































More Related Content
What's hot (6)
Similar to Sulfonamidesssr2020 200528142847 (20)




Recently uploaded (20)




















Sulfonamidesssr2020 200528142847
- 2. Learning Outcome At the end of the session student should be able to: ?Classify the Sulfonamides. ?Explain the mechanism of action, therapeutic uses, adverse effects* of clinically useful Sulfonamides ?Explain the rationale of combination of sulfamethoxazole and Trimethoprim in Cotrimoxazole Sulfonamides/ SSRMC/2020 2
- 3. ? First antimicrobial agent effective against pyogenic bacterial infection ? Scientist-DOMAGK ? PRONTOSIL RED DYE 3
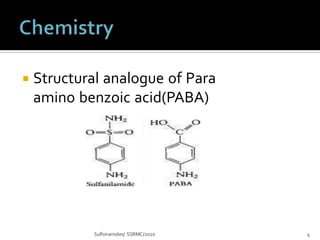
- 4. ? Structural analogue of Para amino benzoic acid(PABA) Sulfonamides/ SSRMC/2020 4
- 5. (1)Oral absorbable ¨C Three types on the basis of half life: (a) Short acting(4-8hr) ¨CSulfadiazine (b) Intermediate acting(8-12hr) - Sulfamethoxazole*,Sulfamoxole (c) Long acting (~7days) ¨C Sulfadoxine , Sulfamethopyrazine Sulfonamides/ SSRMC/2020 5
- 6. Special purposeSulfonamides (2) Oral non absorbable ¨C Sulfasalazine* Sulfonamides/ SSRMC/2020 6 (3) Topical ¨C Mafenide, Sulfacetamide, Silver sulfadiazine**
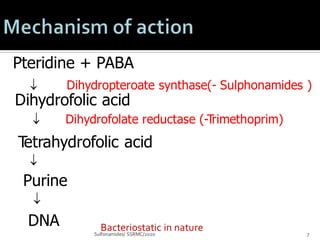
- 7. Pteridine + PABA Sulfonamides/ SSRMC/2020 7 Dihydropteroate synthase(- Sulphonamides ) Dihydrofolic acid Dihydrofolate reductase (-Trimethoprim) Tetrahydrofolic acid ? Purine ? DNA ? ? Bacteriostatic in nature
- 8. SPECTRUM Both gram positive and gram negative Bacteriostatic. Eg.s.pyogenes,s.pneumonia,H.influenza,H.ducreyi, nocardia,actinomyces. MIC(minimum inhibitory conc) range from 0.1microg/ml (C.trachomatosis ) to 4-64 micg/ml for E.coli.
- 9. PHARMACOKINETICS Abs:70-100% orally absorbed sulfonamides can be found in urine within 30 mins peak plasma levels 2-6hrs major site:SI>Stomach bound to albumin Dis:throughout all the tissues and body fluids crosses placenta and cause both antibacterial and troxic effects.
- 10. Cont.. Metabolism:Liver Acetylation metabolic derivative(N4 acetylated sulfonamide) Excretion:excreted in urine t1/2 (depends on renal function) In acid urine,the older sulfonamides are insoluble and may ppt ,forming crystalline deposits tat can cause urinary obs. Small amounts-feces,bile,milk and other secretion.
- 11. ? Toxoplasmosis ¨C Combination of sulfadiazine & Pyrimethamine is DOC . ? Urinary tract infection ¨C Due to appearance of resistant organism , no longer therapy of first choice. - Co-trimoxazole ,Fluoroquinolones are preferred drugs. ? Nocardiasis- Sulfadiazine may be given 6-8 gm daily. ? P. falciparum malaria- 3 tab stat of Sulfadoxine (500mg ) + Pyrimethamine (25mg) Sulfonamides/ SSRMC/2020 1
- 12. ? To prevent burn infection ¨C Silver sulfadiazine 1% cream ? In Ulcerative colitis ¨C Sulfasalazine in dose of 3-4 gm /day induces remission for few weeks. Maintance therapy 1.5-2 gm is required. ? Trachoma- Sulfacetamide Sod. as eye drops & eye ointment. Systemic therapy with tetracycline is preferred. ? Preventing of Streptococcal infection & recurrence of Rheumatic fever- Used in who are sensitive to Penicillin.Sulfonamides/ SSRMC/2020 1
- 13. ? 1.Nausea , vomiting , epigastric pain ? 2.Crystalluria is dose related ? Advice- Alkalization of urine increases pH?solubility of sulfonamide increased. ? Plenty of fluid ¨C daily urine volume in adult at least 1200 ml. ? 3. Hypersensitivity reactions ? Rashes , urticaria,& drug fever Sulfonamides/ SSRMC/2020 10
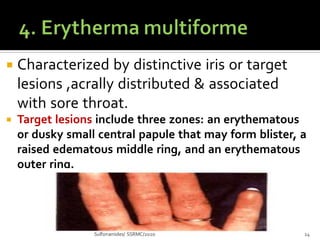
- 14. ? Characterized by distinctive iris or target lesions ,acrally distributed & associated with sore throat. ? Target lesions include three zones: an erythematous or dusky small central papule that may form blister, a raised edematous middle ring, and an erythematous outer ring. Sulfonamides/ SSRMC/2020 14
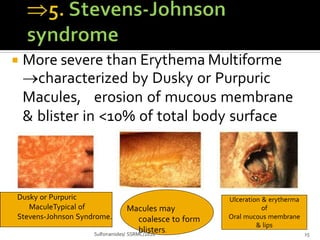
- 15. ? More severe than Erythema Multiforme ?characterized by Dusky or Purpuric Macules, erosion of mucous membrane & blister in <10% of total body surface area Dusky or Purpuric MaculeTypical of Stevens-Johnson Syndrome. Macules may coalesce to form blisters. Sulfonamides/ SSRMC/2020 15 Ulceration & erytherma of Oral mucous membrane & lips
