Pgtd
Download as pptx, pdf1 like316 views

This document presents the case of a 30-year-old woman with a known history of invasive mole who is undergoing chemotherapy. She has a history of irregular bleeding and multiple D&Cs. Her most recent beta-HCG levels indicated a significant drop in tumor marker levels in response to six cycles of chemotherapy. Her physical examination was normal and laboratory results were stable. She will continue chemotherapy on an outpatient basis to further treat her invasive mole.
1 of 28
Download to read offline
![’āÆ Then she attended GOPD at rangamati general hospital on 14.09.16 [0ne month after
evacuation] this time she was attended by a senior Gynae consultant and was advised
to do a s.╬▓ HCG from chittagong city [ done from chevron ; 61000 m IU/l ,5.09.16 ] .
With this report she was referred to CMCH for further management .
’āÆ But she got admitted in a private hospital & received two unit of blood trasnsfusion ,
had some investigation s: [s.╬▓ HCG-8800.30 m IU /L ,11.09.16] referred to CMCH
for further Rx.
’āÆ she went to AD ŌĆōDin Hospital Dhaka ,
’āÆ Diagnosed as a case of incomplete abortion
’āÆ D & C done on ( 19.09.16 )[ 2nd time ]
’āÆ investigations done at AD Din hospital :
’é¦ s.╬▓ HCG 1782 m IU /L ( 21.09.16)
’é¦ CBC :
’é¦ HB%- 9.6 g/dl
’é¦ ESR- 40 mm in 1st hr
’é¦ WBC :
’é¦ TC-8.63X10^3/ uL
’é¦ Platelet -405x10^3/ uL
’é¦ Histopatology report : suggestive of product of conception .](https://image.slidesharecdn.com/pgtd-170924132530/85/Pgtd-5-320.jpg)

Ad
Recommended
Hong Kong - Current Situation in Control Strategies and Health Systems in Asia
Hong Kong - Current Situation in Control Strategies and Health Systems in AsiaThalassaemia International Federation
╠²
The document details the current state of thalassaemia management in Hong Kong, including demographics, healthcare infrastructure, and epidemiology. It highlights the public healthcare system, the availability of treatments like blood transfusions and iron chelation, and the challenges of prenatal diagnosis. The future plans involve transitioning patients from pediatric to adult care and establishing dedicated centers for thalassaemia treatment.Perinatal mort
Perinatal mortLily Tensai
╠²
This document summarizes the prenatal care and delivery of a 32-year-old woman, NFMZ, on her fourth pregnancy. She was diagnosed with late-onset preeclampsia and had two hospital admissions for elevated blood pressure. At 32 weeks gestation, she experienced severe back pain and vaginal bleeding and was transported to the hospital where an ultrasound showed no fetal heartbeat. She delivered a stillborn baby girl weighing 1.7 kg and was discharged after one week, with instructions to monitor her blood pressure postpartum.Caso clinico. apendicitis y lma
Caso clinico. apendicitis y lmaMaira Casta├▒o
╠²
A 59-year-old woman presented with acute appendicitis and was found to have acute myeloid leukemia (AML) based on peripheral smear, bone marrow biopsy, and surgical pathology of the appendix showing AML infiltration. This case describes the rare occurrence of AML initially presenting as acute appendicitis. While the patient underwent an appendectomy for the appendicitis, treatment and management of the AML, including chemotherapy, was critical for remission and survival. Though appendicitis in leukemia carries a high mortality, this patient survived 185 days after diagnosis, longer than most similar cases reported, highlighting the importance of a broad differential diagnosis and prompt treatment.Intimm Meeting Abstracts
Intimm Meeting AbstractsUniversidad Central de Venezuela
╠²
This document summarizes a study examining the role of HLA variability in tuberculosis. The study analyzed the HLA-DRB1 and HLA-DQB1 genes in 93 tuberculosis patients and 101 healthy controls in Venezuela. The frequencies of DRB1*12 and DQB1*0602 were significantly higher in patients, while DRB1*03 and DQB1*0306 were higher in controls. Certain HLA-DQB1 allele combinations encoding or not encoding aspartate at position 57 in the beta chain were only found in patients. The DRB1*13-DQB1*06 haplotype was also more common in controls than patients. The results suggest HLA polymorphisms influence the occurrence of tuberculosis in these patients.Case pr .tayseir
Case pr .tayseirFAARRAG
╠²
A 36-year-old female presented with abdominal pain, lower limb swelling, and elevated renal function tests one month after an abortion. She was initially admitted to another hospital where she became oliguric and developed leg edema. She received hemodialysis with no improvement and was referred for a renal biopsy. On examination at the new hospital, she had mild leg edema and ascites. Imaging showed enlarged kidneys with increased echogenicity. She received plasma exchange sessions and conservative treatment. Her renal function and fluid balance improved with treatment.Hospital Dentistry
Hospital DentistryJoseph Russell Nagal Gorda
╠²
This document contains medical records for a patient admitted for cauterization of genital warts. It includes admission orders, vital sign records, laboratory and ultrasound results, physician notes, and medication orders. The patient was admitted under Dr. Maglaya/Acuna/Sumpang/Villamor and consent was secured for cauterization. Laboratory tests showed anemia. The patient underwent cauterization and was discharged with oral medications including antibiotics and pain relievers.Hellp with di
Hellp with diManjushree Boob
╠²
This document presents a case study of a 24-year-old woman, pregnant with twins, who came to the hospital at 34 weeks gestation with high blood pressure and other symptoms of Preeclampsia with Severe Features (HELLP Syndrome). Tests confirmed HELLP Syndrome and Diabetes Insipidus. She underwent an emergency C-section under spinal anesthesia and delivered two healthy babies. Post-operatively she had excessive urine output consistent with Diabetes Insipidus, which was successfully treated with nasal vasopressin spray. She recovered well and was discharged on post-operative day 8.Senior Medillectuals Mains
Senior Medillectuals MainsQuaesitum MAMC Quiz Club
╠²
Based on the information provided, the next best step would be to start growth hormone replacement therapy to treat her isolated growth hormone deficiency.Temesgen kusse gyn case
Temesgen kusse gyn caseTemesgen Kusse
╠²
AR, a 25-year old pregnant woman, was admitted to the hospital with shortness of breath, cough with blood-tinged sputum, and vaginal bleeding. She was diagnosed with placenta previa and severe pulmonary hypertension due to rheumatic heart disease. During her hospital stay, she received furosemide and iron supplements to manage her symptoms and improve her hemoglobin levels. Her condition stabilized with treatment and monitoring of her vital signs, lab work, and echocardiograms. The goals of care were to improve her symptoms, prevent further bleeding, and delay delivery to avoid preterm birth.Case on sepsis (shahnawaz)
Case on sepsis (shahnawaz)Shahnawaz Ahmad Teli
╠²
This document presents the case of a 74-year-old female patient admitted to the hospital for sepsis. She had a history of asthma, hypertension, obesity, and depression. Upon admission, she was in septic shock with respiratory and renal failure. Laboratory tests showed elevated white blood cell count and abnormal liver and kidney function. She was started on antibiotics, vasopressors, and other medications to treat her infection and stabilize her vital signs. Her treatment in the hospital was successful and she was discharged with medications to continue at home.Case on osteomyelitis (shahnawaz)
Case on osteomyelitis (shahnawaz)Shahnawaz Ahmad Teli
╠²
This document presents a case study of an 18-year-old male patient admitted with pain and swelling in his left thigh for 3 months along with pus discharge for 1 month. He was diagnosed with osteomyelitis based on laboratory tests, blood cultures, and imaging showing bone marrow abnormalities. He underwent two surgeries to drain pus and was treated with antibiotics including ampicillin, cloxacillin, cefuroxime, ofloxacin and amikacin. He was also started on anti-tubercular treatment as his blood cultures grew M.tuberculosis. He showed improvement and was discharged on a course of ofloxacin, omeprazole and diclofenac+Participants workbook
Participants workbookDavid Ngogoyo
╠²
This document provides instructions and case studies for trainees to practice completing comprehensive care clinic patient cards. The case studies describe two patients' visits to care clinics, including their medical history, test results, treatment, and progress. Trainees are asked to use the information from the case studies to fill out blank patient cards. They may find that some information is missing or extra from what is needed on the cards. The goal is to practice accurately documenting patient information for reporting and monitoring purposes.Facilitators workbook
Facilitators workbookDavid Ngogoyo
╠²
1. Use the pre-ART and ART registers to fill out measures on the monthly summary sheet, including the number of new patients enrolled in HIV care, cumulative patients ever enrolled, patients eligible but not started on ART, and patients started on ART or PEP this month.
