Topical corticosteroids
Download as PPTX, PDF1 like502 views

A lecture by Dr. Naya Talal Hassan (Master Degree in Dermatology and STIs) about topical corticosteroids (TCS), that are used very commonly in dermatology. It contains important information which every dermatologist should know.





















































More Related Content
What's hot (20)
Similar to Topical corticosteroids (20)


















Recently uploaded (20)




















Topical corticosteroids
- 1. Topical Corticosteroids By: Dr.Naya Talal Hassan Dermatology Department, Tishreen University Latakia, Syria
- 3. •Corticosteroids (adrenal cortical steroids) arenaturalhormones made by the adrenal cortex. •Cholesterol is the sole precursor of steroids. •Theycan beproducedthrough industry. •Industrial steroids arestronger than the naturallyoccurring hormone. What are Corticosteroids?
- 5. The efficiency ofcorticosteroids to treat wide range of inflammatory conditionsincluding rheumatoidarthritis and asthma marked the birth of a wonder drug
- 6. A topicalcorticosteroidis appliedto aparticularplacethe body(mainly thebodysurfacessuchas theskin ormucous membranes). A topicalsteroidis ananti-inflammatorypreparationusedtocontroleczema andmanyotherskinconditions. Topicalsteroidsareavailablein creams,ointments,solutionsandothervehicles. Topicalsteroidsarealso calledtopicalcorticosteroids,glucocorticosteroids,andcortisone. What is a topicalcorticosteroid?
- 7. How does atopical steroid work? The effects of topical steroid on various cells in the skin are: Anti-inflammatory Immunosuppressive Anti-proliferative Vasoconstrictive.
- 10. The potency of topical steroid The potency of a topical steroid depends on: The specificmolecule The amount thatreaches the target cell Absorption through the skin Formulation “Potency is also increased when a formulation is used under occlusive dressing or in intertriginous areas”
- 12. 01 Very potent or superpotent Clobetasolpropionate Betamethasonedipropionate(in anoptimisedvehicle) (up to600 times as potent as hydrocortisone) Hydrocortisone Hydrocortisoneacetate 04 Mild Clobetasonebutyrate Triamcinoloneacetonide (2–25 times as potent as hydrocortisone) 03 Moderate Betamethasonevalerate Betamethasonedipropionate(cream, ointment,gel) Diflucortolonevalerate Hydrocortisone17-butyrate Mometasonefuroate Methylprednisoloneaceponate (100–150 times as potent as hydrocortisone) 02 Potent
- 14. As a general rule: We use theweakestpossible steroid thatwill do the job. It isoften appropriate to use a potent preparation for a short time to ensure theskin condition clears completely.
- 15. A topical steroid is absorbed in different rates depending on skinthickness. The greatest absorption occurs through the thin skinof eyelids, genitals, and skincreases when a potent topical steroid should be avoided. The leastabsorption occurs through the thick skin of palms and soles, where a mild topical steroid is ineffective. Absorption also depends on the vehicle in which the topical steroid is delivered and is greatly enhanced by occlusion.
- 16. Formulations of topical steroid Several formulationsare availablefortopicalsteroids,intendedtosuitthetypeofskinlesionandits location. Creams andlotions:are themostpopularformulations. Ointment: • The most suitable formulation for dry, non-hairy skin • No requirement for preservative, reducing risk of irritancy and contact allergy • Occlusive, increasing risk of folliculitis and miliaria Gelorsolution: • Useful in hair-bearing skin • Has an astringent (drying) effect • Stings inflamed skin
- 17. Combination products • Topical steroid is sometimes combined with another active ingredient, including antibacterial, antifungalagent or calcipotriol. • Topical corticosteroid/antibiotic preparations should be used rarely, and short-term (eg, three times daily for one week for a small area of infected dermatitis), to reduce the risk of antimicrobial resistance.
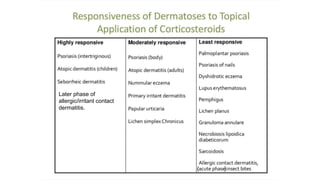
- 20. Later phase of allergic/irritant contact dermatitis. ( )
- 21. What are the sideeffects oftopical steroid? • Side effects are uncommon or rare when topical steroids are used appropriately under medical supervision. • Topicalsteroid may be falselyblamed for a sign when underlying disease or another condition is responsible (for example, postinflammatory hypopigmentation or undertreated atopic eczema).
- 22. Cushing syndrome Internal side effects similar to those due to systemic steroid (Cushing syndrome) are rarely reportedfrom topical steroids, and only after long-term use of large quantities of topical steroid (eg > 50 g of clobetasol propionate or > 500 g of hydrocortisone per week). Cases of Cushing syndrome due to topical corticosteroids most often occur because of inappropriate prescribing or over the counter salesof corticosteroids in countries where that is permitted.
- 23. Cutaneous side effects Skin thinning(atrophy) Stretch marks(striae) in armpits or groin Easy bruising (senile/solar purpura)and tearing of the skin Enlarged blood vessels (telangiectasia) Localised increased hair thickness and length (hypertrichosis) Hypo/hyperpigmentation A ggravate or mask skin infections such as impetigo, tinea, herpes simplex ,malassezia folliculitis and molluscum contagiosum. Periorificial dermatitis (commonwith potent steroids); this can occurin children Steroid rosacea Symptoms dueto topical corticosteroid withdrawal (Psoriasis). Stinging frequentlyoccurs when a topical steroid is first applied, due to underlying inflammation and brokenskin. Contact allergy to steroid molecule, preservative or vehicle is uncommonbut may occurafter the first application of the product or after manyyears of its use.
- 24. Local side effects may arise when a potent topical steroid is applied dailyfor long periods oftime (months). Mostreports of side effects describe prolonged use of an unnecessarily potent topical steroid forinappropriateindications.
- 25. Ocularside effects: Atopical steroid should beused cautiously on eyelid skin, where it commonlyresults in periocular dermatitis. Potentially, excessive use overweeks to months might lead to glaucoma or cataracts. Topical steroid in pregnancy: Mild and moderate-potency topical steroids can be safely used in pregnancy. Caution should be used for potent and ultrapotent topical steroids used over largeareas or under occlusion, of which a proportion will beabsorbed systemically. Reports of low birth-weight infants exposed to high-dose topical steroid are not thought to be due to the medication.
- 26. Topical corticosteroid (TCS) phobia It refers to the negative feelings and beliefs related to TCSsexperienced by patients and patients' caregivers. This phenomenonmaybe a major contributing factor in treatment failure in patients with atopic dermatitis, yetit has been sparsely described in the literature.
- 27. How to use a topical steroid? • Topical steroid is applied usuallyonce daily (usuallyat night) to inflamed skinfor a course of 5 days to several weeks. After that, it isusuallystopped, or the strength or frequency of application is reduced. • Emollients can be applied before or after the application of topical steroid, to relieve irritation and dryness or as a barrier preparation. Infection may need additional treatment.
- 30. T H A N K Y O U