




Intertrochanteric Fracture
- 1. Extern Conference PHRAMONGKUTKLAO COLLEGE OF MEDICINE Ext.Supattarapong Jaideejaroen
- 2. Case : ŕ¸ŕ¸šŕšŕ¸ŕšŕ¸§ŕ¸˘ŕ¸ŕ¸˛ŕ¸˘ŕšŕ¸ŕ¸˘ŕ¸ŕ¸˛ŕ¸˘ŕ¸¸ 45 ŕ¸ŕ¸ľ no underlying disease Chief complaint : ŕ¸ŕ¸§ŕ¸ŕ¸Şŕ¸°ŕšŕ¸ŕ¸ŕ¸ŕ¸§ŕ¸˛ 3 ŕ¸ŕ¸ąŕšŕ¸§ŕšŕ¸Ąŕ¸ ŕ¸ŕšŕ¸ŕ¸ŕ¸Ąŕ¸˛ รŕ¸. Present illness : - 3 ŕ¸ŕ¸Ą.ŕ¸ŕšŕ¸ŕ¸ŕ¸Ąŕ¸˛ รŕ¸. ŕ¸ŕ¸šŕšŕ¸ŕšŕ¸§ŕ¸˘ŕ¸ŕ¸ľŕšŕ¸ŕ¸ąŕ¸ŕ¸Łŕ¸˘ŕ¸˛ŕ¸ŕ¸˘ŕ¸ŕ¸ŕš ŕšŕ¸Ľŕšŕ¸§ŕ¸ŕ¸šŕ¸ŕ¸Łŕ¸ŕ¸ŕ¸Łŕ¸°ŕ¸ŕ¸°ŕ¸ŕ¸ ŕ¸ŕ¸šŕšŕ¸ŕšŕ¸§ŕ¸˘ŕ¸ŕ¸Łŕ¸°ŕšŕ¸ŕšŕ¸ŕšŕ¸Ľŕšŕ¸§ŕ¸ŕ¸ŕ¸Ľŕ¸ŕ¸ŕ¸ˇŕšŕ¸ ŕšŕ¸ŕ¸˘ŕšŕ¸ŕ¸˛ŕ¸Łŕšŕ¸˛ŕ¸ŕ¸ŕ¸˛ŕ¸˘ŕ¸ŕšŕ¸˛ŕ¸ŕ¸ŕ¸§ŕ¸˛ŕ¸Ľŕ¸ŕ¸ŕ¸Łŕ¸°ŕšŕ¸ŕ¸ ŕ¸ŕ¸šŕšŕ¸ŕšŕ¸§ŕ¸˘ŕ¸ŕ¸˛ŕšŕ¸Ťŕ¸ŕ¸¸ŕ¸ŕ¸˛ŕ¸Łŕ¸ŕšŕšŕ¸ŕšŕšŕ¸Ąŕšŕ¸Ťŕ¸Ąŕ¸ŕ¸Şŕ¸ŕ¸´ ŕšŕ¸ŕšŕ¸Ąŕ¸ľŕ¸ŕ¸˛ŕ¸ŕ¸˛ŕ¸Łŕ¸Ąŕ¸śŕ¸ŕšŕ¸Ąŕ¸˛ŕ¸Şŕ¸¸ŕ¸Łŕ¸˛ ญ฼ูŕ¸ŕšŕ¸ŕ¸´ŕ¸ŕšŕ¸Ťŕ¸ŕ¸¸ŕ¸Ąŕ¸ľŕšŕ¸ŕšŕ¸ŕ¸ŕ¸ľŕšŕ¸Ťŕ¸ŕšŕ¸˛ŕ¸ŕ¸ŕšŕ¸Ľŕ¸°ŕ¸ŕ¸ ŕšŕ¸Ľŕ¸°ŕ¸Ąŕ¸ľ ŕ¸ŕ¸˛ŕ¸ŕšŕ¸ŕ¸Ľŕ¸ŕ¸ľŕšŕšŕ¸ŕšŕ¸˛ŕ¸ŕ¸§ŕ¸˛ ล฾ŕ¸ŕ¸˛ŕ¸ŕ¸˛ŕ¸Łŕ¸ŕ¸§ŕ¸ŕ¸Şŕ¸°ŕšŕ¸ŕ¸ŕ¸ŕšŕ¸˛ŕ¸ŕ¸ŕ¸§ŕ¸˛ ŕ¸ŕ¸§ŕ¸ŕ¸Ąŕ¸˛ŕ¸ŕ¸ŕ¸ŕ¸ŕ¸˘ŕ¸ąŕ¸ŕšŕ¸Ąŕšŕšŕ¸ŕš รภEMS สŕšŕ¸ รŕ¸.ŕšŕ¸ŕ¸ŕ¸Şŕ¸šŕ¸ ŕšŕ¸Ľŕšŕ¸§ŕ¸Şŕšŕ¸ŕ¸ŕšŕ¸ŕ¸Ąŕ¸˛ รŕ¸.ลญาราŕ¸
- 3. Primery Survey A : can talk , not tender along C-spine , neck full ROM B : spontaneous breathing , equal chest expansion , equal breath sound , clear both lungs , CCT - C : BP 96/58 mmHg , Heart rate 96/min , capillary refill <2 sec D : E4V5M6 , pupil 3 mm RTLBE , motor grade V all extremities , PR good sphincter tone E : abrasion wound 3x4 cm at right knee , mild swelling , right leg deformity
- 4. Secondary Survey A : no history of drug or food allergy M : no medication P : no underlying disease L : last meal at 18.00 ( 3 hrs PTA) E : ŕšŕ¸ŕ¸´ŕ¸ŕšŕ¸Ťŕ¸ŕ¸¸ŕ¸ŕ¸ŕ¸ŕ¸ŕ¸ ŕ¸ŕ¸šŕšŕ¸ŕšŕ¸§ŕ¸˘ŕ¸ŕ¸šŕ¸ŕ¸Łŕ¸ŕ¸ŕ¸Łŕ¸°ŕ¸ŕ¸°ŕ¸ŕ¸ ŕ¸ŕ¸Łŕ¸°ŕšŕ¸ŕšŕ¸ŕšŕ¸ŕ¸˛ŕ¸Łŕšŕ¸˛ŕ¸ŕ¸ŕ¸˛ŕ¸˘ŕ¸ŕšŕ¸˛ŕ¸ŕ¸ŕ¸§ŕ¸˛ŕ¸Ľŕ¸ŕ¸ŕ¸Łŕ¸°ŕšŕ¸ŕ¸ ŕ¸ŕ¸˛ŕšŕ¸Ťŕ¸ŕ¸¸ŕ¸ŕ¸˛ŕ¸Łŕ¸ŕšŕšŕ¸ŕš ล฾สŕ¸ŕ¸´ŕ¸Łŕ¸šŕšŕ¸ŕ¸ąŕ¸§ ŕšŕ¸ŕšŕ¸Ąŕ¸ľŕ¸ŕ¸˛ŕ¸ŕ¸˛ŕ¸Łŕ¸Ąŕ¸śŕ¸ŕšŕ¸Ąŕ¸˛ ญ฼ูŕ¸ŕšŕ¸ŕ¸´ŕ¸ŕšŕ¸Ťŕ¸ŕ¸¸ŕšŕ¸ŕšŕ¸ŕ¸Ťŕ¸ŕšŕ¸˛ŕ¸ŕ¸ ŕ¸ŕ¸ ŕšŕ¸Ľŕ¸°ŕ¸ŕ¸§ŕ¸ŕ¸Şŕ¸°ŕšŕ¸ŕ¸ŕ¸ŕ¸§ŕ¸˛ŕ¸Ąŕ¸˛ŕ¸ ล฾ŕšŕ¸ŕ¸Ľŕ¸ŕ¸ľŕšŕšŕ¸ŕšŕ¸˛ŕ¸ŕ¸§ŕ¸˛