2. The number of patients eligible but not started on ART is found by counting those in the pre-ART register with an eligibility date but no ART start date.
3. The number currently on ARVs is found by counting patients in the ART register with an ARV regimen listed for the terminal month.
4.Case on emphysema....shahnawaz
Case on emphysema....shahnawazShahnawaz Ahmad Teli
╠²
A 5-year-old male patient presented with fever, chest pain, and breathlessness for 30 days. Physical examination and investigations revealed emphysema. The patient underwent surgery to remove damaged lung tissue and drain pleural fluid. He was treated with antibiotics, supplements, and bronchodilators. After improving, the patient was discharged with medications including Linezolid and advised to exercise regularly and avoid triggers to manage his emphysema.Hemoglobin H Disease
Hemoglobin H DiseaseAlana Saldana
╠²
A 16-year-old Cambodian boy presented with fever, abdominal pain, nausea, vomiting, headache, and sore throat for several days. Initial workup found anemia, jaundice, splenomegaly, and hepatitis B infection. Additional testing revealed ╬▒-thalassemia (-/-╬▒) consistent with Hb H disease. A stool culture was positive for Yersinia enterocolitica. The patient was diagnosed with Hb H disease with Yersinia enterocolitis and hepatitis B. He received supportive care including blood transfusions and gradually improved.CML HITORICAL PERISPECTIVE
CML HITORICAL PERISPECTIVEmanal bessa
╠²
This document provides a historical perspective on chronic myeloid leukemia (CML), summarizing key developments from its early descriptions in the 19th century to modern targeted therapies. Some of the major advances discussed include the discovery of the Philadelphia chromosome in 1960 linking CML to a chromosomal abnormality, identification of the BCR-ABL fusion gene in 1973, development of allogeneic stem cell transplantation as a curative treatment in the 1970s, introduction of interferon-alpha and tyrosine kinase inhibitors like imatinib in the 1990s-2000s, and ongoing research into second- and third-generation tyrosine kinase inhibitors. The CML story illustrates significant progress in understanding and treating the disease through scientific insights and innovationscase on Meningeal tuberculosis (shahnawaz)
case on Meningeal tuberculosis (shahnawaz)Shahnawaz Ahmad Teli
╠²
A 18-year old female patient presented with chronic headache, vomiting and fever for 15 days. Investigation revealed frontotemporal edema on CT scan and significant perilesional edema on MRI. She was diagnosed with meningeal tuberculosis and treated with anti-tubercular drugs along with corticosteroids and mannitol. Her symptoms improved and she was discharged on medications including rifampicin, isoniazid, ethambutol and pyrazinamide to complete the full course of treatment over several months and ensure adherence to prevent relapse or drug resistance.Senior Medillectuals Prelims
Senior Medillectuals Prelims Quaesitum MAMC Quiz Club
╠²
The document contains questions related to various medical topics. It includes 23 multiple choice and matching questions testing knowledge on subjects like pulmonary hypertension, drug exposure in pregnancy, ECG patterns, GCS scoring, radiology, pediatric growth parameters, inborn errors of metabolism, diabetes insipidus, SLE criteria, ARDS management, reproductive endocrinology, biochemical tests, infectious diseases, arrhythmias, neurology, and procedures.A case presentation on Molar pregnancy
A case presentation on Molar pregnancyDr. Tanvir
╠²
This case presentation describes a 24-year-old woman who presented with complaints of amenorrhea for 21+ weeks, per vaginal bleeding for two days, and passage of grape-like substances for one day. Her medical history and examination findings were presented. Initial diagnosis of a molar pregnancy was made based on her history and ultrasound findings. She underwent suction and evacuation surgery, which confirmed the diagnosis of a molar pregnancy based on histopathology. She was discharged with advice for follow up, contraception, and monitoring of beta hCG levels. The case discussion then provides an overview of gestational trophoblastic diseases including classification, etiology, pathogenesis, clinical features and management of hydatidiform mole.Case Presentation Rh negative pregnancy.pptx
Case Presentation Rh negative pregnancy.pptx25charunethrasriniva
╠²
The document presents a case study of a 25-year-old pregnant woman, Mrs. Sudha, who is Rh-negative and currently 37 weeks and 6 days into her pregnancy. She has undergone all necessary immunizations and investigations, with no significant medical complications, and is carrying a single live fetus in a longitudinal cephalic position. The treatment plan includes administration of anti-D immunoglobulin and routine evaluations leading up to delivery at 40 weeks.35 yr old pregnant lady with painless per vaginal bleeding
35 yr old pregnant lady with painless per vaginal bleedingMohammed Shadman Shakib
╠²
A 35-year-old pregnant woman, Mrs. Maleka, presented with painless vaginal bleeding at 34 weeks of gestation and generalized weakness. Her obstetric history includes one normal vaginal delivery and one cesarean due to placenta previa. Provisional diagnosis is antepartum hemorrhage due to placenta previa with breech presentation, and she is currently managed with expectant care and close monitoring until a scheduled cesarean section at 37 weeks.OBS AND GYNAE APH case presentation
OBS AND GYNAE APH case presentationSohailislam12
╠²
This document presents a case study of a 22-year-old pregnant woman, Rupa Serung, who is 38 weeks pregnant and was admitted to the hospital with bleeding per vagina. On examination, she was found to have a grade II placenta previa. Tests showed signs of anemia. An ultrasound confirmed a single fetus in longitudinal lie and cephalic presentation with a low-lying placenta. The diagnosis was grade II placenta previa. The options for management include either expectant management with bed rest or immediate termination of the pregnancy depending on the status of the mother and fetus.Case report Obstetric and Gynecological (obgyn)
Case report Obstetric and Gynecological (obgyn)osamah alfentokh
╠²
The case report details a 46-year-old Saudi housewife presenting with persistent vaginal bleeding post-menopause. Following a medical history review and physical examination, she was diagnosed with endometrial cancer and scheduled for a total abdominal hysterectomy along with a bilateral salpingo-oophorectomy. Pre-operative evaluations by cardiology and anesthesia were also planned to ensure patient safety.Placenta Accreta Spectrum.pptx
