Editor's Notes
- #2: Retinopathy is a complication of diabetes that results in damage to the network of capillaries that supply blood to the retina.
- #4: Diseases that affect the eye in diabetes are: 1. Retinopathy 2. Cataract 3. Cranial nerve palsies leading to diplopia depending on the nerve affected 4. Diabetic papillopathy This presentation will focus on diabetic retinopathy but not on the other conditions.
- #5: Transient vision changes are common in people with diabetes and are not necessarily indicative of eye disease. It is important to ask the person about this common symptom in diabetes. People experience osmotic changes in the lens due to fluctuating blood glucose levels. In other words the lens changes shape, and the vision changes ŌĆō in some it becomes worse ŌĆō in some better. This terrifies many people as they fear it is the beginning of blindness. They have to be reassured that the change will revert several weeks after the blood glucose levels have settled. Also they should be advised not to get spectacles/eyeglasses during this period. Blurred vision may also be due to other eye manifestations; these can be ruled out by an ophthalmologic exam.
- #6: In its initial stages diabetic retinopathy is a silent condition. People can often see well until they have a bleed in the eye. When symptoms do occur the disease is generally quite advanced. This makes treatment much more difficult and potentially poorer outcomes. Therefore, regular screening to look for retinopathy is a cornerstone for diabetes assessment. At any one time, approximately 30% percent of people with diabetes have some form of retinopathy. But it is important to note that only 6-13% will develop vision threatening retinopathy. Therefore, if a person develops a few microaneuryms in the eye, this does not mean it is the beginning of blindness; only a small percentage of people will go on to develop vision threatening retinopathy. Hence once the grade of retinopathy is determined, the person should be informed of the severity of their condition and the implications for their vision. Kempen JH, OŌĆÖColmain BJ, Leske MC et al. (2004) The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol, 122, 552-563.
- #7: When should people with diabetes be screened for retinopathy? People with type 1 diabetes do not usually live undiagnosed for long periods of time. Therefore once the person is more than 10 years old screening for complications should be performed within 5 years of initial diagnosis of diabetes. On the other hand, people with type 2 diabetes may have had the disease for many years without knowing it. At diagnosis, 30% of people with type 2 diabetes already have a complication. For this reason, it is important to screen for complications in type 2 diabetes at the time of diagnosis. Following initial screening, people should be assessed every 1 to 2 years thereafter, depending on the status of the retina. However, assessment may need to be more frequent if the complication status is severe or if the person has had diabetes for a long time. American Diabetes Association. (2010). Clinical Practice Guidelines 2010. Diabetes Care, 33(Suppl 1). Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. (2008). 2008 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diab, 32(Suppl 1).
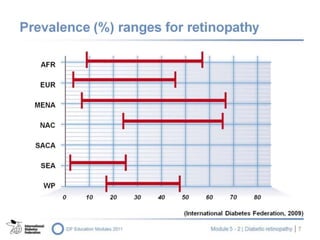
- #8: AFR = African Region EUR = European Region MENA = Middle East and Northern Africa Region NAC = North American and Caribbean SACA = South and Central America SEA = South East Asia WP = Western Pacific International Diabetes Federation. (2009). IDF Diabetes Atlas. Brussels: International Diabetes Federation.