- 5. Physical Examination GA : A middle age Thai man , good consciousness , E4V5M6 HEENT : no discharge from eye or ear , no neck pain , no hematoma Chest : equal chest movement , no stridor , clear and equal breath sound , trachea in midline , equal tympanic on percussion Heart : normal S1,S2 , no murmur , distal pulse can be palpated Abdomen : soft , not tender , no guarding . no rebound tenderness Neuro : pupil 3 mm RTLBE , motor grade V all ext. , sensory intact , reflex 2+ all , PR good sphincter tone V/S : BP 96/58 mmHg BT 36.7 HR 96 /min RR 22 /min
- 6. Extremity : Rt. Leg ď external rotation deformity , Rt.leg shorter than left leg , cannot lift leg , no tender point , pelvic compression negative , no wound , no swelling Rt. Knee ď abrasion wound size 3x4 cm , no deformity , full ROM Rt. Ankle ď no wound , not tender , full ROM Physical Examination
- 10. Investigation
- 11. Investigation
- 12. FAST : negative Film - C-spine : Closed fracture at spinous processC3-C4 - Both Hip AP and Hip lateral : Closed fracture at intertrochanter of right femur Investigation
- 13. Treatment - On skeletal traction right leg 2 kg - On Philadelphia collar - NPO - 5% DN/2 1000 ml IV rate 80 ml/hr - CBC , BUN , Cr , Electrolyte - Chest X-ray
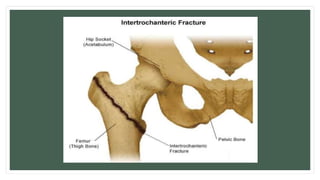
- 15. Definition ⢠An intertrochanteric fracture occurs between the greater and lesser trochanter, where the gluteus medius and minimus muscle (hip extensor and abductor)attach, and the lesser trochanter, where the iliopsoas muscle (hip flexor)attaches.
- 17. General Features ⢠Exuracapsular fracture with better healing potential ⢠Common in elderly osteoporotic patient, usually woman in their 80âs ⢠More common than intracapsular ⢠Rarely causes avascular necrosis