Placenta Accreta Spectrum.pptxFawad Mueen Arbi
╠²
This patient presented with retained placenta after a vaginal delivery. Her ultrasound and MRI showed placenta increta, where placental villi had invaded into the myometrium. She was initially managed conservatively with methotrexate injection, which led to a partial reduction in her beta-hCG levels. However, she later developed heavy bleeding and required an emergency hysterectomy. Placenta accreta spectrum (PAS) describes abnormal placental invasion that can cause life-threatening bleeding. Risk factors include prior uterine surgery. Management challenges include delayed referrals, lack of blood product availability, and counseling patients on prolonged hospitalization sometimes required.Intrauterine fetal demise
Intrauterine fetal demiseAnuradha Sawant
╠²
This document summarizes the case of a 36-week pregnant primigravida woman who presented with absent fetal movements for 2 days and was diagnosed with intrauterine fetal demise. Her antenatal period was otherwise uneventful. Evaluation of the stillborn fetus, placenta, and maternal factors found no anomalies or risks except for acute chorioamnionitis seen on placental histopathology. A thorough evaluation was conducted including autopsy, cultures, and genetic testing to investigate the cause, though it remained undetermined.Case Presentation of Placenta Accreta.pptx
Case Presentation of Placenta Accreta.pptxHeartMind1
╠²
The document presents the clinical profile of a 30-year-old female patient with a history of two previous cesarean sections, now presenting with a third pregnancy at 38 weeks gestation. The diagnosis includes placenta accreta, and the patient undergoes an elective cesarean section with a planned hysterectomy due to significant blood loss during surgery. Postoperative management involves monitoring in the ICU, highlighting the risks associated with this condition.CHORIOCARCINOMA case & presntn-Dr.Mohammad.ashraful amin
CHORIOCARCINOMA case & presntn-Dr.Mohammad.ashraful aminMohammad Asif
╠²
This document presents a case study of a 27-year-old female patient named Shila Rani who presented with symptoms of amenorrhea for 6 weeks, vomiting for 12 days, chest tightness for 12 days, and fever and weakness for 12 days. On examination, she appeared ill with respiratory distress. Tests revealed mild anemia, elevated white blood cell count and beta-HCG levels, suggestive of an ectopic pregnancy in the left ovary with metastasis to the lungs. She was diagnosed with choriocarcinoma and referred to an oncologist for chemotherapy with methotrexate.forcep delivery copy.pdf
forcep delivery copy.pdfJitenLad2
╠²
This case presentation summarizes the forceps delivery of a primigravida woman. The 26-year-old woman, at 38 weeks gestation, was admitted with abdominal pain and found to be in latent labor. After progressing to full dilation, she was unable to bear down effectively. An outlet forceps delivery was performed under local anesthesia due to maternal exhaustion. A baby girl was delivered in good condition, and the placenta was removed manually with an intact membrane. Both mother and baby recovered well.Labor Room Stats.pptx
Labor Room Stats.pptxrobinson405376
╠²
The patient presented at 28 weeks gestation with abdominal pain and vomiting. Her obstetric history included one full term normal delivery. On examination, she had tachycardia and hypotension. An ultrasound at the referring hospital showed an intrauterine fetal demise. She was referred for further management.More Related Content
What's hot (10)
Temesgen kusse gyn case
Temesgen kusse gyn caseTemesgen Kusse
╠²
AR, a 25-year old pregnant woman, was admitted to the hospital with shortness of breath, cough with blood-tinged sputum, and vaginal bleeding. She was diagnosed with placenta previa and severe pulmonary hypertension due to rheumatic heart disease. During her hospital stay, she received furosemide and iron supplements to manage her symptoms and improve her hemoglobin levels. Her condition stabilized with treatment and monitoring of her vital signs, lab work, and echocardiograms. The goals of care were to improve her symptoms, prevent further bleeding, and delay delivery to avoid preterm birth.Case on sepsis (shahnawaz)
Case on sepsis (shahnawaz)Shahnawaz Ahmad Teli
╠²
This document presents the case of a 74-year-old female patient admitted to the hospital for sepsis. She had a history of asthma, hypertension, obesity, and depression. Upon admission, she was in septic shock with respiratory and renal failure. Laboratory tests showed elevated white blood cell count and abnormal liver and kidney function. She was started on antibiotics, vasopressors, and other medications to treat her infection and stabilize her vital signs. Her treatment in the hospital was successful and she was discharged with medications to continue at home.Case on osteomyelitis (shahnawaz)
Case on osteomyelitis (shahnawaz)Shahnawaz Ahmad Teli
╠²
This document presents a case study of an 18-year-old male patient admitted with pain and swelling in his left thigh for 3 months along with pus discharge for 1 month. He was diagnosed with osteomyelitis based on laboratory tests, blood cultures, and imaging showing bone marrow abnormalities. He underwent two surgeries to drain pus and was treated with antibiotics including ampicillin, cloxacillin, cefuroxime, ofloxacin and amikacin. He was also started on anti-tubercular treatment as his blood cultures grew M.tuberculosis. He showed improvement and was discharged on a course of ofloxacin, omeprazole and diclofenac+Participants workbook
Participants workbookDavid Ngogoyo
╠²
This document provides instructions and case studies for trainees to practice completing comprehensive care clinic patient cards. The case studies describe two patients' visits to care clinics, including their medical history, test results, treatment, and progress. Trainees are asked to use the information from the case studies to fill out blank patient cards. They may find that some information is missing or extra from what is needed on the cards. The goal is to practice accurately documenting patient information for reporting and monitoring purposes.Facilitators workbook
Facilitators workbookDavid Ngogoyo
╠²
1. Use the pre-ART and ART registers to fill out measures on the monthly summary sheet, including the number of new patients enrolled in HIV care, cumulative patients ever enrolled, patients eligible but not started on ART, and patients started on ART or PEP this month.
