
































![Resources
? Adigun R, Singh R. Tuberculosis. [Updated 2023 May 14]. In: StatPearls
[Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK441916/
? Das S, Das D, Bhuyan UT, Saikia N. Head and Neck Tuberculosis:
Scenario in a Tertiary Care Hospital of North Eastern India. J Clin Diagn
Res. 2016 Jan;10(1):MC04-7. doi: 10.7860/JCDR/2016/17171.7076. Epub
2016 Jan 1. PMID: 26894099; PMCID: PMC4740627.
? Sabah Handbook on Management of Tuberculosis, 2021
? CPG Management of Tuberculosis, 4th Edition](https://image.slidesharecdn.com/tuberculosiskogicopy-240818160431-07e4df96/85/Tuberculosis-kogi-copy-pptxgfhnfgbftyrtghbcxt-38-320.jpg)










![TB [Autosaved].pptxnhgfytetrstrht65356yf](https://cdn.slidesharecdn.com/ss_thumbnails/tbautosaved-241207141258-e6d69ce6-thumbnail.jpg?width=560&fit=bounds)
![TB [Autosaved].pptx gg897dt4sr3rshtfjry8](https://cdn.slidesharecdn.com/ss_thumbnails/tbautosaved-241204074724-e0f6b93a-thumbnail.jpg?width=560&fit=bounds)


















More Related Content
Similar to Tuberculosis kogi copy.pptxgfhnfgbftyrtghbcxt (20)
More from arvind339112 (6)




Recently uploaded (20)




















