


















![(4)=(2)-(3)
自然悪化なかり
せば基準時間
(分)
(5)
純改善
時間
(分)
(6)
自立支援介護
サービス提供
時間(分/
月)
(7)
自立支援介護
サービス提供
時間(1週当り
平均分数)
(8)=a*(7)*(1)
区間別回帰直線
(9)
回帰直線
(10)=[(5)-(9)]^2
区間別残差分散
48.2 0.0 0.0 0.0
975
780
46.9 1.3 780 3.25 6.6 6.6 28.7
975
780
24.4 23.8 780 3.25 6.6 13.2 111.9
975
780
23.1 25.1 585 2.97 6.1 19.3 33.0
780
780
21.8 26.4 975 3.21 6.6 26.0 0.2
202020/1/31
年月日 (1)
区間週数
20150901
20151001
20151101
20151201 13
20160101
20160201
20160301 13
20160401
20160501
20160601 13.14
20160701
20160801
20160901 13.14
サービス提供実績
区間週数 1週間当りサービス提供時間 ?
残差分散を最小化する
回帰係数 を求める?
残差分散
区間別回帰
直線の累積
残差分散
実際の計算例
要介護認定一次判定項目の一部を用いた要介護改善の推計例](https://image.slidesharecdn.com/20200131astem-200211072507/85/-21-320.jpg)

































More Related Content
Similar to 要介护高齢者の自立支援型介护の効果と介护事业者へのインセンティブメカニズム (18)
要介护高齢者の自立支援型介护の効果と介护事业者へのインセンティブメカニズム
- 3. 22020/1/31 インセンティブ理論とは プリンシパル=エージェント問題(エージェンシー問題)を扱う理論 売上 労働量 プリンシパル(雇用主) エージェント(従業員) 機会費用 報酬 純効用 l エージェントは純効用を最大化するよ うに,労働量を決めたい l プリンシパルは利益を最大化したい 利益 余暇,高い報酬が得られ るかもしれない仕事 ? 売上を最大化するようにエージェ ントに最大限の努力(労働量)を させつつ,利益を最大化できる報 酬水準を決めたい
- 4. 32020/1/31 インセンティブ理論とは 問題の所在 l 報酬は売上に連動したものにしたい. l 売上はエージェントがどれだけ一生懸命働 いたか,つまり努力したかに依るので,報 酬はエージェントに最大限の努力を動機づ けるものにしたい. プリンシパル側 エージェント側 l プリンシパルはエージェントがどれだけ努 力しているか分からない. l 労働時間に応じて報酬を支払うと,エー ジェントは努力はしないかもしれない. l どれだけ努力しても,不可抗力の要因に よって売上は減少するリスクがあるので, 報酬が売上に連動するのは困る. l 労働時間に応じた報酬にして欲しい. リスク分担の問題 情報の非対称性?モラルハザードの問題 インセンティブ理論は,これらの問題 を数理モデルを用いて解析し,最適解 を求めるもの 動機づけの問題
- 5. 0 1,000 2,000 3,000 4,000 5,000 6,000 7,000 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 要介護(要支援)認定者数の推移 要支援1 要支援2 経過的要介護 要介護1 要介護2 要介護3 要介護4 要介護5 高齢化に伴い要介護者は年々増加 42020/1/31 (千人) 6,203 2,562 2,983 3,445 3,480 4,086 4,324 4,400 4,529 4,673 4,846 5,063 5,305 5,611 5,838 6,0585.5% per year 高齢化に伴い,要介護 者も年々増加 介護保険制度が開始し た2000年から2017ま でに,要介護認定者数 は約400万人の増(年 率5.5%) 6,320 6,412 Masaru Unno
- 6. 32,427 41,143 46,576 50,990 55,594 57,943 58,743 61,600 64,185 68,721 72,536 76,298 81,283 85,121 89,005 90,976 92,290 94,443 0 10,000 20,000 30,000 40,000 50,000 60,000 70,000 80,000 90,000 100,000 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 年度別給付費の推移 介護費用も年々増加 52020/1/31 (億円) 9兆円 介護費用も年々増加を続 け,このまま増加を続け れば,財政的に介護保険 制度を維持することが困 難になるおそれも Masaru Unno
- 8. 先行研究 72020/1/31 Original Study Economic Evaluation of a Multifactorial, Interdisciplinary Intervention Versus Usual Care to Reduce Frailty in Frail Older People Nicola Fairhall PhD a , Catherine Sherrington PhD b , Susan E. Kurrle MBBS, PhD c , Stephen R. Lord PhD d , Keri Lockwood BHSci c , Kirsten Howard PhD e , Alison Hayes PhD e , Noeline Monaghan MSc, Dip Law a , Colleen Langron MHSci c , Christina Aggar PhD f , Ian D. Cameron MBBS, PhD a, * a Rehabilitation Studies Unit, Faculty of Medicine, The University of Sydney, Sydney, Australia b The George Institute for Global Health, The University of Sydney, Sydney, Australia c Rehabilitation and