- 16. Or Lyells syndrome > 30 % of body surface area. ?7. Hemolysis in dose dependent in G- 6-PD deficiency patients. 8.Kernicterus may precipitate in premature neonate , by displacement of bilirubin from plasma protein binding site. ?9. Hepatitis Sulfonamides/ SSRMC/2020 16
- 17. DRUG INTERACTION: Oral anticoagulants, sulfonylureas,hypoglycaemic agents and hydantoin anticonvulsants In each case sulfonamides can potentiate the effects of each other drug.
- 18. ? The resistant mutants either: -Produced increase amount of PABA. -Dihydropteroate synthase enzyme has low affinity for sulfonamide. Sulfonamides/ SSRMC/2020 18
- 19. ? Combination of sulfamethoxazole(400mg) with Trimethoprim (80 mg) ¨C 5:1 Ratio ?Combination preferred due to ? MOA- Individual compounds are bacteriostatic - combination become bactericidal due to sequential blockade of folate metabolism. - STUDENTS +TEACHER 15
- 20. ? To achieve optimum synergism -absorption &Excretion characteristics are similar -Half life sulfamethaoxazole ¨C 10 hrs Trimethoprim ¨C 11 hrs -Trimethoprim more widely distributed in tissue than sulfamethaoxazole ? To reduce bacterial resistance. Sulfonamides/ SSRMC/2020 20
- 21. ? Trimethoprim 80 mg Sulfonamides/ SSRMC/2020 21 + 0ral or Inj/5ml ? Sulfamethoxazole 400 mg = Co-trimoxazole ? Dose ¨C 2 tab or double strength (DS) of single tab given twice daily for 10 ¨C14 days for management of most infection
- 22. ? Megaloblastic anemia occur in patient with marginal folate level ? Hemolytic anemia may develop individual with G6PD deficiency ? Stevens ¨CJohnson syndrome & Lyell¡¯s syndrome can occur. Sulfonamides/ SSRMC/2020 22
- 23. ? Nausea, vomiting, stomatitis, headache, rashes ? Patient with renal disease may develop uremia ? Fever, bone marrow hypoplasia in AIDS patients with Pneumocystis jiroveci ? Diuretics along with cotrimoxazole- thrombocytopenia Sulfonamides/ SSRMC/2020 23
- 24. ? Urinary tract infection (UTI) ?single dose of 4 tab of Co ¨C trimoxazole Sulfonamides/ SSRMC/2020 20 T/t for acute cystitis or Uncomplicated UTI ? Prostatitis has good value - 4-6 weeks T/t ? Bacterial respiratory tract infection ? Effective in acute otitis media in children & acute maxillary sinusitis caused by H. influenza ? Streptococcal pharyngitis¨C does not eradicatestreptococcus
- 25. ? Typhoid fever ¨C Now DOC Ciprofloxacin/ Cephalosporins ?Used as alternative in patients not tolerating Fluroquinolones ?Bacterial diarrhoea & dysentry Fluoroquinolone is better drugs ?Chancroid ¨C Co-trimoxazole 2 tabs BD for 5-7 days is DOC. ?Pneumocystis joroveci- severe pneumoniaSulfonamides/ SSRMC/2020 21
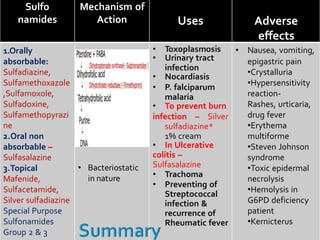
- 26. Sulfonamides/ SSRMC/2020 Sulfo namides Mechanism of Action Uses Adverse effects 1.Orally absorbable: Sulfadiazine, Sulfamethoxazole ,Sulfamoxole, Sulfadoxine, Sulfamethopyrazi ne 2.Oral non absorbable ¨C Sulfasalazine 3.Topical Mafenide, Sulfacetamide, Silver sulfadiazine Special Purpose Sulfonamides Group 2 & 3 ? Bacteriostatic in nature ? Toxoplasmosis ? Urinary tract infection ? Nocardiasis ? P. falciparum malaria ? To prevent burn infection ¨C Silver sulfadiazine* 1% cream ? In Ulcerative colitis ¨C Sulfasalazine ? Trachoma ? Preventing of Streptococcal infection & recurrence of Rheumatic fever ? Nausea, vomiting, epigastric pain ?Crystalluria ?Hypersensitivity reaction- Rashes, urticaria, drug fever ?Erythema multiforme ?Steven Johnson syndrome ?Toxic epidermal necrolysis ?Hemolysis in G6PD deficiency patient ?Kernicterus
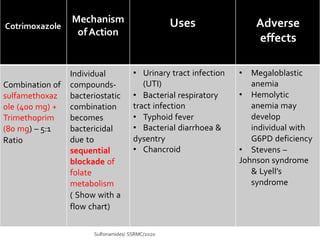
- 27. Cotrimoxazole Sulfonamides/ SSRMC/2020 Mechanism ofAction Uses Adverse effects Combination of sulfamethoxaz ole (400 mg) + Trimethoprim (80 mg) ¨C 5:1 Ratio Individual compounds- bacteriostatic combination becomes bactericidal due to sequential blockade of folate metabolism ( Show with a flow chart) ? Urinary tract infection (UTI) ? Bacterial respiratory tract infection ? Typhoid fever ? Bacterial diarrhoea & dysentry ? Chancroid ? Megaloblastic anemia ? Hemolytic anemia may develop individual with G6PD deficiency ? Stevens ¨C Johnson syndrome & Lyell¡¯s syndrome