CHEST CT SCAN PRESENTATION FOR NEW RADIOGRAPHERS AND CT SCAN TECHNICIANS .pptx
Download as PPTX, PDF0 likes38 views
chest ct scan presentation for new radiographers and ct scan technicians
1 of 16
Download to read offline





Recommended
ctaheadandneckyash-190917182954.pdf
ctaheadandneckyash-190917182954.pdfBrian Sells
?
Computerized tomographic angiography (CTA) uses CT imaging with intravenous iodinated contrast to visualize blood vessels. It can be used to assess conditions like aneurysms, atherosclerosis, and tumors. For a head and neck CTA, iodinated contrast is power injected at 4-5 ml/s, followed by a saline flush. Scanning is timed to maximize arterial contrast while minimizing venous overlay. CTA requires minimizing radiation exposure while obtaining diagnostic image quality to safely evaluate head and neck vasculature.CT Angiography Head and Neck
CT Angiography Head and NeckDr. Yash Kumar Achantani
?
CT angiography (CTA) uses computed tomography (CT) and intravenous iodinated contrast to visualize blood vessels. It can be used to assess arteries, veins, and vascular structures throughout the head and neck. Performing a CTA requires optimizing multiple factors including the injection of contrast, timing of the CT scan, and image post-processing techniques. The document provides detailed guidelines on patient preparation, equipment, techniques, and safety considerations for head and neck CTA exams.CT Coronary Angiography.pptx, eart muscle) Acute angina (type of chest pain) ...
CT Coronary Angiography.pptx, eart muscle) Acute angina (type of chest pain) ...RukamaneeYadav
?
MI ( blockage of blood flow to heart muscle)
Acute angina (type of chest pain)
Aneurysms
AVM( Arterio-venous Malformations) abnormal connection between artery and vein.
eg. In spine and brain.
AVF (Arterio-venous Fistulas), LCA ,RCA EQUIPMENT
RUKAMANEE YADAV
Investigation FOR thoracic trauma
Investigation FOR thoracic traumaDr. Devkumar Sahu
?
The document summarizes various investigations used for thoracic trauma, including clinical examination, chest radiograph, ultrasound (EFAST), CT scan, and thoracentesis. A chest radiograph is the initial investigation and can reveal abnormalities like pneumothorax, hemothorax, lung pathology, and skeletal injuries. An ultrasound uses sonar to detect cardiac tamponade, free blood, and lung contusions. A CT scan provides detailed three-dimensional images of the chest and abdomen to reliably diagnose major thoracic injuries like lung contusions, hemothorax, and pneumothorax. Thoracentesis is a minimally invasive procedure used to remove fluid or air from the lungs for diagnostic and therapeutic purposes.ct angiography and pre and post scans by WAQAS MAHMOOD RIT 6TH SEMESTER.pptx
ct angiography and pre and post scans by WAQAS MAHMOOD RIT 6TH SEMESTER.pptxWaqasMahmood55
?
CT ANGIOGRAPHYEsc aortic diseases pptx new skd
Esc aortic diseases pptx new skdSoumya Kanti Dutta
?
The document discusses guidelines for the diagnosis and treatment of aortic diseases. It covers the epidemiology of aortic aneurysms and aortic dissection, providing statistics on prevalence and mortality. It also describes the clinical assessment and various imaging modalities used to evaluate the aorta, including echocardiography, CT, MRI, and angiography. Recommendations are presented regarding imaging and measurement of the aorta, as well as medical, endovascular, and surgical treatment approaches for different aortic conditions.Transverse Aortic Constriction: The Importance of Monitoring Surgical Outcomes
Transverse Aortic Constriction: The Importance of Monitoring Surgical OutcomesScintica Instrumentation
?
This free webinar hosted by Scintica Instrumentation reviewed with the viewer the importance of monitoring their surgical outcomes, specifically following transverse aortic constriction (TAC)
Join Tonya Coulthard as she discussed some background information about the TAC surgery, variability in the surgical outcomes and how to monitor those, as well as the importance of stratifying animals based on severity of constriction prior to initiating any form of intervention.
View more here https://www.scintica.com/webinar-transverse-aortic-constriction-the-importance-of-monitoring-surgical-outcomes/Upper Extrem CT Venography_Hallett_2017_sm.pdf
Upper Extrem CT Venography_Hallett_2017_sm.pdfMonicaKamal5
?