Aged Care Services, Hornsby Ku-ring-gai Hospital, Sydney, Australia d Neuroscience Research Australia, University of New South Wales, Sydney, Australia e Sydney School of Public Health, Faculty of Medicine, The University of Sydney, Sydney, Australia f Faculty of Nursing and Midwifery, The University of Sydney, Sydney, Australia Keywords: Frailty randomized controlled trial cost-effectiveness a b s t r a c t Objective: To compare the costs and cost-effectiveness of a multifactorial interdisciplinary intervention versus usual care for older people who are frail. Design: Cost-effectiveness study embedded within a randomized controlled trial. Setting: Community-based intervention in Sydney, Australia. Participants: A total of 241 community-dwelling people 70 years or older who met the Cardiovascular Health Study criteria for frailty. Intervention: A 12-month multifactorial, interdisciplinary intervention targeting identi?ed frailty char- acteristics versus usual care. Measurements: Health and social service use, frailty, and health-related quality of life (EQ-5D) were measured over the 12-month intervention period. The difference between the mean cost per person for 12 months in the intervention and control groups (incremental cost) and the ratio between incremental cost and effectiveness were calculated. Results: A total of 216 participants (90%) completed the study. The prevalence of frailty was 14.7% lower in the intervention group compared with the control group at 12 months (95% CI 2.4%e27.0%; P ? .02). There was no signi?cant between-group difference in EQ-5D utility scores. The cost for 1 extra person to transition out of frailty was $A15,955 (at 2011 prices). In the “very frail” subgroup (participants met >3 Cardiovascular Health Study frailty criteria), the intervention was both more effective and less costly than the control. A cost-effectiveness acceptability curve shows that the intervention would be cost-effective with 80% certainty if decision makers were willing to pay $A50,000 per extra person transitioning from frailty. In the very frail subpopulation, this reduced to $25,000. Conclusion: For frail older people residing in the community, a 12-month multifactorial intervention provided better value for money than usual care, particularly for the very frail, in whom it has a high probability of being cost saving, as well as effective. ? 2015 AMDA e The Society for Post-Acute and Long-Term Care Medicine. JAMDA journal homepage: www.jamda.com Fairhall et al.(2015)が,216名の 要介護者に対して運動や食事コント ロールなどの複合的介入を行った結 果,通常介護を行った比較群と比べ 要介護状態(frailty)が14.7%改善 し,かつ50,000豪州ドルを追加的 に支出することで信頼度80%で介入 を行なう方が費用対効果を見込める と報告. Masaru Unno
- 10. 成果型報酬による動機づけ問題の解決 92020/1/31 この問題は,要介護度が改善した場合に成果型報酬を支払うという仕組みを導入することで,解決できる可能性. これは,自立支援型介護サービスによって要介護度が改善したときに,要介護度改善に伴う減収分と自立支援型 介護に要する追加的コストの合計額以上の報酬を介護事業者に支払うというもの. 改善 悪化 要介護度 評価開始時点 改善した対象者の改善 度に応じて,報酬を支 払い Aさん Bさん Cさん Dさん 改善しなかったCさん については報酬は支 払われない