- 18. Mechanism of Injury ⢠In younger individual are usually the result of a high-energy injury, such as a motor vehicle accident or fall from high. ⢠In elderly, it result from a simple fall.
- 19. Signs and Symptoms ⢠Pain ⢠Marked shortening of lower limb ⢠Patient can not lift their leg ⢠Complete external rotation deformity ⢠Swelling, ecchymosis and tenderness over the greater trochanter
- 20. Investigation - Pelvis AP - Pelvis cross-table lateral
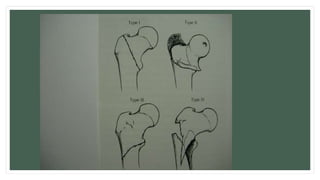
- 21. Classification(Boyd & Griffin) Stable fractures ⢠Type I: Nondisplaced fracture ⢠Type II: Displaced fracture Unstable fractures ⢠Type III: Reverse,subtrochanteric,or posteromedial comminution fracture ⢠Type IV: Intertrochanteric fracture with subtrochanteric fracture
- 23. Stability of fracture ⢠Integrity of the posteromedial cortex is the most important factor ⢠Reverse fracture is more unstable ⢠Subtrochanter fracture is more unstable
- 24. Treament - Nonoperative nonweightbearing with early out of bed to chair indications - nonambulatory patients - patients at high risk for perioperative mortality outcomes - high rates of pneumonia, urinary tract infections, decubiti, and DVT
- 25. Treament - Operative - sliding hip compression screw indications - stable intertrochanteric fractures - intramedullary hip screw (cephalomedullary nail) indications - stable fracture patterns - unstable fracture patterns - reverse obliquity fractures 56% failure when treated with sliding hip screw - subtrochanteric extension - lack of integrity of femoral wall associated with increased displacement and collapse when treated with sliding hip screw
- 26. Complications ďś Less non-union or avascular necrosis ďś Malunion happened in unstable fractures
- 27. Thank you