- #9: There are many risk factors that influence the development of retinopathy. These include: Poor glycaemic control; the next couple of slides will provide data from major clinical trials showing conclusive evidence The longer the person has diabetes the more likely they are to develop retinopathy; the level of glycaemic control and duration are the two most important predictors of retinopathy Other important predictors of risk but to a lesser degree are hypertension, high cholesterol and kidney disease Pregnancy is another risk factor; it will be addressed later in this presentation
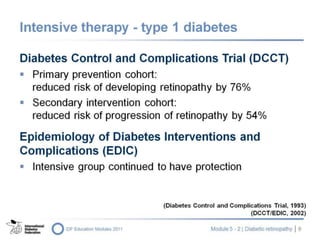
- #10: In the primary prevention cohort of the Diabetes Control and Complications Trial (DCCT), people with type 1 diabetes receiving intensive insulin therapy who entered the trial without retinopathy saw their risk of developing retinopathy reduced by 76%. Participants who had some retinopathy at the beginning of the study also showed a significant reduction in the risk of progression of their retinopathy. These are very encouraging results and form the basis for tightening diabetes control in people with type 1 diabetes. And the follow up study to the DCCT ŌĆō Epidemiology of Diabetes Interventions and Complications (EDIC) ŌĆō showed after 7 years those in the DCCT conventional group had lowered their A1C from 9% to 8% and those in the former intensive therapy group had seen A1C rise from about 7% to about 8%. The conventional group did not see a dramatic reduction in the progression of retinopathy, but neither did the intensive group see an increase in the progression of retinopathy. This study has shown that the effects of hyperglycaemia exist long after the glucose levels have fallen but the effects of intensive therapy may persist long for a period. DCCT Trial Research Group. (1993). The effect of intensive treatment of diabetes on the development and progression of long-term complication in insulin-dependent diabetes mellitus. N Engl J Med, 329, 977-86. DCCT/EDIC writing team. (2002). Effect of intensive therapy on the microvascular complications of type 1 diabetes. JAMA, 287(19).
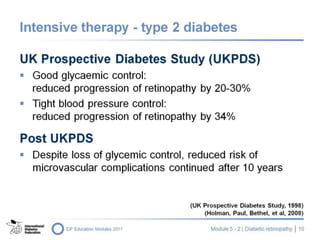
- #11: Similar results to those of the DCCT trial were also found in the large UK clinical trial in people with type 2 diabetes known as the UK Prospective Diabetes Study (UKPDS). In addition to demonstrating that intensive blood glucose control reduces progression of retinopathy by up to 30%, this major trial provided evidence on the importance of blood pressure control and in particular the importance of reducing blood pressure to reduce macular oedema. UK Prospective Diabetes Study Group. (1998). Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes. UKPDS 38. BMJ, 317, 708-13. Holman R.R., Paul, S.K., Bethel, M.A., Matthews, D.R., Neil, H.A. (2008). 10-year follow-up of intensive glucose control in type 2 diabetes. New Eng J Med, 359, 15, 1577-1589
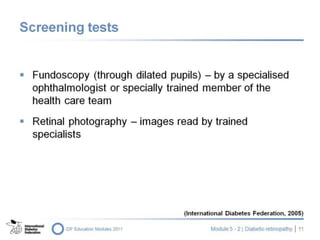
- #12: Retinal photography is recommended wherever possible. A worsening visual acuity is a warning sign that a deterioration in retinopathy status may have occurred. Reduced visual acuity, not corrected by pin-hole assessment or glasses, can be suggestive of maculopathy. It may also indicate a worsening of cataract or macular degeneration. Once visual acuity decreases to 6/24 the chance of saving the sight using laser therapy is significantly reduced. Fundoscopy is done to view the fundus or back of the eye and assess the retina and blood vessels using an ophthalmoscope. The pupil must be dilated in order to assess the fundus. Assessment with an ophthalmoscope through an undilated pupil is unacceptable as the pupil constricts with the bright light reducing the amount of retina that can be visualised. Fundoscopy must be done by a specialist ophthalmologist or a specially trained member of the health care team. In some situations, especially where access to a competent and experienced examiner is difficult, a retinal camera can be used. Photographs of the retina can then be read at a later stage by a person experienced in the diagnosis and management of retinopathy. Visualising the retina in older people or those with autonomic neuropathy may be problematic due to poor dilatation. Tests for intra-ocular pressure should be done periodically. Glaucoma is known to occur more frequently in people with diabetes. International Diabetes Federation. (2005). Global Guideline for type 2 diabetes. Brussels: International Diabetes Federation.
