Patient referral form1
0 likes570 views

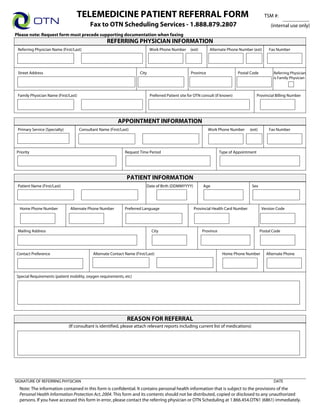
This Telemedicine Patient Referral Form contains fields for a referring physician to provide information about a patient they are referring for an OTN telemedicine consultation, including the patient's name, date of birth, contact details, primary service requested, and reason for referral. The form is to be faxed to OTN Scheduling Services to initiate a telemedicine appointment for the patient.
1 of 1
Download to read offline
Ad
Recommended
Dawn Cortazar resume (1)
Dawn Cortazar resume (1)Dawn Cortazar
Ěý
Dawn Cortazar is an experienced paralegal with skills in negotiation, conflict resolution, and easing tensions between parties. She has over 20 years of experience working in nursing homes and private nursing. Cortazar has an Associate's Degree in Paralegal Studies and is currently interning at two law firms, where her duties include document preparation, client communication, and legal research.Microsoft word june 15th agenda otn woundcare consult meeting
Microsoft word june 15th agenda otn woundcare consult meetingJenna Verenka
Ěý
This agenda outlines a woundcare consult meeting presented by Jenna Verenka at Linhaven, VWWH, and Shalom Village. The meeting will introduce the OTN Woundcare Consult Program and referral process, including who can be consulted and on what days and times. It will also cover the required clinical protocol for consults and leave time for questions and input on the protocol.Tm clinical protocol_outline1
Tm clinical protocol_outline1Jenna Verenka
Ěý
This document outlines the clinical protocol for telemedicine services at an unnamed organization. It includes sections on overview with inclusion and exclusion criteria, referral and scheduling procedures, preparation requirements for patients and the telemedicine studio at both the referring site and specialist site, and procedures for telemedicine sessions including obtaining consent, introducing participants, conducting examinations, making recommendations, and documenting follow-up plans. The protocol aims to standardize telemedicine visits and ensure patient privacy and continuity of care.Microsoft word june 15th agenda otn woundcare consult meeting
Microsoft word june 15th agenda otn woundcare consult meetingJenna Verenka
Ěý
This agenda outlines an OTN woundcare consult meeting to discuss the program's purpose and referral process, including who can be consulted and on what days. It also covers the required clinical protocol for consults and leaves time for questions and feedback on the protocol.Training otn woundcare poster june 2011
Training otn woundcare poster june 2011Jenna Verenka
Ěý
This document provides information about training workshops for submitting wound care referrals via videoconference. It lists the date, time, and event details for two workshops presented by Jenna Verenka, RN, from Shalom Villiage in Hamilton. The objectives of the workshops are to teach attendees how to submit new and follow-up consult referrals and what clinic information should be presented by wound care champions. The intended audience is long-term care homes participating in an RNAO pilot project. It provides instructions for sites to self-register or submit their information to reserve a videoconference room and system to participate.Bwat
BwatJenna Verenka
Ěý
The Bates-Jensen Wound Assessment Tool provides instructions for evaluating wounds based on 13 items: size, depth, edges, undermining, necrotic tissue type and amount, exudate type and amount, skin color surrounding wound, peripheral tissue edema/induration, granulation tissue, and epithelialization. Nurses are directed to rate each item by selecting the response that best describes the wound and calculating a total score, with higher scores indicating more severe wound status. Wound progress should be tracked by plotting total scores on the Wound Status Continuum.Patient camera qrg1
Patient camera qrg1Jenna Verenka
Ěý
The document provides start-up and operation procedures for the AMD-2500 general examination camera. [1] To start up the camera, plug in power and video cables, turn on the power and light switches, and set the autofocus feature. [2] For operation, buttons allow the user to turn off light polarization for better surface views, zoom in and out for close-up and overall views, and freeze images. [3] Technical support is available from the OTN Service Desk.2024 Trend Updates: What Really Works In SEO & Content Marketing
2024 Trend Updates: What Really Works In SEO & Content MarketingSearch Engine Journal
Ěý