2. The number of patients eligible but not started on ART is found by counting those in the pre-ART register with an eligibility date but no ART start date.
3. The number currently on ARVs is found by counting patients in the ART register with an ARV regimen listed for the terminal month.
4.Case on emphysema....shahnawaz
Case on emphysema....shahnawazShahnawaz Ahmad Teli
╠²
A 5-year-old male patient presented with fever, chest pain, and breathlessness for 30 days. Physical examination and investigations revealed emphysema. The patient underwent surgery to remove damaged lung tissue and drain pleural fluid. He was treated with antibiotics, supplements, and bronchodilators. After improving, the patient was discharged with medications including Linezolid and advised to exercise regularly and avoid triggers to manage his emphysema.Hemoglobin H Disease
Hemoglobin H DiseaseAlana Saldana
╠²
A 16-year-old Cambodian boy presented with fever, abdominal pain, nausea, vomiting, headache, and sore throat for several days. Initial workup found anemia, jaundice, splenomegaly, and hepatitis B infection. Additional testing revealed ╬▒-thalassemia (-/-╬▒) consistent with Hb H disease. A stool culture was positive for Yersinia enterocolitica. The patient was diagnosed with Hb H disease with Yersinia enterocolitis and hepatitis B. He received supportive care including blood transfusions and gradually improved.CML HITORICAL PERISPECTIVE
CML HITORICAL PERISPECTIVEmanal bessa
╠²
This document provides a historical perspective on chronic myeloid leukemia (CML), summarizing key developments from its early descriptions in the 19th century to modern targeted therapies. Some of the major advances discussed include the discovery of the Philadelphia chromosome in 1960 linking CML to a chromosomal abnormality, identification of the BCR-ABL fusion gene in 1973, development of allogeneic stem cell transplantation as a curative treatment in the 1970s, introduction of interferon-alpha and tyrosine kinase inhibitors like imatinib in the 1990s-2000s, and ongoing research into second- and third-generation tyrosine kinase inhibitors. The CML story illustrates significant progress in understanding and treating the disease through scientific insights and innovationscase on Meningeal tuberculosis (shahnawaz)
case on Meningeal tuberculosis (shahnawaz)Shahnawaz Ahmad Teli
╠²
A 18-year old female patient presented with chronic headache, vomiting and fever for 15 days. Investigation revealed frontotemporal edema on CT scan and significant perilesional edema on MRI. She was diagnosed with meningeal tuberculosis and treated with anti-tubercular drugs along with corticosteroids and mannitol. Her symptoms improved and she was discharged on medications including rifampicin, isoniazid, ethambutol and pyrazinamide to complete the full course of treatment over several months and ensure adherence to prevent relapse or drug resistance.Senior Medillectuals Prelims
Senior Medillectuals Prelims Quaesitum MAMC Quiz Club
╠²
The document contains questions related to various medical topics. It includes 23 multiple choice and matching questions testing knowledge on subjects like pulmonary hypertension, drug exposure in pregnancy, ECG patterns, GCS scoring, radiology, pediatric growth parameters, inborn errors of metabolism, diabetes insipidus, SLE criteria, ARDS management, reproductive endocrinology, biochemical tests, infectious diseases, arrhythmias, neurology, and procedures.Similar to Pgtd (20)
A case presentation on Molar pregnancy
A case presentation on Molar pregnancyDr. Tanvir
╠²
This case presentation describes a 24-year-old woman who presented with complaints of amenorrhea for 21+ weeks, per vaginal bleeding for two days, and passage of grape-like substances for one day. Her medical history and examination findings were presented. Initial diagnosis of a molar pregnancy was made based on her history and ultrasound findings. She underwent suction and evacuation surgery, which confirmed the diagnosis of a molar pregnancy based on histopathology. She was discharged with advice for follow up, contraception, and monitoring of beta hCG levels. The case discussion then provides an overview of gestational trophoblastic diseases including classification, etiology, pathogenesis, clinical features and management of hydatidiform mole.Case Presentation Rh negative pregnancy.pptx
Case Presentation Rh negative pregnancy.pptx25charunethrasriniva
╠²
The document presents a case study of a 25-year-old pregnant woman, Mrs. Sudha, who is Rh-negative and currently 37 weeks and 6 days into her pregnancy. She has undergone all necessary immunizations and investigations, with no significant medical complications, and is carrying a single live fetus in a longitudinal cephalic position. The treatment plan includes administration of anti-D immunoglobulin and routine evaluations leading up to delivery at 40 weeks.35 yr old pregnant lady with painless per vaginal bleeding
35 yr old pregnant lady with painless per vaginal bleedingMohammed Shadman Shakib
╠²
A 35-year-old pregnant woman, Mrs. Maleka, presented with painless vaginal bleeding at 34 weeks of gestation and generalized weakness. Her obstetric history includes one normal vaginal delivery and one cesarean due to placenta previa. Provisional diagnosis is antepartum hemorrhage due to placenta previa with breech presentation, and she is currently managed with expectant care and close monitoring until a scheduled cesarean section at 37 weeks.OBS AND GYNAE APH case presentation
OBS AND GYNAE APH case presentationSohailislam12
╠²
This document presents a case study of a 22-year-old pregnant woman, Rupa Serung, who is 38 weeks pregnant and was admitted to the hospital with bleeding per vagina. On examination, she was found to have a grade II placenta previa. Tests showed signs of anemia. An ultrasound confirmed a single fetus in longitudinal lie and cephalic presentation with a low-lying placenta. The diagnosis was grade II placenta previa. The options for management include either expectant management with bed rest or immediate termination of the pregnancy depending on the status of the mother and fetus.Case report Obstetric and Gynecological (obgyn)
Case report Obstetric and Gynecological (obgyn)osamah alfentokh
╠²
The case report details a 46-year-old Saudi housewife presenting with persistent vaginal bleeding post-menopause. Following a medical history review and physical examination, she was diagnosed with endometrial cancer and scheduled for a total abdominal hysterectomy along with a bilateral salpingo-oophorectomy. Pre-operative evaluations by cardiology and anesthesia were also planned to ensure patient safety.Placenta Accreta Spectrum.pptx
Placenta Accreta Spectrum.pptxFawad Mueen Arbi
╠²
This patient presented with retained placenta after a vaginal delivery. Her ultrasound and MRI showed placenta increta, where placental villi had invaded into the myometrium. She was initially managed conservatively with methotrexate injection, which led to a partial reduction in her beta-hCG levels. However, she later developed heavy bleeding and required an emergency hysterectomy. Placenta accreta spectrum (PAS) describes abnormal placental invasion that can cause life-threatening bleeding. Risk factors include prior uterine surgery. Management challenges include delayed referrals, lack of blood product availability, and counseling patients on prolonged hospitalization sometimes required.Intrauterine fetal demise
