
![25歳男性 腹部膨満感
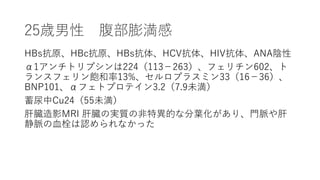
穿刺を行い、透明な黄色の腹水3.5リットルを吸引した。
白血球数 245/ml(好中球32%、リンパ球28%、組織球39%、好塩
基球1%)、赤血球数 1095/ml
アルブミン 2.5 g/dL(血清-腹水アルブミン 差[SAAG] 1.6 g/dL)、
総タンパク4.7 g/dL、LDH 106U/L、アミラーゼ18U/L、TG
56mg/dL
グラム染色は陰性、細菌及び真菌培養は陰性、抗酸菌染色は陰性
であった
抗酸菌培養の結果はまだ出ていない。細胞学的解析では悪性細胞
は認められなかった。](https://image.slidesharecdn.com/40-200108134521/85/40-the-right-angle-8-320.jpg)
40. the right angle
- 1. 40. The Right Angle 25歳男性 腹部膨満感 N Engl J Med 2011;364:1350-6.
- 5. 25歳男性 腹部膨満感 白血球数10,300/m3, Hb14.3 g/dL, 血小板数179,000/m3 Na 138mmol/L,K 4.2 mmol/L,クレアチニン0.9 mg/dL, グルコース98mg/dL,AST 23U/L,ALT 29U/L,ALP 122U/L, T-Bil 2.1 mg/dL, D-Bil1.0 mg/dL, 総蛋白質7.3 g/dL,アルブミン 4.1 g/dL,リパーゼ14U/dL PT12.7秒(PT-INR,1.2), APTT29.9秒
- 6. 25歳男性 腹部膨満感 白血球数10,300/m3, Hb14.3 g/dL, 血小板数179,000/m3 Na 138mmol/L,K 4.2 mmol/L,クレアチニン0.9 mg/dL, グルコース98mg/dL,AST 23U/L,ALT 29U/L,ALP 122U/L, T-Bil 2.1 mg/dL, D-Bil1.0 mg/dL, 総蛋白質7.3 g/dL,アルブミン 4.1 g/dL,リパーゼ14U/dL PT12.7秒(PT-INR,1.2), APTT29.9秒
- 8. 25歳男性 腹部膨満感 穿刺を行い、透明な黄色の腹水3.5リットルを吸引した。 白血球数 245/ml(好中球32%、リンパ球28%、組織球39%、好塩 基球1%)、赤血球数 1095/ml アルブミン 2.5 g/dL(血清-腹水アルブミン 差[SAAG] 1.6 g/dL)、 総タンパク4.7 g/dL、LDH 106U/L、アミラーゼ18U/L、TG 56mg/dL グラム染色は陰性、細菌及び真菌培養は陰性、抗酸菌染色は陰性 であった 抗酸菌培養の結果はまだ出ていない。細胞学的解析では悪性細胞 は認められなかった。
- 11. 25歳男性 腹部膨満感 経頸静脈肝生検は、慢性静脈流出閉塞と一致する洞様拡張を伴う 細胞周囲線維症を示したが、肝硬変は認めなかった 経頸静脈肝圧力測定で右心房静脈圧上昇(32 mm Hg)、肝静脈 圧上昇(30 mm Hg)が認められたが、体循環勾配はなかった (肝静脈楔入圧32 mm Hg) 経胸壁心エコー検査は技術的に困難だったが、正常な左心室の サイズと機能で、弁膜症はなく、軽度の右心房と心室の拡大が示 唆された 心室中隔の異常な「跳ね返り」が記録された 推定右室収縮期圧は20 mm Hg(推定右心房圧5 mm Hg )
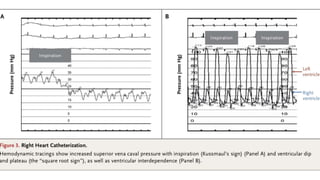
- 12. 25歳男性 腹部膨満感 心臓カテーテル検査により、右心房圧??(29 mm Hg)、肺毛細血管 楔入圧??(30 mm Hg)、肺動脈圧??(45/30 mm Hg;平均36 mm Hg)、右心室の上昇と均等化が明らかになった 右室拡張期圧(30 mm Hg)、左室拡張期圧(30 mm Hg) 心指数は大幅に減少していた(熱希釈法:1.68リットル、フィック 法:1.87リットル) 右室造影では上大静脈圧の吸気時の上昇を示した(クスマウルの兆 候) 右室のdip and plateau(「平方根サイン」)、右心室と左心室の相互 依存性も明らかだった 冠動脈造影は正常