The document outlines key SEO and content marketing trends for 2024, emphasizing the impact of AI, the importance of E-E-A-T (Experience, Expertise, Authoritativeness, Trustworthiness), and a shift towards user-centric content strategies. It advises against focusing on outdated trends like voice search and stresses the need for creating value-driven, authoritative content. Additionally, it highlights the need to leverage AI as a supportive tool rather than relying solely on it for content creation.Storytelling For The Web: Integrate Storytelling in your Design Process
Storytelling For The Web: Integrate Storytelling in your Design ProcessChiara Aliotta
Ěý
The document outlines a livestream presentation by Chiara Aliotta on integrating storytelling into web design to enhance user experiences. It covers the storytelling process for designers, emphasizing aspects such as understanding the audience, structuring narratives, and creating emotional connections. The presentation also includes case studies and practical examples to demonstrate effective storytelling in UX/UI design.Artificial Intelligence, Data and Competition – SCHREPEL – June 2024 OECD dis...
Artificial Intelligence, Data and Competition – SCHREPEL – June 2024 OECD dis...OECD Directorate for Financial and Enterprise Affairs
Ěý
This presentation by Thibault Schrepel, Associate Professor of Law at Vrije Universiteit Amsterdam University, was made during the discussion “Artificial Intelligence, Data and Competition” held at the 143rd meeting of the OECD Competition Committee on 12 June 2024. More papers and presentations on the topic can be found at oe.cd/aicomp.
This presentation was uploaded with the author’s consent.
How to Leverage AI to Boost Employee Wellness - Lydia Di Francesco - SocialHR...
How to Leverage AI to Boost Employee Wellness - Lydia Di Francesco - SocialHR...SocialHRCamp
Ěý
The document discusses leveraging AI to enhance employee wellness through data analytics, automating tasks, and personalized wellness apps, emphasizing the shared responsibility of employee well-being between leaders and organizations. It outlines best practices for using AI in wellness strategies, including ensuring data privacy and security, understanding employee needs, and promoting inclusivity. Lydia Di Francesco, a wellness specialist, shares insights to optimize workplace wellness strategy using AI-driven data analytics and encourages collaboration and transparency.2024 State of Marketing Report – by Hubspot
2024 State of Marketing Report – by HubspotMarius Sescu
Ěý
The State of Marketing 2024 report highlights the transformative impact of AI and automation, emphasizing the importance of personalization and engagement to drive growth in a competitive landscape. Marketers are focusing on optimizing budgets, leveraging social media for brand awareness, and utilizing AI tools to enhance efficiency across tasks. Key trends for 2024 include the rise of experiential marketing, content creation that meets user needs, and strengthened connections through personalized customer experiences.Everything You Need To Know About ChatGPT
Everything You Need To Know About ChatGPTExpeed Software
Ěý
ChatGPT is an AI chatbot developed by OpenAI, built on advanced language models to facilitate human-like conversational interactions. Launched in November 2022, it utilizes a transformer architecture to understand and generate text, with applications ranging from content creation to customer service. Despite its capabilities, there are concerns about potential misuse and biases in its responses, which OpenAI aims to mitigate through moderation and user feedback.Product Design Trends in 2024 | Teenage Engineerings
Product Design Trends in 2024 | Teenage EngineeringsPixeldarts
Ěý
The realm of product design is a constantly changing environment where technology and style intersect. Every year introduces fresh challenges and exciting trends that mold the future of this captivating art form. In this piece, we delve into the significant trends set to influence the look and functionality of product design in the year 2024.How Race, Age and Gender Shape Attitudes Towards Mental Health
How Race, Age and Gender Shape Attitudes Towards Mental HealthThinkNow
Ěý
The November 2023 mental health report indicates that 70% of respondents rate their mental health as 'good' or 'excellent,' with higher diagnoses reported among African Americans and non-Hispanic whites compared to Hispanics and Asians. Younger generations, particularly Gen Z and millennials, are more likely to experience mental health challenges, seek information online, and report that their mental health impacts their work and relationships. Half of the respondents feel comfortable discussing their mental health with professionals, although Gen Z shows the least comfort in this area.AI Trends in Creative Operations 2024 by Artwork Flow.pdf