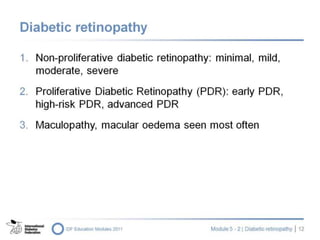
- #13: There are different grades of retinopathy that are classified as non-proliferative or proliferative diabetic retinopathy with or without maculopathy. Within each grade there are different levels of severity of retinopathy: Minimal NPDR Mild NPDR Moderate NPDR Severe NPDR Each grade is carefully defined by specific clinical characteristics. This does not mean that mild is more than minimal or moderate is more than mild and so on, but rather that each grade has specific clinical signs that characterise the particular grade of retinopathy. Each of these grades can be with or without macular oedema ’ĆŁ defined as any swelling within two disc diameters of the macular. Proliferative retinopathy is classified as early PDR, high-risk or advanced PDR.
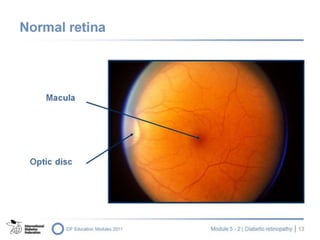
- #14: This is a normal left retina. The more prominent vessels are the veins, the lighter vessels are the arterioles. The optic disc is on the left. The macula or the part of the eye required for central vision is the darker area indicated by the top arrow and is situated two disc diameters lateral to the optic disc margin.
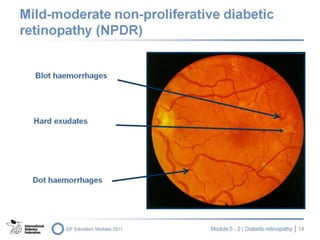
- #15: As mentioned previously, there are different grades of retinopathy within the NPDR classification. In minimal retinopathy, only one or two microaneurysms are present In mild NPDR, there are microaneuryms as well as dot or blot haemorrhages In moderate NPDR, hard exudates ’ĆŁ deposits of lipids ’ĆŁ are also present
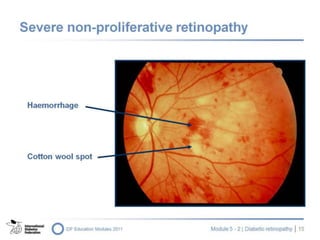
- #16: The features that characterise severe non-proliferative retinopathy are: Venous beading or looping Multiple haemorrhages Multiple soft exudates or cotton wool spots which indicate areas of ischaemia A condition called intra-retinal microvascular abnormalities (IRMA) Early referral to an ophthalmologist is essential as these lesions are sight-threatening.
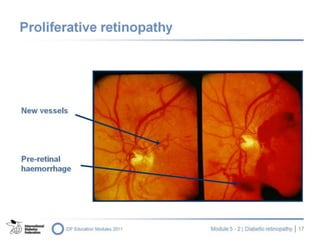
- #17: Retinopathy is classified as proliferative when there are new vessels on the disc and elsewhere. The new vessels are weak and tend to bleed into and behind the vitreous humour causing impaired vision, detachment of the retina and even blindness.
- #18: Proliferative retinopathy is sight-threatening and requires immediate referral to an ophthalmologist for treatment. The features of proliferative retinopathy are: New vessels on the optic disc or new vessels anywhere in the retina. These are fine, fragile vessels that break and bleed easily Pre-retinal haemorrhage
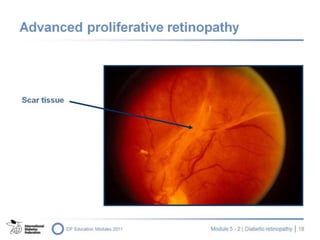
- #19: This slide shows advanced proliferative retinopathy, fibrous tissue or old scar tissue which develops from previous bleeds and can lead to retinal detachment and blindness.