Intrauterine fetal demiseAnuradha Sawant
╠²
This document summarizes the case of a 36-week pregnant primigravida woman who presented with absent fetal movements for 2 days and was diagnosed with intrauterine fetal demise. Her antenatal period was otherwise uneventful. Evaluation of the stillborn fetus, placenta, and maternal factors found no anomalies or risks except for acute chorioamnionitis seen on placental histopathology. A thorough evaluation was conducted including autopsy, cultures, and genetic testing to investigate the cause, though it remained undetermined.Case Presentation of Placenta Accreta.pptx
Case Presentation of Placenta Accreta.pptxHeartMind1
╠²
The document presents the clinical profile of a 30-year-old female patient with a history of two previous cesarean sections, now presenting with a third pregnancy at 38 weeks gestation. The diagnosis includes placenta accreta, and the patient undergoes an elective cesarean section with a planned hysterectomy due to significant blood loss during surgery. Postoperative management involves monitoring in the ICU, highlighting the risks associated with this condition.CHORIOCARCINOMA case & presntn-Dr.Mohammad.ashraful amin
CHORIOCARCINOMA case & presntn-Dr.Mohammad.ashraful aminMohammad Asif
╠²
This document presents a case study of a 27-year-old female patient named Shila Rani who presented with symptoms of amenorrhea for 6 weeks, vomiting for 12 days, chest tightness for 12 days, and fever and weakness for 12 days. On examination, she appeared ill with respiratory distress. Tests revealed mild anemia, elevated white blood cell count and beta-HCG levels, suggestive of an ectopic pregnancy in the left ovary with metastasis to the lungs. She was diagnosed with choriocarcinoma and referred to an oncologist for chemotherapy with methotrexate.forcep delivery copy.pdf
forcep delivery copy.pdfJitenLad2
╠²
This case presentation summarizes the forceps delivery of a primigravida woman. The 26-year-old woman, at 38 weeks gestation, was admitted with abdominal pain and found to be in latent labor. After progressing to full dilation, she was unable to bear down effectively. An outlet forceps delivery was performed under local anesthesia due to maternal exhaustion. A baby girl was delivered in good condition, and the placenta was removed manually with an intact membrane. Both mother and baby recovered well.Labor Room Stats.pptx
Labor Room Stats.pptxrobinson405376
╠²
The patient presented at 28 weeks gestation with abdominal pain and vomiting. Her obstetric history included one full term normal delivery. On examination, she had tachycardia and hypotension. An ultrasound at the referring hospital showed an intrauterine fetal demise. She was referred for further management.Obstetrics and gynaecology seminar a case of Intrauterine Growth Restriction
Obstetrics and gynaecology seminar a case of Intrauterine Growth RestrictionAnandarup Das
╠²
SFH = 34 cm
’éĘ Fetal parts = head felt in the lower abdomen.
’éĘ Presentation = Cephalic.
’éĘ Lie = Longitudinal.
’éĘ Attitude = Flexed.
’éĘ Fetal movement = Felt.
’éĘ Fetal heart sound = Heard.
’éĘ Placenta = Not felt separately.
3. AUSCULTATION
’éĘ Fetal heart sound = Heard, rate = 140/min.
’éĘ Fetal movement = Heard.
4. FUNDAL GRASP
’éĘ Contraction = None.
5. PALPRH NEGATIVE.pptx
RH NEGATIVE.pptxdivya kumar
╠²
This case presentation is for a 45-year-old primigravida woman at 32+2 weeks of gestation who came in for prophylactic steroid coverage due to her advanced maternal age and IVF conception. Her pregnancy has been uncomplicated with good prenatal care. On examination, her vital signs were normal and her pregnancy appeared to be progressing well.matrn mortility (3).pptx
matrn mortility (3).pptxkajalgupta681731
╠²
This document summarizes a maternal mortality audit discussing a patient who presented with postpartum hemorrhage after a stillbirth. The 24-year-old patient delivered a stillborn baby at 34 weeks gestation and experienced atonic PPH. She received initial management at another hospital but was referred for further care due to continued bleeding and deterioration. Upon arrival, her condition was poor. Despite aggressive management including blood transfusions, uterotonic drugs, uterine packing and balloon tamponade, her condition continued to decline and she suffered cardiac arrest. She could not be revived after extensive resuscitation efforts and was declared dead. The audit discusses her clinical course, management, and cause of death from postpartum hemorrhage.Incomplete abortion.pptx
Incomplete abortion.pptxDrNajmulIslam1
╠²
This document presents a case study of a 34-year-old woman admitted to the hospital with heavy vaginal bleeding and weakness. On examination, she was found to have a bulky uterus and vaginal bleeding. Tests showed low hemoglobin and a positive pregnancy test. Ultrasound revealed retained products of conception in the uterus. She was diagnosed with incomplete abortion and shock. Treatment included blood transfusion, antibiotics, and misoprostol to complete the abortion. Her condition improved and she was discharged with medications and advice to rest and use contraception.CASE PRESENTATION ON occipito fronto presentation
CASE PRESENTATION ON occipito fronto presentation JitenLad2
╠²
This document presents a case study of a 26-year-old primigravida woman at 38 weeks and 4 days of twin pregnancy who presented with abdominal pain. On examination, she was found to be in active labor with an occiput posterior fetal position. She underwent an emergency lower segment cesarean section due to lack of descent of the fetal head after full cervical dilation. The procedure was uncomplicated and she was discharged on postpartum day 4 in stable condition.Grand round 24 nov case discussion. .pptx
Grand round 24 nov case discussion. .pptxauxietaks
╠²
The document details the medical history and current condition of a 25-year-old patient with a complicated obstetric history, including a recent miscarriage and ongoing symptoms related to septic abortion and potential incomplete miscarriage. It outlines her vital signs, lab results, and management plans, including admissions, medication regimens, and consultations with specialists. Additionally, the document discusses another case of a patient with deep vein thrombosis (DVT) and symptomatic anemia related to abnormal uterine bleeding, emphasizing the need for ongoing evaluation and care.Clinic psychosocial Case on Antenatal cum Post Natal Care
Clinic psychosocial Case on Antenatal cum Post Natal CareYogesh Arora
╠²
A 27-year-old woman living in Chandigarh is a third gravida at 37+4 weeks pregnant with a history of 1 previous cesarean section and 2 abdominal surgeries. She has been admitted to the hospital for a planned vaginal birth after cesarean. Her previous pregnancies and medical history were unremarkable except for a history of abdominal tuberculosis 3 years ago. On examination, she is stable and her pregnancy is progressing normally.Ad
Recently uploaded (20)
Mastering the Review Article: Structure, Strategy & Success
Mastering the Review Article: Structure, Strategy & SuccessRajendra Dev Bhatt
╠²
A scoping search identified various types of review articles. For this training, most common types were selected, highlighting their key features, strengths, weaknesses, and uses.Mindfull Midwives: MENTAL WELLBEING OF MIDWIVES FOR BETTER FOR RESPECTFUL MAT...