AI Trends in Creative Operations 2024 by Artwork Flow.pdfmarketingartwork
Ěý
Creative operations teams expect increased AI use in 2024. Currently, over half of tasks are not AI-enabled, but this is expected to decrease in the coming year. ChatGPT is the most popular AI tool currently. Business leaders are more actively exploring AI benefits than individual contributors. Most respondents do not believe AI will impact workforce size in 2024. However, some inhibitions still exist around AI accuracy and lack of understanding. Creatives primarily want to use AI to save time on mundane tasks and boost productivity.Skeleton Culture Code
Skeleton Culture CodeSkeleton Technologies
Ěý
Organizational culture includes values, norms, systems, symbols, language, assumptions, beliefs, and habits that influence employee behaviors and how people interpret those behaviors. It is important because culture can help or hinder a company's success. Some key aspects of Netflix's culture that help it achieve results include hiring smartly so every position has stars, focusing on attitude over just aptitude, and having a strict policy against peacocks, whiners, and jerks.PEPSICO Presentation to CAGNY Conference Feb 2024
PEPSICO Presentation to CAGNY Conference Feb 2024Neil Kimberley
Ěý
PepsiCo provided a safe harbor statement noting that any forward-looking statements are based on currently available information and are subject to risks and uncertainties. It also provided information on non-GAAP measures and directing readers to its website for disclosure and reconciliation. The document then discussed PepsiCo's business overview, including that it is a global beverage and convenient food company with iconic brands, $91 billion in net revenue in 2023, and nearly $14 billion in core operating profit. It operates through a divisional structure with a focus on local consumers.Content Methodology: A Best Practices Report (Webinar)
Content Methodology: A Best Practices Report (Webinar)contently
Ěý
This document provides an overview of content methodology best practices. It defines content methodology as establishing objectives, KPIs, and a culture of continuous learning and iteration. An effective methodology focuses on connecting with audiences, creating optimal content, and optimizing processes. It also discusses why a methodology is needed due to the competitive landscape, proliferation of channels, and opportunities for improvement. Components of an effective methodology include defining objectives and KPIs, audience analysis, identifying opportunities, and evaluating resources. The document concludes with recommendations around creating a content plan, testing and optimizing content over 90 days.How to Prepare For a Successful Job Search for 2024
How to Prepare For a Successful Job Search for 2024Albert Qian
Ěý
The document provides guidance on preparing a job search for 2024. It discusses the state of the job market, focusing on growth in AI and healthcare but also continued layoffs. It recommends figuring out what you want to do by researching interests and skills, then conducting informational interviews. The job search should involve building a personal brand on LinkedIn, actively applying to jobs, tailoring resumes and interviews, maintaining job hunting as a habit, and continuing self-improvement. Once hired, the document advises setting new goals and keeping skills and networking active in case of future opportunities.Social Media Marketing Trends 2024 // The Global Indie Insights
Social Media Marketing Trends 2024 // The Global Indie InsightsKurio // The Social Media Age(ncy)
Ěý
The 2024 social media marketing trends report highlights significant shifts influenced by generative AI, including the emergence of personalized content, the rise of virtual influencers, and a stronger focus on user-generated content. Insights were gathered from 33 experts across 23 leading independent agencies, providing a perspective that emphasizes creativity and authenticity in marketing strategies. Key trends also include the blending of B2B and B2C approaches, reflecting changes in consumer behavior and the evolving landscape of social media engagement.Trends In Paid Search: Navigating The Digital Landscape In 2024
Trends In Paid Search: Navigating The Digital Landscape In 2024Search Engine Journal
Ěý