CT venography is a technique used to assess venous anatomy and determine patency. It can be performed using direct or indirect methods. Direct CTV involves slowly infusing diluted contrast directly into veins of interest. Indirect CTV uses a larger bolus of full-strength contrast followed by a delayed scan to image recirculating contrast in the veins. CTV provides non-invasive evaluation of venous anatomy from the upper extremities to the pelvis with good spatial resolution and ability to combine with arterial imaging. It is useful for evaluating issues like deep vein thrombosis, thoracic outlet syndrome, and superior vena cava syndrome.Cardiac output monitoring 
Cardiac output monitoring pbsherren
?
This document discusses various techniques for monitoring cardiac output (CO), including invasive and non-invasive options. It provides details on pulmonary artery catheters, the Fick principle, transesophageal echocardiography, esophageal Doppler, pulse contour analysis methods (PiCCO, LiDCO, Flowtrac), transthoracic bioimpedance, and transthoracic echocardiography. While some methods like pulmonary artery catheters and LiDCO are well-validated, the document notes that rigorous validation studies are still needed for newer non-invasive options like Flowtrac and transthoracic bioimpedance. Overall, it emphasizes understanding the limitations of different CO monitoring systems and using trends overOptimization of ct scan protocol in acute abdomen 2003 revised aa
Optimization of ct scan protocol in acute abdomen 2003 revised aaHisham Khatib
?
This document provides guidance on optimizing CT scan protocols for evaluating acute abdomen. It defines acute abdomen and lists common causes such as appendicitis, cholecystitis, and bowel obstruction. The document recommends CT as the best first-line imaging modality for evaluating upper right quadrant and pelvic pain. It provides details on oral, IV, and rectal contrast administration as well as scanning parameters and protocols for common acute abdomen conditions to optimize diagnostic image quality while minimizing radiation dose.Ct thorax
Ct thoraxMaajid Mohi ud din
?
This document provides information about computed tomography (CT) scans of the chest, including high-resolution CT. It describes what a chest CT is used for, how it is performed, what the equipment looks like, benefits, and normal findings. A chest CT can detect abnormalities in the lungs, chest wall, heart and blood vessels. It is performed by positioning the patient on a table that slides into a donut-shaped machine. Rotating x-rays create cross-sectional images which are analyzed to diagnose conditions like lung cancer, pneumonia and tumors.cardiac output pptx
cardiac output pptxananya nanda
?
Cardiac output monitoring can be done using invasive, minimally invasive, and non-invasive methods. Invasive methods like pulmonary artery catheter use thermodilution or dye dilution to directly measure cardiac output but carry risks. Minimally invasive methods like LiDCO, PiCCO, and FloTrac use pulse contour analysis after initial calibration. Non-invasive options include thoracic bioimpedance and echocardiography. The choice of monitoring method depends on factors like accuracy, ease of use, risks, and costs. While goal-directed therapy using cardiac output monitoring may improve outcomes in some high-risk patients, large trials found no clear benefit of pulmonary artery catheters on mortality.
Chest x-ray ppt
Chest x-ray pptMhmwdFthy
?
An arterial blood gas test measures the levels of oxygen and carbon dioxide in the blood as well as blood pH. It is performed by drawing blood from an artery, usually in the wrist, groin or arm, and analyzing the sample to evaluate respiratory conditions and determine the effectiveness of oxygen therapy. The test involves inserting a small needle into the artery to collect blood, after which pressure is applied to stop any bleeding. Special preparation is generally not needed other than maintaining consistent oxygen levels if the patient uses oxygen therapy. Risks are low but can include bleeding, bruising or fainting at the puncture site.CT enhancement protocols 
CT enhancement protocols Yanan Zhai
?
This document discusses CT contrast injection protocols and timing. It provides an overview of the basics of contrast enhancement, including the phases of enhancement, timing of CECT scans, amount of contrast used, and injection rates. It also discusses protocols for specific organs and conditions like the liver, pancreas, ileus, pulmonary emboli, and anastomosis leakage. The goal is to provide optimal contrast enhancement for successful CT scans and diagnoses.


TRIPLE PHASE CT AND ITS TECHNIQUE BY VANI PUSHPA (2).pptx
TRIPLE PHASE CT AND ITS TECHNIQUE BY VANI PUSHPA (2).pptxVANI PUSHPA MUDAVATH
?