- 13. 生活環境,既往症 等の個人属性 体調,メンタル面の変 化等による要介護度の 不規則な変動 要介護度の改善度合いに影響を与える要因を分析 時点 の 要介護状態 単位時間あたりの自立 支援型介護提供量 ? 要介護状態の変化量 AB C 122020/1/31 D E ? ? 時点 の 要介護状態 ? ? ? ?? = ? ? ? ? ? 要介護度の改善度合い( )は,自立支援型介護の単位時間当たり提供量( ),個人属性( ),老化によ る自然な悪化( ),不規則な変動( )に依存する. A B C D E リスク分担の問題 老化による要介護 度の自然な悪化
- 14. 介護事業者のリスク補償を含めた成果型報酬 132020/1/31 成果型報酬を適切に決め ることで,介護事業者に 最適な自立支援型介護 サービスを提供するよう 動機づけることが可能. ? 事業者は利益を最大化 するように自立支援型 介護サービスを提供. ? 成果型報酬を変動させ れば,事業者はサービ ス提供量を変化させる. ? 報酬を適切な水準に設 定すれば,事業者に適 切なサービスを提供さ せることができる. 要介護 高齢者 介護事業者 行政 成果型報酬 追加的コスト 介護報酬の減 リスクの補償 利 益 要介護度改善 要介護度改善 将来に渡って 抑制?削減 される介護 費用 利益を最大化す るように提供量 をコントロール 介護費用削減額か ら報酬を減じた残 余額を最大化する ような提供量を動 機づける報酬額を 支払い
- 16. 成果型報酬の仕組みが有効に機能するためには 152020/1/31 成果型報酬の仕組みが有効に機能するためには, 自立支援型介護の要介護度改善に対する有効性の検証と,その効果の定量化 が必要.具体的には, (1) 成果を適切に評価する方法論の確立 ? 自立支援型介護の手法や提供量等に応じた KPI改善度を統計的に解析し,効果を定量 化 (2) 手法や提供量に応じた効果の定量化 自立支援型介護の具体的なサービス項目が 各KPIの改善に与える影響を推定 ? 要介護度の改善度合いに関する評価指標 (KPI) ? 評価基準(各KPIの値がいくら以上なら成 果があったと判断するか,その閾値)
- 17. 要介護度の改善度合いに関するKPI 162020/1/31 KPIとして最も望ましいのは「要介護度」そのものだが,2年毎にしか更新されない,離散的な評価段階であるな どの点から,必ずしも適切とは言えない. 要介護度を代替するKPIとしては, (1) 要介護認定の一次判定項目のうち,自立支援型介 護の効果を評価するのに適した項目に限定し,よ り短い時間間隔(3ヶ月毎等)で測定 ? 自立支援型介護が主にADL/IADL改善に主眼を 置いていることから,一次判定項目の第1群およ び第2群の項目の全て若しくは一部を採用 ? KPIとしては,要介護認定一次判定と同様の基準 時間とする ? KPIの計算は,例えば,他の項目が直前の要介護 認定(更新)と変化がないものとして,一次判定 と同じロジックで基準時間を求める,等 (2) バーセルインデックス(BI)(ADL加算の 計算に用いられている) (3) 個別機能訓練にかかるアセスメント項目 (厚労省雛形の居宅訪問チェックシート記 載の項目) (4) 体力測定 握力,開眼片足立ち, TUG(Timed Up & Go Test),等
- 18. 個人属性 自立支援型介護(介入) 要介護度のKPI(状態) デモグラフィック 疾患(既往症) 栄養?水分管理等 栄養状態 ADL/IADL/起居動作 に関する評価 (居宅訪問チェック) 運動能力テスト結果 おむつ利用 下剤使用 QOL バーセルインデックス (観測困難な要因の解析が課題) 本人のモチベーション 家族の理解?支援 ...在宅の生活 自立支援型介護の手法や提供量等に応じたKPI改善度を統計的に解析し,効果を定量化する. 以下のような構造を仮定し,自立支援型介護の各項目の提供量と各KPI改善度合いに関する時系列データから,自立支援型介 護の効果を推定する. 172020/1/31 要介護認定情報 介護レセプト ? サービス別利用日数, 回数 ? 加算(個別機能訓練加 算等) ? TUG ? FR ? 開眼片足立ち 等 要介護認定情報 ? 全項目 若しくは ? ADL/IADL関連 項目のみ 体調,メンタル面の変化等 による自立支援型介護効果 の不規則な変動 加算以外の機能訓練 手法や提供量に応じた効果の定量化
- 19. 182020/1/31 一部の項目を用い, 一次判定ロジックに 従って基準時間を算定 一次判定項目 身体機能? 起居動作 社会生活 への適応 生活機能 認知機能 精神?行動 障害 麻痺の種類 拘縮 視力 聴力 移乗 移動 ズボン等の着脱 外出頻度 意思の伝達 外出して戻れない 毎日の日課を理解 被害的 ~ ~ ~ 作話 自分勝手に行動する 話がまとまらない 薬の内服 簡単な調理 ~ ~ 中間評価 分類 評価項目 評価項目得点 基準時間の算定ロジック 樹形モデル 時間の表示範囲 食事 排泄 1.1分~71.4分 0.2分~28.0分 移動 0.4分~21.4分 直接生活 介助 清潔保持 1.2分~24.3分 間接生活介助 0.4分~11.3分 BPSD関連行為 5.8分~21.2分 機能訓練関連行為 0.5分~15.4分 医療関連行為 1.0分~37.2分 自立と設定 自立と設定 55項目 21項目 要介護認定一次判定項目の一部を用いた要介護改善の推計例
- 20. 192020/1/31 実際の計算例 評価期間のスタート時点 スタート時点から基準時間 の改善分(=減少分) 年月日 (1) 区間週数 (2) 基準時間 (3) 自然悪化 (δ) (4)=(2)-(3) 自然悪化なかり せば基準時間 (分) (5) 純改善 時間 (分) 20150901 48.2 0.0 48.2 0.0 20151001 20151101 20151201 13 48.2 1.3 46.9 1.3 20160101 20160201 20160301 13 26.9 2.5 24.4 23.8 20160401 20160501 20160601 13.14 26.9 3.8 23.1 25.1 20160701 20160801 20160901 13.14 26.9 5.1 21.8 26.4 要介護認定等基準時間(注) 自然な要介護状態悪化 ? 要介護認定一次判定項目の一部を用いた要介護改善の推計例 (注)第3群~第5群の項目は 自立と評価しているため, 基準時間は実際の本人の ものより短くなる.