Mindfull Midwives: MENTAL WELLBEING OF MIDWIVES FOR BETTER FOR RESPECTFUL MAT...LaxmiDeshpande6
╠²
Midwifery practioners should be mindful while caring of mother at all stages like antenatal, postnatal ,during delivery , care of baby.Theories of Learning and Teaching.......
Theories of Learning and Teaching.......Avantika Gupta
╠²
Definition of Teaching:
ŌĆ£Teaching is a form of interpersonal influence aim at changing the behavior potential of another personŌĆØ.
Nature and Characteristics of Teaching:
’āś Teaching is giving information.
’āś Teaching is causing to learn.
’āś Teaching is a matter of helping the child to respond to his environment in an effective manner.
’āś Teaching is helping a child to adjust himself to his environment.
’āś Teaching is stimulation and encouragement.
’āś Teaching is guidance.
’āś Teaching is Training the emotions of the child.
’āś Teaching is a mean of preparation.
’āś Teaching is an art and science.
General Theory of Teaching:
The General Theory of Teaching, also known as the "Theory of Teaching" or "General Theory of Instruction," is a comprehensive framework that outlines the fundamental principles and processes of teaching.
Benefits of the General Theory of Teaching:
ŌĆó Improved Student Learning
ŌĆó Increased Teacher Efficacy
ŌĆó Enhanced Teacher Professional Development
ŌĆó Better Student Engagement
CONCLUSION
ŌĆó Teaching theory is prescriptive.
ŌĆó Teachers and pupils are the major variables of teaching theory.
ŌĆó It is narrow and specific.
ŌĆó It is based upon learning theory, learning conditions and learning components.
ŌĆó While learning theory are formulated by conducting experiments on animals teaching theory is developed by dealing with human subjects in normal situations.
ŌĆó It is concerned with effective learning and development of pupils.
Learning is a complex and multifaceted process that involves the acquisition, processing, and retention of knowledge, skills, and attitudes.
The relatively permanent change in a person's knowledge or behavior due to experience.
Characteristics of Learning:
ŌĆó Learning is Growth.
ŌĆó Learning is adjustment.
ŌĆó Learning is purposeful.
ŌĆó Learning is intelligent.
ŌĆó Learning is active.
ŌĆó Learning is both individual and social.
ŌĆó Learning is the product of the environment.
ŌĆó Learning is experience.
Learning Theory: Learning theory refers to the body of knowledge that explains how people learn and acquire new knowledge, skills, and attitudes.
Types of Teaching Theory:
1.Formal Theory of Teaching
ŌĆó Meutic Theory of teaching.
ŌĆó Communication theory of teaching.
ŌĆó Moulding theory of teaching.
ŌĆó The mutual enquiry theory.
2.Descriptive theory of teaching
ŌĆó Theories of instruction
ŌĆó Prescriptive theory of teaching
3.Normative theory of teaching
ŌĆó Cognitive theory of teaching
ŌĆó Theory of teacher behaviour
ŌĆó Psychological theory of teaching
ŌĆó General theory of teaching
FORMAL THEORY OF TEACHING
Formal theory of teaching is also known as philosophical theory. The theory which is based upon certain logic, certain metaphysical, epistemological assumptions and propositions is known as formal theory of teaching.
1.Meutic Theory of Teaching:
ŌĆó This theory conceives that teaching process helps to recollect or unfold that knowledge with questioning techniques.
ŌĆó The SocraticŌĆÖs method is an essential for this theory.
ŌĆó The heredity plays an importGrowth hormone by Dr Kondam AmbareeshaGoud
Growth hormone by Dr Kondam AmbareeshaGoudDr K Ambareesha Goud PhD
╠²
Growth hormone (GH) secretion from anterior pituitary is regulated by the hypothalamus and the mediators of GH actions. Major regulatory factors include GH releasing hormone (GHRH), somatostatin (SRIF), GH releasing peptide (ghrerin) and insulin-like growth factor (IGF-I).A Day in the Life of an Immunologist.pptx
A Day in the Life of an Immunologist.pptxClinical Immunology Laboratory, HMRUO, Oran.
╠²
My day usually begins with a short team meeting.
Then I move into the labŌĆ”ŌĆØ
To study how the immune system reactsŌĆ”...
Then I move into the clinicŌĆ”ŌĆØ
After the lab, the clinicŌĆ”ŌĆ”ŌĆ”
I return to my office
Another part of my job is teachingŌĆ”ŌĆ”. Inside the hospital and outside
Communication is also part of my job.
Another wonderful aspect of my lifeŌĆ”..
clinical studies
In the afternoons or evenings,
I often work on academic writing.
Special Research Contribution:
Special Research Contribution:
OUR SRS SBRT EXPERIENCE BY DR KANHU CHARAN PATRO
OUR SRS SBRT EXPERIENCE BY DR KANHU CHARAN PATROKanhu Charan
╠²
OUR SRS SBRT EXPERIENCE BY DR KANHU CHARAN PATRO5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...
5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...Bolan University of Medical and Health Sciences ,Quetta
╠²
Lift Analysis in ergonomics focuses on evaluating the safety and efficiency of manual lifting tasks in the workplace. It involves assessing the physical demands placed on the human body during lifting activities to prevent musculoskeletal disorders (MSDs), particularly lower back injuriesDay care surgery anaesthesia and management of complications in postoperative...
Day care surgery anaesthesia and management of complications in postoperative...deepika582423
╠²
Day care COUGH AND THIER DRUGS AND MODE OF ACTION.pptx
COUGH AND THIER DRUGS AND MODE OF ACTION.pptxPackialakshmiP
╠²
COUGH AND THIER DRUGS AND MODE OF ACTIONAnti-Infective Agents: Classification, Uses & Formulations Detailed Guide to...