The document discusses trends in paid search for 2024, highlighting changes in user behavior, the implications for financial services, and privacy challenges. It emphasizes the importance of adapting search strategies, utilizing AI-driven tools like performance max and smart bidding, and leveraging first-party data for better marketing efficacy. Key takeaways include holistic SEO and SEM approaches, monitoring shifting user intents, and the need for continuous performance evaluation.5 Public speaking tips from TED - Visualized summary
5 Public speaking tips from TED - Visualized summarySpeakerHub
Ěý
The document outlines five public speaking tips from Chris Anderson, TED Talks curator, emphasizing the importance of eye contact, vulnerability, humor, humility, and storytelling. These skills are presented as essential for engaging audiences effectively and are increasingly valuable in today's economy. The article posits that mastering these techniques can enhance speakers' ability to communicate ideas powerfully.ChatGPT and the Future of Work - Clark Boyd
ChatGPT and the Future of Work - Clark Boyd Clark Boyd
Ěý
The document provides an overview of generative AI, particularly focusing on ChatGPT and its implications for business and the job market. It discusses the rapid growth of generative AI, its applications in marketing, and the skills needed for the AI era while addressing potential job displacement and the need for adaptation. The agenda includes a Q&A session and emphasizes rethinking work in collaboration with AI technology.Getting into the tech field. what next
Getting into the tech field. what next Tessa Mero
Ěý
The document provides career advice for getting into the tech field, including:
- Doing projects and internships in college to build a portfolio.
- Learning about different roles and technologies through industry research.
- Contributing to open source projects to build experience and network.
- Developing a personal brand through a website and social media presence.
- Networking through events, communities, and finding a mentor.
- Practicing interviews through mock interviews and whiteboarding coding questions.Google's Just Not That Into You: Understanding Core Updates & Search Intent
Google's Just Not That Into You: Understanding Core Updates & Search IntentLily Ray
Ěý
1. Core updates from Google periodically change how its algorithms assess and rank websites and pages. This can impact rankings through shifts in user intent, site quality issues being caught up to, world events influencing queries, and overhauls to search like the E-A-T framework.
2. There are many possible user intents beyond just transactional, navigational and informational. Identifying intent shifts is important during core updates. Sites may need to optimize for new intents through different content types and sections.
3. Responding effectively to core updates requires analyzing "before and after" data to understand changes, identifying new intents or page types, and ensuring content matches appropriate intents across video, images, knowledge graphs and more.How to have difficult conversations
How to have difficult conversations Rajiv Jayarajah, MAppComm, ACC
Ěý
The document provides essential tips on how to handle difficult conversations in a workplace setting, emphasizing the importance of preparation, environment, and timing. It highlights that many employees dread such conversations, often leading to avoidance and worsening situations. Ultimately, the guide aims to promote positive outcomes while maintaining professional relationships.Introduction to Data Science
Introduction to Data ScienceChristy Abraham Joy
Ěý
The document discusses the rise and importance of data science and machine learning, highlighting the growing demand for data scientists and the challenges they face. It explains machine learning concepts such as supervised and unsupervised learning, along with various real-world applications and the necessary steps involved in a machine learning workflow. Additionally, the document emphasizes the iterative process of model improvement and feature engineering used to enhance machine learning outcomes.More Related Content
Featured (20)
Storytelling For The Web: Integrate Storytelling in your Design Process
Storytelling For The Web: Integrate Storytelling in your Design ProcessChiara Aliotta
Ěý
The document outlines a livestream presentation by Chiara Aliotta on integrating storytelling into web design to enhance user experiences. It covers the storytelling process for designers, emphasizing aspects such as understanding the audience, structuring narratives, and creating emotional connections. The presentation also includes case studies and practical examples to demonstrate effective storytelling in UX/UI design.Artificial Intelligence, Data and Competition – SCHREPEL – June 2024 OECD dis...