The triple phase CT scan of the abdomen involves three contrast enhanced phases (arterial, portal venous, and delayed) to accurately detect cancers in the liver, pancreas, and other abdominal organs. The arterial phase highlights hypervascular lesions, the portal venous phase shows hypovascular lesions, and the delayed phase aids in lesion characterization. Careful protocoling of contrast dose, injection rate, and timing of scans in each phase is required to obtain diagnostic images while minimizing radiation dose.Ankle brachial pressure index (ABPI)
Ankle brachial pressure index (ABPI)Jibran Mohsin
?
This document provides an overview of ankle-brachial pressure index (ABPI) testing, including definitions, indications, methodology, interpretations, and limitations. ABPI is a non-invasive test that involves measuring the blood pressure in the ankles and arms to calculate a ratio, with ratios below 0.9 indicating peripheral artery disease. The document outlines the equipment, patient positioning, measurement techniques, and calculations required to perform ABPI testing and interpret the results. Limitations include variability in measurements, inability to determine stenosis location, and overestimation in patients with calcified ankle arteries.TRIPLE PHASE CT TECHNIQUE for ct scan technicians .pdf
TRIPLE PHASE CT TECHNIQUE for ct scan technicians .pdfMMCRADIOLOGY1
?
ct scan triple phase for ct scan techniciansBiomedical Instrumentation
Biomedical Instrumentationlinsstalex
?
Measurement of blood pressure is one of the oldest physiological measurements. It originates from the heart and depends on three factors: cardiac output, artery diameter, and blood quantity. Normal values are below 120/80 mmHg. Indirect non-invasive methods like auscultation and oscillometry use an occlusive cuff on the brachial artery. Direct invasive methods involve catheter insertion but are needed for continuous accurate readings in dynamic situations. Both methods rely on measuring pressures as a cuff is inflated and deflated over the artery.Evaluation and imaging for lung SBRT
Evaluation and imaging for lung SBRTNaveen Mummudi
?
The document discusses the key steps in pre-SBRT workup including medical evaluation, tumor assessment, imaging, and motion management. It notes that patients with stage I lung cancer can be treated with surgery, sublobar resection, or SBRT depending on their risk level. For medically inoperable patients, imaging includes PET/CT and pathology confirmation if possible. Pulmonary function tests and cardiac evaluation are done. Tumor characteristics like size and location are assessed. During simulation, immobilization and respiratory motion management techniques like 4DCT are used to accurately define the tumor and organs at risk.18-09-2020 CT CORONARY ANGIOGRAM Dr.Sowmya.Dr.BGJ.pptx.pptx
18-09-2020 CT CORONARY ANGIOGRAM Dr.Sowmya.Dr.BGJ.pptx.pptxMANU38331
?
CT coronary angiography can provide detailed images of the coronary arteries. It has high temporal and spatial resolution allowing visualization of small coronary arteries. The technique uses ECG gating and retrospective reconstruction to achieve motion-free images. Various pathologies like stenosis, anomalies, plaques and bypass grafts can be evaluated. Image quality can be affected by artifacts from calcium, stents or irregular heart rates.Monitoring_New (1).pptx
Monitoring_New (1).pptxNehaMasarkar1
?
Monitoring in anaesthesia is important to assess the patient's physiological status and response to interventions. Basic monitoring includes clinical assessments while advanced monitoring uses instruments. Instrumental monitoring can assess the cardiovascular, respiratory, temperature, central nervous, and neuromuscular systems. Electrocardiography, blood pressure monitoring, capnography, pulse oximetry, and central nervous system monitors like the bispectral index and entropy are commonly used advanced monitoring methods. Each method has advantages and limitations that should be considered during anaesthesia.CECT NECK NECK ANGIOGRAPHY CAROTID ANGIOGRAPHY
CECT NECK NECK ANGIOGRAPHY CAROTID ANGIOGRAPHYRMC
?
Neck angiography cect neck angiography carotid angiography
CT scan neck angiography
Carotid angiography useful for medical radiology students thank you process explain in simple language for more content like this presentation Aortic acceleration as a noninvasive index of left ventricular contractility ...
Aortic acceleration as a noninvasive index of left ventricular contractility ...Scintica Instrumentation
?
