesterone relaxes the venous wall and reduces its tone, enlarged uterus compresses the pelvic vein and constipation is a common problem. Visit on youtube: @nexus medical media
- 7. HEMORRHOIDS/PILES CLINICAL FEATURES ŌĆó It occurs at any age but mostly between 30 to 65 years. ŌĆó Incidence is equal in both sexes. ŌĆó Painless Bleeding- 1st symptom- ŌĆśsplash in the panŌĆÖ- ŌĆśbright red and freshŌĆÖ- occurs during defecation ŌĆó Mass per anum. ŌĆó Pain- may be due to prolapse, infection or spasm ŌĆó Prolapse of internal hemorrhoids may produce moisture in the anal region or mucus discharge that causing itching. ŌĆó Anemia- secondary Visit on youtube: @nexus medical media
- 8. HEMORRHOIDS/PILES EXAMINATION ’é¦ On inspection, prolapsed piles will be visualized ’é¦ On P/R examination, only thrombosed piles can be felt. INVESTIGATIONS ’é¦ Proctoscopy: note number, degree, size, surface and appearance of piles as well as features of chronicity of the prolapse. ’é¦ Sigmoidoscopy or colonoscopy: malignancy ’é¦ Endoscopy to rule out other sources of rectal bleeding e.g. cancer and inflammatory bowel disease. ’é¦ Full blood count-check for anemia (hematocrit) and platelet count Visit on youtube: @nexus medical media
- 9. HEMORRHOIDS/PILES COMPLICATIONS ŌĆó Profuse hemorrhage which may require blood transfusion ŌĆó Strangulation- by anal sphincter ŌĆó Thrombosis- piles appear dark purple/black, feels solid and tender ŌĆó Ulceration ŌĆó Gangrene ŌĆó Fibrosis ŌĆó Stenosis ŌĆó Suppuration leads to perianal or submucosal abscess ŌĆó Pylephlebitis (portal pyaemia) is rare but can occur in 3rd degree piles after surgery. Visit on youtube: @nexus medical media
- 10. HEMORRHOIDS/PILES TREATMENT Medical ’āś Sitz bath- immersing anal region for 15-20 minutes, 2-3 times a day. ŌĆó To reduce edema, pain and promote healing ’āś Analgesics, local anesthetic cream ’āś Antihistamines ’āś Antibiotics ’āś Laxatives ’āś Local anesthetics and anti-inflammatory drugs e.g. annomax Visit on youtube: @nexus medical media
- 11. HEMORRHOIDS/PILES TREATMENT Parasurgical ’āś Sclerotherapy ’āś Banding ’āś Cryotherapy ’āś Infrared coagulation (IRC) ’āś Laser therapy ’ā╝ Doppler guided haemorrhoidal artery ligation (DGHAL): ŌĆó good for pregnant and diabetic patients Visit on youtube: @nexus medical media
- 12. HEMORRHOIDS/PILES TREATMENT Surgical ’āś Open haemorrhoidectomy (Milligan-Morgan)-Britain ’āś Closed haemorrhoidectomy (Hill-Fergusson)- USA ’āś Stapled haemorrhoidopexy (Antonio Longo) ’āś Anal stretching Visit on youtube: @nexus medical media
- 13. HEMORRHOIDS/PILES SEVERITY MEDICAL PARASURGICAL SURGICAL 1st degree Medical interventions usually enough ŌĆó Sclerotherapy can be done ŌĆó DGHAL can be done 2nd degree Medical interventions usually enough ŌĆó Sclerotherapy can be done ŌĆó BarronŌĆÖs banding is done ŌĆó DGHAL can be done 3rd degree Medical interventions can help patients especially before surgery ŌĆó Laser therapy can be done ŌĆó DGHAL can be done Hemorrhoidectomy is gold standard 4th degree Medical interventions can help patients especially before DGHAL can be done Hemorrhoidectomy is gold standard Visit on youtube: @nexus medical media
- 14. HEMORRHOIDECTOMY Visit on youtube: @nexus medical media