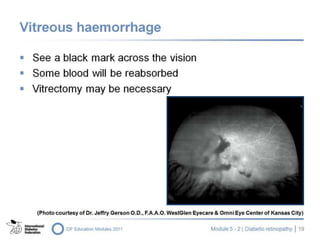
- #20: In the severest form of retinopathy a large bleed can occur into the vitreous body. People often report a black mark across their vision. Some of this blood will be reabsorbed but in the case of a dense and non-clearing bleed, vitrectomy will probably be considered within a few months to remove the blood-filled vitreous body.
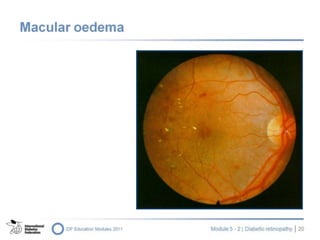
- #21: Macular oedema is the swelling of the macula; eyesight is reduced and laser therapy is required. In this situation, immediate referral to an ophthalmologist is essential. Recently, ophthalmologists have been using intra-vitreal injections of steroid in an attempt to reduce the oedema. Macula oedema is almost impossible to diagnose using direct ophthalmoscopy. While not strictly a grade of retinopathy many clinicians still use the term maculopathy to describe lesions near the macula. This is often associated with a decrease in visual acuity, can be vision threatening and needs to be reviewed by an expert in the area. Thiazolodinediones can exacerbate macular oedema and thus should be used with caution in people whom macular oedema is known or expected.
- #22: A fluorescein angiogram gives detailed information on the degree of severity of the retinopathy. The indications to do fluroescein angiography are: To locate new vessels Loss of some vision (decreasing visual acuity) Due to newer technology, fluorescein angiography is not used as often in some countries. OCT (Optical Coherence Tomography) is widely used for the diagnosis and especially for the follow up of the macular edema in diabetes
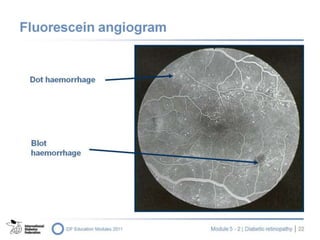
- #23: This is a picture of an eye following a fluorescein angiogram. The dot and blot haemorrhages appear much clearer.
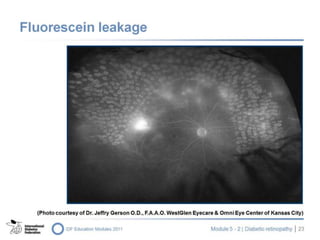
- #24: This slide shows the severe leakage from vessels across the whole retina.
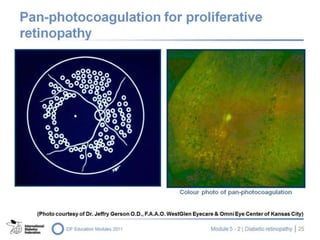
- #25: One of most important outcomes of these trials was the discovery that laser therapy has the potential to save sight. There are different laser treatments available to treat the different types of retinopathy. In proliferative retinopathy, pan- or pattern-retinal laser therapy is required. In macular oedema, focal or grid laser therapy is necessary.
- #26: This is an example of pan- or pattern-photocoagulation used in proliferative retinopathy. In other words, the periphery of the retina is targeted.
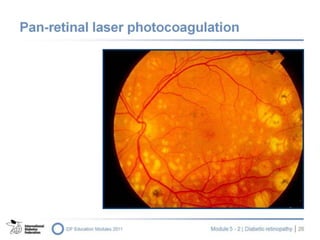
- #27: This slide shows a retina treated by laser for proliferative retinopathy. The yellow dots are laser burns.
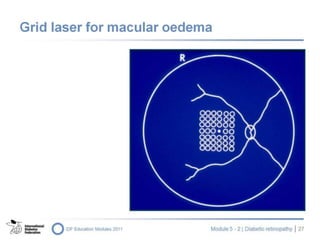
- #28: Grid or focal laser is required to target the lesions such as hard or soft exudates around the macula. In this situation, an ophthalmologist, very experienced in performing laser therapy, is required to ensure that the macula, and hence the vision, is preserved.