Anti-Infective Agents: Classification, Uses & Formulations Detailed Guide to...Sajini
╠²
This presentation covers various classes of anti-infective agents including antifungal, antiviral, antitubercular, antimalarial, urinary tract anti-infectives, and sulphonamides. It provides classification, properties, storage conditions, uses, brand names, and pharmaceutical formulations of each drug. Ideal for pharmacy, nursing, and medical students preparing for pharmacology and mediciUnlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions
Unlocking the Potential of Long-Acting PrEP to Halt HIV TransmissionsPVI, PeerView Institute for Medical Education
╠²
Chair, Allison Agwu, MD, ScM, FAAP, FIDSA, discusses HIV in this CME/MOC/NCPD/CPE/AAPA/IPCE activity titled ŌĆ£Unlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions.ŌĆØ For the full presentation, downloadable Practice Aids, and complete CME/MOC/NCPD/CPE/AAPA/IPCE information, and to apply for credit, please visit us at https://bit.ly/40Mr2AC. CME/MOC/NCPD/CPE/AAPA/IPCE credit will be available until June 12, 2026.nanoparticle and liposomes ppt .(NTDS)pdf
nanoparticle and liposomes ppt .(NTDS)pdfsiddhikalbande
╠²
Nanoparticles and liposomes are advanced carriers used for targeted drug delivery.
Nanoparticles enhance drug effectiveness by directing treatment to specific sites.
Liposomes are biocompatible vesicles that enable controlled and sustained drug release.Drmohamedaslam_resident_copd2025_fm.pptx
Drmohamedaslam_resident_copd2025_fm.pptxAslam
╠²
COPD :LATEST GUIDELINES 2025
REFERENCE: HarrisonŌĆÖs Principles of Internal Medicine
GOLD -2025 Guidelines
It highlights updated diagnostic criteria, pharmacological and non-pharmacological treatment options, and current best practices for resident doctors and healthcare professionals.
Ideal for medical students, residents, and practitioners seeking an up-to-date, evidence-based reference.
¤æē Download, share, and feel free to reach out for related study material!Clinical Signs Overview: PICCKLE Mnemonic
Clinical Signs Overview: PICCKLE MnemonicDr Aman Suresh Tharayil
╠²
This presentation provides a concise yet comprehensive review of common clinical signs and their diagnostic significance, summarized under the acronym PICCKLE ŌĆō Pallor, Icterus, Clubbing, Cyanosis, Koilonychia, Lymphadenopathy, and Edema. Each condition is defined, followed by key causes, pathophysiology, diagnostic techniques, and clinical relevance. The content is tailored for undergraduate and postgraduate students in medicine and pharmacy, as well as early-career clinicians seeking to reinforce their clinical examination skillsComputer aided formulation development optimization
Computer aided formulation development optimizationSwami ramanand teerth marathwada university
╠²
Concept of optimization, optimization parameters, factorial design, optimization technology & screening design. AD-SAFE: An Initiative to Build Understanding of ARIA and Skills Needed to Gu...
AD-SAFE: An Initiative to Build Understanding of ARIA and Skills Needed to Gu...PVI, PeerView Institute for Medical Education
╠²
Chair and Presenter, Ana M. Franceschi, MD, PhD, and Petrice M. Cogswell, MD, PhD, discuss AlzheimerŌĆÖs disease in this CME/MOC/NCPD/CPE/AAPA/IPCE activity titled ŌĆ£AD-SAFE: An Initiative to Build Understanding of ARIA and Skills Needed to Guide Treatment Decisions and Support Rapid Recognition and Response in Radiology.ŌĆØ For the full presentation, downloadable Practice Aids, and complete CME/MOC/NCPD/CPE/AAPA/IPCE information, and to apply for credit, please visit us at https://bit.ly/42nd09H. CME/MOC/NCPD/CPE/AAPA/IPCE credit will be available until May 26, 2026.5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...
5-Lift Analysis in ergonomics focuses on evaluating the safety and efficienc...Bolan University of Medical and Health Sciences ,Quetta
╠²
Unlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions
Unlocking the Potential of Long-Acting PrEP to Halt HIV TransmissionsPVI, PeerView Institute for Medical Education
╠²
AD-SAFE: An Initiative to Build Understanding of ARIA and Skills Needed to Gu...
AD-SAFE: An Initiative to Build Understanding of ARIA and Skills Needed to Gu...PVI, PeerView Institute for Medical Education
╠²
Ad
Pgtd
- 1. CASE PRESENTATION Dr. SK. Tasnuva Alam MS Resident ,Phase-B (Obs and Gynae) Unit-IV
- 2. Name ŌĆō Yeasmin akter Age - 30yrs HusbandŌĆÖs name -Boshir Ahmed Occupation -House wife. Address - Rangamati , Date of admission -30.01.2017 Date of examination-27.04.201 PARTICULARS OF THE PATIENT
- 3. CHIEF COMPLAINTS ’āÆ Known case of invasive mole ’āÆ patient on chemotherapy
- 4. H/O OF PRESENT ILLNESS ’āÆ According to the patients statement she was alright one year back then she became amenorrhoeic for 1.5 months, her pregnancy test was positive . ’āÆ At 3 month of her pregnancy she noticed irregular p/v bleeding, which was small in amount . With this complain she visited at GOPD, Rangamati General Hospital . ’āÆ She was treated with tab. metherspan 1 tab. TDS for 3 days on 11.07.16 but her p/v bleeding continued irregularly for a month which was moderate in amount . ’āÆ With this complain again she was admitted to the same hospital & advised to do a USG of L/A & diagnosed as a case of incomplete abortion. She was advised for MVA. ’āÆ Her MVA was done on 10.08.16 by a staff nurse at Rangamati General Hospital . The attending nurse mentioned that the product of conception was grape like , but it was not sent for any examination & her bleeding continued about a month after evacuation .
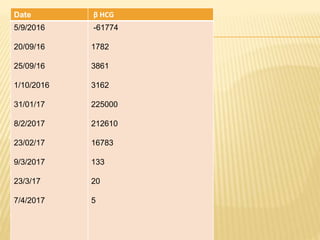
- 5. ’āÆ Then she attended GOPD at rangamati general hospital on 14.09.16 [0ne month after evacuation] this time she was attended by a senior Gynae consultant and was advised to do a s.╬▓ HCG from chittagong city [ done from chevron ; 61000 m IU/l ,5.09.16 ] . With this report she was referred to CMCH for further management . ’āÆ But she got admitted in a private hospital & received two unit of blood trasnsfusion , had some investigation s: [s.╬▓ HCG-8800.30 m IU /L ,11.09.16] referred to CMCH for further Rx. ’āÆ she went to AD ŌĆōDin Hospital Dhaka , ’āÆ Diagnosed as a case of incomplete abortion ’āÆ D & C done on ( 19.09.16 )[ 2nd time ] ’āÆ investigations done at AD Din hospital : ’é¦ s.╬▓ HCG 1782 m IU /L ( 21.09.16) ’é¦ CBC : ’é¦ HB%- 9.6 g/dl ’é¦ ESR- 40 mm in 1st hr ’é¦ WBC : ’é¦ TC-8.63X10^3/ uL ’é¦ Platelet -405x10^3/ uL ’é¦ Histopatology report : suggestive of product of conception .