Artificial Intelligence, Data and Competition – SCHREPEL – June 2024 OECD dis...OECD Directorate for Financial and Enterprise Affairs
Ěý
This presentation by Thibault Schrepel, Associate Professor of Law at Vrije Universiteit Amsterdam University, was made during the discussion “Artificial Intelligence, Data and Competition” held at the 143rd meeting of the OECD Competition Committee on 12 June 2024. More papers and presentations on the topic can be found at oe.cd/aicomp.
This presentation was uploaded with the author’s consent.
How to Leverage AI to Boost Employee Wellness - Lydia Di Francesco - SocialHR...
How to Leverage AI to Boost Employee Wellness - Lydia Di Francesco - SocialHR...SocialHRCamp
Ěý
The document discusses leveraging AI to enhance employee wellness through data analytics, automating tasks, and personalized wellness apps, emphasizing the shared responsibility of employee well-being between leaders and organizations. It outlines best practices for using AI in wellness strategies, including ensuring data privacy and security, understanding employee needs, and promoting inclusivity. Lydia Di Francesco, a wellness specialist, shares insights to optimize workplace wellness strategy using AI-driven data analytics and encourages collaboration and transparency.2024 State of Marketing Report – by Hubspot
2024 State of Marketing Report – by HubspotMarius Sescu
Ěý
The State of Marketing 2024 report highlights the transformative impact of AI and automation, emphasizing the importance of personalization and engagement to drive growth in a competitive landscape. Marketers are focusing on optimizing budgets, leveraging social media for brand awareness, and utilizing AI tools to enhance efficiency across tasks. Key trends for 2024 include the rise of experiential marketing, content creation that meets user needs, and strengthened connections through personalized customer experiences.Everything You Need To Know About ChatGPT
Everything You Need To Know About ChatGPTExpeed Software
Ěý
ChatGPT is an AI chatbot developed by OpenAI, built on advanced language models to facilitate human-like conversational interactions. Launched in November 2022, it utilizes a transformer architecture to understand and generate text, with applications ranging from content creation to customer service. Despite its capabilities, there are concerns about potential misuse and biases in its responses, which OpenAI aims to mitigate through moderation and user feedback.Product Design Trends in 2024 | Teenage Engineerings
Product Design Trends in 2024 | Teenage EngineeringsPixeldarts
Ěý
The realm of product design is a constantly changing environment where technology and style intersect. Every year introduces fresh challenges and exciting trends that mold the future of this captivating art form. In this piece, we delve into the significant trends set to influence the look and functionality of product design in the year 2024.How Race, Age and Gender Shape Attitudes Towards Mental Health
How Race, Age and Gender Shape Attitudes Towards Mental HealthThinkNow
Ěý
The November 2023 mental health report indicates that 70% of respondents rate their mental health as 'good' or 'excellent,' with higher diagnoses reported among African Americans and non-Hispanic whites compared to Hispanics and Asians. Younger generations, particularly Gen Z and millennials, are more likely to experience mental health challenges, seek information online, and report that their mental health impacts their work and relationships. Half of the respondents feel comfortable discussing their mental health with professionals, although Gen Z shows the least comfort in this area.AI Trends in Creative Operations 2024 by Artwork Flow.pdf
AI Trends in Creative Operations 2024 by Artwork Flow.pdfmarketingartwork
Ěý
Creative operations teams expect increased AI use in 2024. Currently, over half of tasks are not AI-enabled, but this is expected to decrease in the coming year. ChatGPT is the most popular AI tool currently. Business leaders are more actively exploring AI benefits than individual contributors. Most respondents do not believe AI will impact workforce size in 2024. However, some inhibitions still exist around AI accuracy and lack of understanding. Creatives primarily want to use AI to save time on mundane tasks and boost productivity.Skeleton Culture Code
Skeleton Culture CodeSkeleton Technologies
Ěý
Organizational culture includes values, norms, systems, symbols, language, assumptions, beliefs, and habits that influence employee behaviors and how people interpret those behaviors. It is important because culture can help or hinder a company's success. Some key aspects of Netflix's culture that help it achieve results include hiring smartly so every position has stars, focusing on attitude over just aptitude, and having a strict policy against peacocks, whiners, and jerks.PEPSICO Presentation to CAGNY Conference Feb 2024