- 13. 25歳男性 腹部膨満感 心臓カテーテル検査により、右心房圧??(29 mm Hg)、肺毛細血管 楔入圧??(30 mm Hg)、肺動脈圧??(45/30 mm Hg;平均36 mm Hg)、右心室の上昇と均等化が明らかになった 右室拡張期圧(30 mm Hg)、左室拡張期圧(30 mm Hg) 心指数は大幅に減少していた(熱希釈法:1.68リットル、フィック 法:1.87リットル) 右室造影では上大静脈圧の吸気時の上昇を示した(クスマウルの兆 候) 右室のdip and plateau(「平方根サイン」)、右心室と左心室の相互 依存性も明らかだった 冠動脈造影は正常
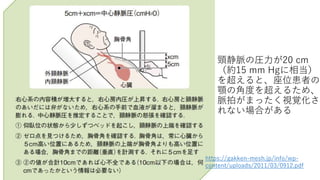
- 17. ショートサマリー 頸静脈の圧力が20 cm (約15 mm Hgに相当) を超えると、座位患者の 顎の角度を超えるため、 脈拍がまったく視覚化さ れない場合がある https://gakken-mesh.jp/info/wp- content/uploads/2011/03/0912.pdf
Editor's Notes
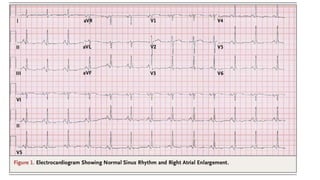
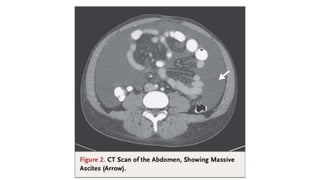
- #7: An electrocardiogram showed sinus rhythm with right atrial enlargement (Fig. 1). An ultraso- nographic examination of the abdomen showed marked ascites with splenomegaly and a mild in- crease in liver echodensity. Computed tomogra- phy (CT) of the abdomen and pelvis showed mas- sive ascites and splenomegaly (Fig. 2).
- #8: An electrocardiogram showed sinus rhythm with right atrial enlargement (Fig. 1). An ultraso- nographic examination of the abdomen showed marked ascites with splenomegaly and a mild in- crease in liver echodensity. Computed tomogra- phy (CT) of the abdomen and pelvis showed mas- sive ascites and splenomegaly (Fig. 2).
- #10: The syndrome was first reported in 1955 by Cronkhite and Canada, who described two pa- tients with a clinical syndrome of gastrointestinal polyposis with hair loss, hyperpigmentation, and nail atrophy.1
- #14: A 上大静脈圧 吸気で上昇:クスマウル
- #17: The syndrome was first reported in 1955 by Cronkhite and Canada, who described two pa- tients with a clinical syndrome of gastrointestinal polyposis with hair loss, hyperpigmentation, and nail atrophy.1
- #18: The syndrome was first reported in 1955 by Cronkhite and Canada, who described two pa- tients with a clinical syndrome of gastrointestinal polyposis with hair loss, hyperpigmentation, and nail atrophy.1
- #19: The syndrome was first reported in 1955 by Cronkhite and Canada, who described two pa- tients with a clinical syndrome of gastrointestinal polyposis with hair loss, hyperpigmentation, and nail atrophy.1