- 6. ’é¦ s.╬▓ HCG 3861 m IU /L ( 25. 09.16) ’é¦ s.╬▓ HCG 3162m IU /L ( 01.10.16) ’āÆ After that her bleeding stopped she returned to Rangamati with advice to came F/U after two weeks . ’āÆ But her bleeding starts 3/4 days after her discharge ,then she admitted herself at AD ŌĆō Din hospital after admission she had a ’āÆ USG of L/A impression : Suggestive of persistent trophoblastic disease with right ovarian cyst. ’āÆ so her gynecologist advised for hysterectomy but she refused . ’āÆ Then she consulted with an other gynecologist of AD-Din was advised for D & C. ; ’āē .
- 7. ’āē On 6th november she had her 3rd D n C . ’āē Tissue Send For Histopathology Report : Fragments of endometrial tissue show invasive foci of trophoblastic cells. Features are suggestive mole or choriocarcinoma. ’āÆ They referred her to DMC for further management . but she refused to take treatment and went home . ’āÆ She had on and off p/v bleeding which was not alarming . ThatŌĆÖs why she didnŌĆÖt came for follow up . ’āē Then around three months after she had severe p/v bleeding followed by unconsciousness was admitted to Rangamati medical college on 29.01.17 . there she was managed with two units of blood & referred to CMCH for further management .
- 8. ’āÆ She admitted on our unit as an emergency case on 30.01 .17at 9.00 pm ’āÆ On admission ’āē Appearance ŌĆōanxious ’āē Anaemia ŌĆō ++ ’āē BP- 90/70 mm of Hg ’āē PULSE ŌĆō 110 b/min ’āē R/R ŌĆō30 b/min ’āē Heart ŌĆō NAD ’āē Lungs ŌĆōNAD ’āē U/O -100 ml ’āÆ P/A/E: NAD ’āÆ P/V/E: ’āē Ut- bulky ’āē Os ŌĆō Closed ’āē Bleeding ŌĆō +
- 9. Management : ’āÆ Diet : liquid ’āÆ O2 inhalation 4-6 litter ’āÆ INJ : plasmasol 500 ml IV running ’āÆ INJ. Hartsol 1L IV running then ’āÆ inj. Cefron 1 gm IV stat then BD ’āÆ cap. Omep 20 mg 1+0+1 continious catheterization Blood trasnfusion 2 unit
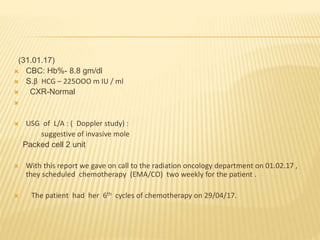
- 10. (31.01.17) ’āÆ CBC: Hb%- 8.8 gm/dl ’āÆ S.╬▓ HCG ŌĆō 225OOO m IU / ml ’āÆ CXR-Normal ’āÆ ’āÆ USG of L/A : ( Doppler study) : suggestive of invasive mole Packed cell 2 unit ’āÆ With this report we gave on call to the radiation oncology department on 01.02.17 , they scheduled chemotherapy (EMA/CO) two weekly for the patient . ’āÆ The patient had her 6th cycles of chemotherapy on 29/04/17.
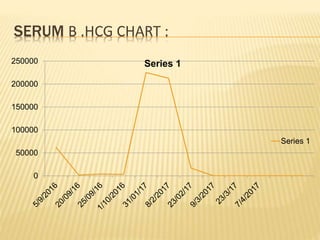
- 13. SERUM Β .HCG CHART : 0 50000 100000 150000 200000 250000 Series 1 Series 1
- 14. H/O past illness: She gave no H/O HTN,DM,Asthma she gave h/o chronic constipation. Personal History: No H/o smoking and betel nut chewing. Family history : Nothing contributory.
- 15. Socioeconomic History: She came from middle class family. Drug History: Nothing significant
- 16. MENSTRUAL HISTORY Menarche at - 13 years MP/MC : 3-4 d/28-30 d LMP : canŌĆÖt mention Contraceptive history- She took ocp irregularly for last 3 year now she is using barrier method
- 17. OBSTETRIC HISTORY Married for 11 years Para-2( NVD)+1( invasive mole ) ALC-5 yrs
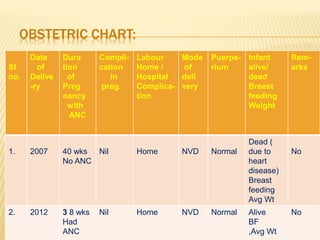
- 18. OBSTETRIC CHART: Sl no. Date of Delive -ry Dura tion of Preg nancy with ANC Compli- cation in preg. Labour Home / Hospital Complica- tion Mode of deli very Puerpe- rium Infant alive/ dead Breast feeding Weight Rem- arks 1. 2007 40 wks No ANC Nil Home NVD Normal Dead ( due to heart disease) Breast feeding Avg Wt No 2. 2012 3 8 wks Had ANC Nil Home NVD Normal Alive BF ,Avg Wt No
- 19. PHYSICAL EXAMINATION General examination: Appearance- anxious Body builds and nutrition- average Anaemia- absent Jaundice- absent Edema- absent Lymph nodes-not palpable
- 20. Pulse- 80 beats /min BP- 110/80 mm of Hg Temperature- 98.4┬░ F Respiratory rate-14 breaths/min Heart- NAD Lungs- NAD Thyroid gland ŌĆō Not enlarged Breasts- No abnormality detected
- 21. P/A EXAMINATION No abnormality detected. PELVIC EXAMINATION: Inspection: vulva & perineum looks healthy. Per speculum: not done Bi manual examination: Not done Per rectal exam: Not done
- 22. INVESTIGATION (21.04.17) ’āÆ CBC Hb-11.8 gm/dl ESR-40mm/1st hour TC- 8800/cmm Platelet count-2,33000/cm m ’āÆ SGPT ŌĆō 25 U/L ’āÆ SGOT-23 U/L ’āÆ S.urea -20.9 mg/dl ’āÆ S. billirubin - .2 mg/dl ’āÆ S.creatinine- .7 mg/d
- 23. MANAGEMENT ’āÆ General management: ’āÆ Counselling ’āÆ Improvement of general health. Definitive management: ’āÆ chemotherapy
- 24. THANK YOU