PEPSICO Presentation to CAGNY Conference Feb 2024Neil Kimberley
Ěý
PepsiCo provided a safe harbor statement noting that any forward-looking statements are based on currently available information and are subject to risks and uncertainties. It also provided information on non-GAAP measures and directing readers to its website for disclosure and reconciliation. The document then discussed PepsiCo's business overview, including that it is a global beverage and convenient food company with iconic brands, $91 billion in net revenue in 2023, and nearly $14 billion in core operating profit. It operates through a divisional structure with a focus on local consumers.Content Methodology: A Best Practices Report (Webinar)
Content Methodology: A Best Practices Report (Webinar)contently
Ěý
This document provides an overview of content methodology best practices. It defines content methodology as establishing objectives, KPIs, and a culture of continuous learning and iteration. An effective methodology focuses on connecting with audiences, creating optimal content, and optimizing processes. It also discusses why a methodology is needed due to the competitive landscape, proliferation of channels, and opportunities for improvement. Components of an effective methodology include defining objectives and KPIs, audience analysis, identifying opportunities, and evaluating resources. The document concludes with recommendations around creating a content plan, testing and optimizing content over 90 days.How to Prepare For a Successful Job Search for 2024
How to Prepare For a Successful Job Search for 2024Albert Qian
Ěý
The document provides guidance on preparing a job search for 2024. It discusses the state of the job market, focusing on growth in AI and healthcare but also continued layoffs. It recommends figuring out what you want to do by researching interests and skills, then conducting informational interviews. The job search should involve building a personal brand on LinkedIn, actively applying to jobs, tailoring resumes and interviews, maintaining job hunting as a habit, and continuing self-improvement. Once hired, the document advises setting new goals and keeping skills and networking active in case of future opportunities.Social Media Marketing Trends 2024 // The Global Indie Insights
Social Media Marketing Trends 2024 // The Global Indie InsightsKurio // The Social Media Age(ncy)
Ěý
The 2024 social media marketing trends report highlights significant shifts influenced by generative AI, including the emergence of personalized content, the rise of virtual influencers, and a stronger focus on user-generated content. Insights were gathered from 33 experts across 23 leading independent agencies, providing a perspective that emphasizes creativity and authenticity in marketing strategies. Key trends also include the blending of B2B and B2C approaches, reflecting changes in consumer behavior and the evolving landscape of social media engagement.Trends In Paid Search: Navigating The Digital Landscape In 2024
Trends In Paid Search: Navigating The Digital Landscape In 2024Search Engine Journal
Ěý
The document discusses trends in paid search for 2024, highlighting changes in user behavior, the implications for financial services, and privacy challenges. It emphasizes the importance of adapting search strategies, utilizing AI-driven tools like performance max and smart bidding, and leveraging first-party data for better marketing efficacy. Key takeaways include holistic SEO and SEM approaches, monitoring shifting user intents, and the need for continuous performance evaluation.5 Public speaking tips from TED - Visualized summary
5 Public speaking tips from TED - Visualized summarySpeakerHub
Ěý
The document outlines five public speaking tips from Chris Anderson, TED Talks curator, emphasizing the importance of eye contact, vulnerability, humor, humility, and storytelling. These skills are presented as essential for engaging audiences effectively and are increasingly valuable in today's economy. The article posits that mastering these techniques can enhance speakers' ability to communicate ideas powerfully.ChatGPT and the Future of Work - Clark Boyd
ChatGPT and the Future of Work - Clark Boyd Clark Boyd
Ěý
The document provides an overview of generative AI, particularly focusing on ChatGPT and its implications for business and the job market. It discusses the rapid growth of generative AI, its applications in marketing, and the skills needed for the AI era while addressing potential job displacement and the need for adaptation. The agenda includes a Q&A session and emphasizes rethinking work in collaboration with AI technology.Getting into the tech field. what next
Getting into the tech field. what next Tessa Mero
Ěý
The document provides career advice for getting into the tech field, including:
- Doing projects and internships in college to build a portfolio.