Tuberculosis kogi copy.pptxgfhnfgbftyrtghbcxt
- 1. Tuberculosis Presenter: Kogilavani Mani ( Kogi )
- 2. Epidemiology In Malaysia, Sabah has recorded the highest number of TB cases followed by Selangor in the year of 2023 In the year 2023, a total 5,814 cases of tuberculosis were reported in Sabah, followed by Selangor 5,631 cases and Sarawak with 3,177 cases. The district with the highest TB cases was Kota Kinabalu with 793 cases followed by Sandakan 485 cases, Tawau 445 cases, Lahad Datu 353 cases, Semporna 334 cases and Keningau 277 cases. The other district only reported less than 200 cases per year. Source: Sabah Handbook on Management of TB
- 3. Introduction Etiology Mycobacterium tuberculosis Mode of transmission inhalation of infected aerosolized droplets. " It mainly affects the lungs, making pulmonary disease the most common presentation " " Tuberculosis can affect every organ in the body except nail, hair and teeth " Tuberculosis
- 4. Approach to patient suspected with TB
- 5. Presentation Extrapulmonary symptoms GIT:Abd. pain, diarrhoea, bloating CNS: Headache, focal neurology deficit CVS: chest pain, failure symptoms Bone/Joint: swellings, fractures, discharging sinus. Larynx: hoarseness of voice, odynophagia, dysphagia Constutional symptoms 1.Prolonged Fever ? Low grade fever 2. Night sweats 3. Loss of weight and loss of appetite Risk factors ? Any h/o close contact with PTB patients ? High risk behaviour: Subtance Abusers, h/o multiple partners ? Active smokers ? Overcrowded conditions: prison, shelters, immigrants Respiratory symptoms: ? Prolong cough ? Chest pain ? SOB ? Hemoptysis
- 6. Examination Physical examination findings associated with TB depend on the organs involved. General condition: Cachexic, lethargic looking, tachypneic Pulmonary TB Palpation: Reduced chest expansion, increased vocal fremitus Percussion: Dull Auscultation: Bronchial breath, Increased vocal resonance Signs of extrapulmonary TB Differ according to the organs involved
- 7. What is a ghon focus? A Ghon focus is a primary lesion usually subpleural, often in the mid to lower zones, caused by Mycobacterium bacilli (tuberculosis) developed in the lung of a nonimmune host (usually a child). It is named for Anton Ghon (1866¨C1936), an Austrian pathologist. Approximately three weeks after the initial infection, more specific immune cells (e.g., T cells, B cells, and Neutrophils) surround the site of TB infection, creating a wall of immune cells known as a granuloma, which isolates the bacteria and prevents it from spreading. The tissue inside the granuloma then dies during a process referred to as caseous necrosis, or cheese-like necrosis. This necrotic area is known as a Ghon focus. TB infection can also spread to nearby hilar lymph nodes, either carried through the lymph or by direct extension of the Ghon focus. Together, the caseating tissue and associated lymph node involvement make up the characteristic ˇ°Ghon complex.ˇ±
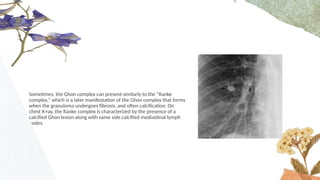
- 8. Sometimes, the Ghon complex can present similarly to the ˇ°Ranke complex,ˇ± which is a later manifestation of the Ghon complex that forms when the granuloma undergoes fibrosis, and often calcification. On chest X-ray, the Ranke complex is characterized by the presence of a calcified Ghon lesion along with same side calcified mediastinal lymph nodes.
- 9. The usual location for Ghon focus is the apical segment of right lower lobe. ?Ghon complex comprising Ghon focus and right hilar lymphadenopathy plus pleural effusion.
- 10. The combination of late fibrocalcific lesions of the lung and lymph node which evolved from the Ghon complex is referred to as the ˇ°Ranke complexˇ± Ranke Complex. There is a combination of a calcified peripheral granuloma (black arrow) and a calcified hilar lymph node (white arrow) on the same side. Several other, small calcified granulomas are seen in the right mid-lung field.
- 11. ? Parenchymal opacities ¨C heterogeneous opacities most commonly in apical and posterior segmental upper lobes and the superior segment of the lower lobes. ? Cavitation and Air-fluid levels ? Bronchogenic spread Chest X-ray of our patient at the time of admission
- 12. TypIcal features Of prImary PTB consolidation of the upper zone with ipsilateral hilar enlargement due to lymphadenopathy
- 13. GRADING OFPULMONARY TUBERCULOSIS SEVERITY BASED ON CHEST RADIOGRAPH IN ADULTS (1/3) Minimal ˇń Minimal lesions confined to a small part of one of both lungs ˇń total extent of the lesions should not exceed the volume of the lung on one side.
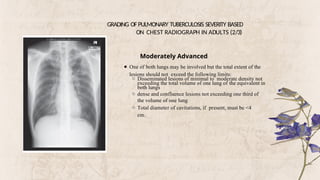
- 14. GRADING OFPULMONARY TUBERCULOSIS SEVERITY BASED ON CHEST RADIOGRAPH IN ADULTS (2/3) Moderately Advanced ˇń One of both lungs may be involved but the total extent of the lesions should not exceed the following limits: ˇđ Disseminated lesions of minimal to moderate density not exceeding the total volume of one lung of the equivalent in both lungs ˇđ dense and confluence lesions not exceeding one third of the volume of one lung ˇđ Total diameter of cavitations, if present, must be <4 cm.
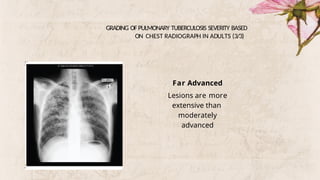
- 15. GRADING OF PULMONARY TUBERCULOSIS SEVERITY BASED ON CHEST RADIOGRAPH IN ADULTS (3/3) Far Advanced Lesions are more extensive than moderately advanced
- 16. CXR Example of patientˇŻs CXR
- 17. Sputum AFB Example of lab result Microscopic evaluation of sputum for acid- fast bacilli begins with making a smear
- 18. What if the AFB is Negative? Always ensure satisfactory specimen
- 19. MTB GeneXpert ? Able to simultaneously detect MTBC and Rifampicin resistance ? Sputum should be sent for MTB GeneXpert if smear negative PTB is suspected. ? In 2020, WHO recommended that this test be used as the first line TB screening test, however this is not feasible as yet in Sabah due to steep testing costs.
- 20. MTB GeneXpert