- #29: There are side effects from laser therapy that need to be discussed with the person. In pan- or pattern-bombing laser therapy for proliferative retinopathy, peripheral vision can be lost leading to night blindness. In this case, people should be advised not to drive at night. They will also find it more difficult to move from a light environment to a dark one (e.g. entering a movie theatre) as the eye which received laser treatment has less ability to adapt quickly to different light environments. In some countries loss of peripheral visual fields may result in loss of driverŌĆÖs license. Some people who undergo laser therapy will experience loss of colour perception. In fact, vision may deteriorate with laser therapy. However, the therapy does stop progression and can save sight in the long term.
- #30: There are several additional important aspects to the treatment of retinopathy. People with retinopathy require aggressive treatment of blood pressure. As seen in the DCCT, the follow-up EDIC Study and UKPDS and its Post Study Monitoring Study, it is important to improve blood glucose control. This helps to slow the progression of retinopathy. Any improvement in HbA1c levels has a positive effect on reducing the risk of development and/or progression of retinopathy. However, glycaemic control should be improved gradually because a rapid change in blood glucose levels can worsen the retinopathy. This may be transient or require treatment if haemorhage occurs. Lipids should be treated to target. Evidence indicates that the use of aspirin does not increase the risk of retinal bleeding and therefore can be used in retinopathy.
- #31: If available, medical therapies such as corticosteriods and antiVEGF injected directly into the eye (intravitreal) are used when further laser therapy is no longer feasible to treat the growth of new vessels or to reduce macular oedema. They have not been studied systematically in diabetes and currently are used as a "last resort" treatment. They have been reported to increase the progression of cataract especially with corticosteroid use. The most feared complication of intravitreal injections is the infection. Gillies, M.C., Simpson, J.M., Billson, F.A., Luo, W., Penfold, P., Chua, W., Mitchell, P., Zhu, M., Hunyor, A.B.L. (2004). Safety of an Intravitreal Injection of Triamcinolone : Results From a Randomized Clinical Trial. Arch Ophthalmol, 122, 336-340. Jorge, R., Costa, R.A., Calucci, D., Cintra, L.P., Scott, I.U. (2006). Intravitreal Bevacizumab (Avastin) for Persistent New Vessels in Diabetic Retinopathy (Ibepe Study). Retina, 26(9), 1006-1013. Elman M, Aiello L, Beck R, et al. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 27 April 2010
- #32: A special area of consideration is the influence of pregnancy on diabetic retinopathy. Pregnancy can cause transient deterioration of diabetic retinopathy, but generally does not cause permanent damage. Ideally a woman should have a baseline retinal assessment before becoming pregnant. If the pregnancy is not planned, retinal assessment should be performed as soon as possible. The retinal status of all women should be re-assessed in the second and third trimesters. Diabetic retinopathy does not occur in gestational diabetes.
- #33: In the older person, the presence of cataract and other age-related factors, such as smaller pupils, makes visualisation of the fundi more difficult. Cataract surgery may exacerbate macular oedema. It is thus very important that people have their retinae assessed following surgery. Visual outcome after cataract surgery largely depends on the preoperative severity of diabetic retinopathy and the presence of diabetic macular edema. In older people, NPDR with macular oedema is the main cause of visual loss.
- #34: The key lessons to remember are: 1. With time, most people with diabetes will develop some grade of retinopathy 2. Appropriate timely treatment, including laser therapy, has been shown unequivocally to save sight; if laser therapy is delivered when vision is still clear, the treatment is most effective 3. The most effective measure for prevention is to achieve recommended targets for blood pressure, lipids and blood glucose 4. As retinopathy is asymptomatic in its early stages, regular screening of the eyes by a practitioner who is experienced in diabetic eye disease annually where available is recommended. ADA 2010 Diabetes Care 33(Suppl 1).