- Learning about different roles and technologies through industry research.
- Contributing to open source projects to build experience and network.
- Developing a personal brand through a website and social media presence.
- Networking through events, communities, and finding a mentor.
- Practicing interviews through mock interviews and whiteboarding coding questions.Google's Just Not That Into You: Understanding Core Updates & Search Intent
Google's Just Not That Into You: Understanding Core Updates & Search IntentLily Ray
Ěý
1. Core updates from Google periodically change how its algorithms assess and rank websites and pages. This can impact rankings through shifts in user intent, site quality issues being caught up to, world events influencing queries, and overhauls to search like the E-A-T framework.
2. There are many possible user intents beyond just transactional, navigational and informational. Identifying intent shifts is important during core updates. Sites may need to optimize for new intents through different content types and sections.
3. Responding effectively to core updates requires analyzing "before and after" data to understand changes, identifying new intents or page types, and ensuring content matches appropriate intents across video, images, knowledge graphs and more.How to have difficult conversations
How to have difficult conversations Rajiv Jayarajah, MAppComm, ACC
Ěý
The document provides essential tips on how to handle difficult conversations in a workplace setting, emphasizing the importance of preparation, environment, and timing. It highlights that many employees dread such conversations, often leading to avoidance and worsening situations. Ultimately, the guide aims to promote positive outcomes while maintaining professional relationships.Introduction to Data Science
Introduction to Data ScienceChristy Abraham Joy
Ěý
The document discusses the rise and importance of data science and machine learning, highlighting the growing demand for data scientists and the challenges they face. It explains machine learning concepts such as supervised and unsupervised learning, along with various real-world applications and the necessary steps involved in a machine learning workflow. Additionally, the document emphasizes the iterative process of model improvement and feature engineering used to enhance machine learning outcomes.Artificial Intelligence, Data and Competition – SCHREPEL – June 2024 OECD dis...
Artificial Intelligence, Data and Competition – SCHREPEL – June 2024 OECD dis...OECD Directorate for Financial and Enterprise Affairs
Ěý
Patient referral form1
- 1. TELEMEDICINE PATIENT REFERRAL FORM TSM #: Fax to OTN Scheduling Services - 1.888.879.2807 (internal use only) Please note: Request form must precede supporting documentation when faxing Print Form REFERRING PHYSICIAN INFORMATION Referring Physician Name (First/Last) Work Phone Number (ext) Alternate Phone Number (ext) Fax Number Street Address City Province Postal Code Referring Physician is Family Physician Ontario Family Physician Name (First/Last) Preferred Patient site for OTN consult (if known) Provincial Billing Number APPOINTMENT INFORMATION Primary Service (Specialty) Consultant Name (First/Last) Work Phone Number (ext) Fax Number Priority Request Time Period Type of Appointment PATIENT INFORMATION Patient Name (First/Last) Date of Birth (DDMMYYYY) Age Sex Home Phone Number Alternate Phone Number Preferred Language Provincial Health Card Number Version Code Mailing Address City Province Postal Code Ontario Contact Preference Alternate Contact Name (First/Last) Home Phone Number Alternate Phone Special Requirements (patient mobility, oxygen requirements, etc) REASON FOR REFERRAL (If consultant is identified, please attach relevant reports including current list of medications) SIGNATURE OF REFERRING PHYSICIAN DATE Note: The information contained in this form is confidential. It contains personal health information that is subject to the provisions of the Personal Health Information Protection Act, 2004. This form and its contents should not be distributed, copied or disclosed to any unauthorized persons. If you have accessed this form in error, please contact the referring physician or OTN Scheduling at 1.866.454.OTN1 (6861) immediately.