- 22. Investigations PTB Specific Investigations Other investigations Investigations for Extra-PTB 1. Sputum AFB - x1, x2, x3 2. Mycobacterial culture and sensitivity * Taken at initiation of TB treatment * To confirm presence of Mycobacterium Tuberculosis * To test for drug sensitivity LTAT for culture is 14 days while LTAT sensitivity is 42 days to 68 days 3. MTB GeneXpert 4. Sputum LPA ( Line Probe Assay ) - is another molecular method and relatively fast in determining Isoniazid and Rifampicin resistant - Indication: a. Persistant smear positive despite after 2month of effective regime b. Prior to MDR regime initiation (to determine mutation ) c. Newly diagnose PTB smear positive patient with positive contact with Isoniazid resistant index. 5. Imaging ¨C CXR 1.Blood Baseline ? FBC, RP, LFT,CRP,ESR TRO immunocompromised state ? Infective screening ? FBS 2. Urine - UPT ( all female childbearing ages ) 1. CNS * Contrasted CT brain * Lumbar puncture - MTB GeneXpert - AFB - MTB C&S 2. Spine * CT/MRI Spine * Tissue for HPE MTB C+S * Pus - AFB - MTB C+S - MTB GeneXpert 3. Pericardium * Echocardiography * Pericardial tapping - AFB - MTB C+S - MTB GeneXpert 4. Abdomen ( Liver, Gut, Peritoneum ) * Ultrasound Abdomen * CECT Abdomen if needed * Colonoscopy * Tissues for HPE & MTB C+S 5. Lymph node * Lymph node FNAC and/or biopsy - HPE & MTB C+S 6. Pleural * Pleural fluid ADA * MTB C+S * AFB
- 23. Treatment
- 24. Treatment for new case Six-month regimen consisting of two months of daily EHRZ* (2EHRZ) followed by four months of daily HR* (4HR) is recommended for newly-diagnosed PTB Pyridoxine 10 mg OD is also prescribed to prevent peripheral neuropathy caused by Isoniazid
- 25. Treatment for new case After measuring latest body weight, attending clinician should round ATT dosage to nearest available preparation (highest range is preferred for H & R)
- 26. Refer to Opthal Clinic for Eye Assessment Ethambutol ADR: Optic neuritis - decrease in visual acuity, red- green colour blindness, blurring and central scotoma. SnellenˇŻs Chart Ishihara
- 27. Duration of ATT will depend on severity or site of infection. All EPTB cases in Sabah should be referred to Infectious Disease (ID) team for optimum regime & duration of treatment.
- 28. Steroid ? is required for TB meningitis and TB pericarditis. ? It can improve symptom and survival
- 30. So until when do we keep the patient? By right, we can allow discharge and continue follow up in JPL, if: 1. - Patient is clinically well - Sputum smear conversion * Sputum AFB is repeated @ 2 weeks after ATT initiation * Indicating response to ATT * Reduces risk of transmission 2. * If patient has an isolated room in his/her house * Clinically well
- 31. Directly observe therapy (DOT) Every clinician managing TB should ensure all TB patient that on ATT treatment need to undergo DOT to optimised management of TB.
- 32. Follow up
- 33. Problems During Follow Up Common problems encountered in managing TB are: ? Adverse drug reaction: -Drug-induced liver injury(DILI) - Drug-induced rash(DIR) - Other common adverse drug reactions(ADR) ? Delay conversion ? Treatment interruption
- 34. Drug Induced Liver Injury ( DILI ) The most important aspect of DILI management is that the clinician should know when to stop and how to rechallenge. The most common drug causing transaminitis are as below: ? Pyrazinamide ? Isoniazid ? Rifampicin Cases should be divided into symptom and/or severity of transaminitis. Healthcare providers should be aware that the initial presentation of DILI could be as mild as: ?Abdominal pain ?Nausea ?Vomiting ?Lethargy ?Jaundice will usually increases later as severity increase.
- 35. Approach to DILI
- 36. Common Adverse Drug Reaction
- 37. THANK YOU
- 38. Resources ? Adigun R, Singh R. Tuberculosis. [Updated 2023 May 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441916/ ? Das S, Das D, Bhuyan UT, Saikia N. Head and Neck Tuberculosis: Scenario in a Tertiary Care Hospital of North Eastern India. J Clin Diagn Res. 2016 Jan;10(1):MC04-7. doi: 10.7860/JCDR/2016/17171.7076. Epub 2016 Jan 1. PMID: 26894099; PMCID: PMC4740627. ? Sabah Handbook on Management of Tuberculosis, 2021 ? CPG Management of Tuberculosis, 4th Edition
Editor's Notes
- #1: Good afternoon, to my respected specialists and fellow friends. My name is kogi. Today, ill be presenting on TB
- #2: I will start off with the epidemiology of TB, Did you know that, Sabah has the highest recorded cases of TB in 2023 - a total of more than 4 thousand cases were reported in Sabah The highest district being KK followed by Sandakan then Tawau. Can anyone guess why the distribution is like this Kenapa KK banyak, lepas tu Sandakan lepas tu Tawau because according to population, KK has a lot of people so by right KK has the most number of cases and d/t the number of health facilities available ¨C hence higher detection right
- #3: So a small introduction to TB - TB is caused by a very stubborn pathogen known as mycobacterium tuberculosis and its mode of transmission is - inhalation of infected aerosolized droplets - so when that person sneezes or cough then aerosolized droplets stays in the air, then another person comes and breaths it in ¨C they can get TB - mycobacterium tuberculosis usually affects the lungs, and every organ in the body such a bones,joints, Genito-urinary, intestines,skin, tb meningitis
- #4: So how do we approach a patient suspected with TB so first and foremost, we would suspect TB in a patient according to their signs and symptoms so basically ¨C based on h/o and examination
- #5: So how do we approach a patient suspected with TB so first and foremost, we would suspect TB in a patient according to their signs and symptoms so basically ¨C based on h/o and examination - the most common symptoms of tb A cough that lasts more than 2 weeks Cough with sputum which is occasionally bloodstained GIT- gastro intestinal tract CNS ¨C central nervous system CVS- cardiovascular systems
- #17: PLHIV- PEOPLE LIVING WITH HIV
- #19: MTBC- MYCOBACTERIUM TUBERCULOSIS COMPLEX
- #23: New patients have never been treated for TB or have taken anti-TB drugs for less than 1 month
- #26: CENTRAL SCOTOMA- blind spots is in the middle of the vision
- #27: Duration of ATT will depend on severity of site of infection