Key topics covered during this webinar include:
Evaluating cardiac contractility using mean or peak aortic acceleration
Investigating cardiac relaxation using mitral peak early velocity to peak atrial velocity ratio
Interpreting myocardial perfusion capacity through coronary flow reserve at baseline and with disease or other conditions
How Doppler Flow Velocity measurements can be used in translational research from mice to mammals
In a recent ground-breaking publication in Scientific Reports by Nature Research, Perez et al. highlight the use of noninvasive blood flow velocity measurements to quantify cardiac contractility as a surrogate to +dP/dt max. The article titled ˇ°Aortic acceleration as a noninvasive index of left ventricular contractility in the mouseˇ± describes an alternate methodology to what is highly considered the gold standard for evaluating cardiac contractility and relaxation in preclinical research. The acute and terminal nature of acquiring +dP/dt using invasive blood pressure catheters is less than ideal, so finding a noninvasive surrogate is of great interest to the scientific research community.
Utilizing a Doppler Flow Velocity System (DFVS) from Indus Instruments, Dr. Reddy and his group show that peak acceleration in the ascending aorta can be used in place of invasive LVP catheters. This novel technique enables serial measurements in the same animal, which reduces animal-to-animal variability, allows for the use of fewer subjects, and decreases data collection time.
Please join us during our upcoming webinar on March 4th, 2021 at 11am EST to hear Dr. Reddy present his findings with a LIVE Q&A session at the end.
References:
Perez, J.E.T., Ortiz-Urbina, J., Heredia, C.P. et al. Aortic acceleration as a noninvasive index of left ventricular contractility in the mouse. Sci Rep 11, 536 (2021)Ct scan
Ct scanA.Muhammad Rezky Sulfajri
?
CT-SCAN provides concise summaries of medical documents. This document discusses the history and evolution of computed tomography (CT) scanning technology. It begins with definitions of CT scanning and diagrams of early CT scanner designs. It then summarizes the key developments, including the invention of CT scanning by Godfrey Hounsfield in 1971, the installation of the first CT prototype, and improvements in processing time. The document outlines the generations of CT scanners from first to fifth generation and describes advances in multi-slice and multi-detector array technologies. It concludes with examples of clinical applications and cases imaged with various CT techniques.Nursing process33.ppt for new student of nursing program
Nursing process33.ppt for new student of nursing programMMCRADIOLOGY1
?
this presentation is for nursing students brain mri.pdf of Afghan Society of Radiology Technologist
brain mri.pdf of Afghan Society of Radiology TechnologistMMCRADIOLOGY1
?
brain mri by Afghan Radiographer society and for Radiology Students More Related Content
Similar to CHEST CT SCAN PRESENTATION FOR NEW RADIOGRAPHERS AND CT SCAN TECHNICIANS .pptx (20)
Cardiac output monitoring
Cardiac output monitoring pbsherren
?
This document discusses various techniques for monitoring cardiac output (CO), including invasive and non-invasive options. It provides details on pulmonary artery catheters, the Fick principle, transesophageal echocardiography, esophageal Doppler, pulse contour analysis methods (PiCCO, LiDCO, Flowtrac), transthoracic bioimpedance, and transthoracic echocardiography. While some methods like pulmonary artery catheters and LiDCO are well-validated, the document notes that rigorous validation studies are still needed for newer non-invasive options like Flowtrac and transthoracic bioimpedance. Overall, it emphasizes understanding the limitations of different CO monitoring systems and using trends overOptimization of ct scan protocol in acute abdomen 2003 revised aa
Optimization of ct scan protocol in acute abdomen 2003 revised aaHisham Khatib
?
This document provides guidance on optimizing CT scan protocols for evaluating acute abdomen. It defines acute abdomen and lists common causes such as appendicitis, cholecystitis, and bowel obstruction. The document recommends CT as the best first-line imaging modality for evaluating upper right quadrant and pelvic pain. It provides details on oral, IV, and rectal contrast administration as well as scanning parameters and protocols for common acute abdomen conditions to optimize diagnostic image quality while minimizing radiation dose.Ct thorax
Ct thoraxMaajid Mohi ud din
?