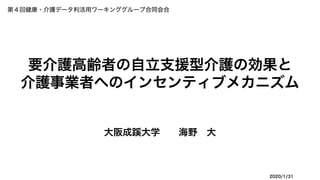
- 21. (4)=(2)-(3) 自然悪化なかり せば基準時間 (分) (5) 純改善 時間 (分) (6) 自立支援介護 サービス提供 時間(分/ 月) (7) 自立支援介護 サービス提供 時間(1週当り 平均分数) (8)=a*(7)*(1) 区間別回帰直線 (9) 回帰直線 (10)=[(5)-(9)]^2 区間別残差分散 48.2 0.0 0.0 0.0 975 780 46.9 1.3 780 3.25 6.6 6.6 28.7 975 780 24.4 23.8 780 3.25 6.6 13.2 111.9 975 780 23.1 25.1 585 2.97 6.1 19.3 33.0 780 780 21.8 26.4 975 3.21 6.6 26.0 0.2 202020/1/31 年月日 (1) 区間週数 20150901 20151001 20151101 20151201 13 20160101 20160201 20160301 13 20160401 20160501 20160601 13.14 20160701 20160801 20160901 13.14 サービス提供実績 区間週数 1週間当りサービス提供時間 ? 残差分散を最小化する 回帰係数 を求める? 残差分散 区間別回帰 直線の累積 残差分散 実際の計算例 要介護認定一次判定項目の一部を用いた要介護改善の推計例
- 22. 介入量 -10 0 10 20 30 40 50 2015/4/6 2015/7/15 2015/10/23 2016/1/31 2016/5/10 2016/8/18 2016/11/26 p00000003 state_normalized regression_line 実績 線形回帰直線 利用者毎の1週間当り利用 時間(=自立支援介護提供 時間)を介入量とする. 右グラフでは,利用時間当 りの要介護状態変化量の実 績値を求め,これを線形回 帰して,傾き を求める.? 測定区間内に実際に提供した サービス時間 ? good worse 状態 要介護認定一次判定のロ ジックに従い,ポラリスで 記録している「身体機能? 起居動作」「生活機能」を 中心とした測定値のみで基 本時間を計算し,基本時間 の変化を要介護状態の変化 量とする. ? ? ? ? 212020/1/31 要介護認定一次判定項目の一部を用いた要介護改善の推計例
- 23. その前提として,データベースが必要です 222020/1/31 電子カルテ 薬歴 レセプトデータ(医療) DPCデータ 検診データ 要介護認定情報 レセプトデータ(介護) ケアプラン 介護記録 統合データベース 電子お薬手帳 健康アプリ 生涯PHRアプリ PHRデータベース 連携 ü データの包括性 ü データの適正性 ü 二次利用可能性 ü 個人情報保護 医療機関?薬局 介護施設 本人?家族
- 27. データ活用による新たなサービス開発 262020/1/31 胎 児 期 乳 幼 児 期 少 年 期 青 年 期 中年期 老年期 生活習慣病 フレイル 要支援 要介護 維持? 改善? 自立へ公的保険,公的事業 による支援 民間(公的保険外)サービスによる介護予防,自立支援サービス ? データ活用,ITによる自立支援 型介護の手法開発,改善 ? 公的保険における成果型報酬の仕組みをレバレッジ とした自立支援型介護サービス市場の創造