This document provides information about computed tomography (CT) scans of the chest, including high-resolution CT. It describes what a chest CT is used for, how it is performed, what the equipment looks like, benefits, and normal findings. A chest CT can detect abnormalities in the lungs, chest wall, heart and blood vessels. It is performed by positioning the patient on a table that slides into a donut-shaped machine. Rotating x-rays create cross-sectional images which are analyzed to diagnose conditions like lung cancer, pneumonia and tumors.cardiac output pptx
cardiac output pptxananya nanda
?
Cardiac output monitoring can be done using invasive, minimally invasive, and non-invasive methods. Invasive methods like pulmonary artery catheter use thermodilution or dye dilution to directly measure cardiac output but carry risks. Minimally invasive methods like LiDCO, PiCCO, and FloTrac use pulse contour analysis after initial calibration. Non-invasive options include thoracic bioimpedance and echocardiography. The choice of monitoring method depends on factors like accuracy, ease of use, risks, and costs. While goal-directed therapy using cardiac output monitoring may improve outcomes in some high-risk patients, large trials found no clear benefit of pulmonary artery catheters on mortality.Chest x-ray ppt
Chest x-ray pptMhmwdFthy
?
An arterial blood gas test measures the levels of oxygen and carbon dioxide in the blood as well as blood pH. It is performed by drawing blood from an artery, usually in the wrist, groin or arm, and analyzing the sample to evaluate respiratory conditions and determine the effectiveness of oxygen therapy. The test involves inserting a small needle into the artery to collect blood, after which pressure is applied to stop any bleeding. Special preparation is generally not needed other than maintaining consistent oxygen levels if the patient uses oxygen therapy. Risks are low but can include bleeding, bruising or fainting at the puncture site.CT enhancement protocols
CT enhancement protocols Yanan Zhai
?
This document discusses CT contrast injection protocols and timing. It provides an overview of the basics of contrast enhancement, including the phases of enhancement, timing of CECT scans, amount of contrast used, and injection rates. It also discusses protocols for specific organs and conditions like the liver, pancreas, ileus, pulmonary emboli, and anastomosis leakage. The goal is to provide optimal contrast enhancement for successful CT scans and diagnoses.TRIPLE PHASE CT AND ITS TECHNIQUE BY VANI PUSHPA (2).pptx
TRIPLE PHASE CT AND ITS TECHNIQUE BY VANI PUSHPA (2).pptxVANI PUSHPA MUDAVATH
?
The triple phase CT scan of the abdomen involves three contrast enhanced phases (arterial, portal venous, and delayed) to accurately detect cancers in the liver, pancreas, and other abdominal organs. The arterial phase highlights hypervascular lesions, the portal venous phase shows hypovascular lesions, and the delayed phase aids in lesion characterization. Careful protocoling of contrast dose, injection rate, and timing of scans in each phase is required to obtain diagnostic images while minimizing radiation dose.Ankle brachial pressure index (ABPI)
Ankle brachial pressure index (ABPI)Jibran Mohsin
?
This document provides an overview of ankle-brachial pressure index (ABPI) testing, including definitions, indications, methodology, interpretations, and limitations. ABPI is a non-invasive test that involves measuring the blood pressure in the ankles and arms to calculate a ratio, with ratios below 0.9 indicating peripheral artery disease. The document outlines the equipment, patient positioning, measurement techniques, and calculations required to perform ABPI testing and interpret the results. Limitations include variability in measurements, inability to determine stenosis location, and overestimation in patients with calcified ankle arteries.TRIPLE PHASE CT TECHNIQUE for ct scan technicians .pdf
TRIPLE PHASE CT TECHNIQUE for ct scan technicians .pdfMMCRADIOLOGY1
?
ct scan triple phase for ct scan techniciansBiomedical Instrumentation
Biomedical Instrumentationlinsstalex
?
Measurement of blood pressure is one of the oldest physiological measurements. It originates from the heart and depends on three factors: cardiac output, artery diameter, and blood quantity. Normal values are below 120/80 mmHg. Indirect non-invasive methods like auscultation and oscillometry use an occlusive cuff on the brachial artery. Direct invasive methods involve catheter insertion but are needed for continuous accurate readings in dynamic situations. Both methods rely on measuring pressures as a cuff is inflated and deflated over the artery.Evaluation and imaging for lung SBRT
Evaluation and imaging for lung SBRTNaveen Mummudi
?
The document discusses the key steps in pre-SBRT workup including medical evaluation, tumor assessment, imaging, and motion management. It notes that patients with stage I lung cancer can be treated with surgery, sublobar resection, or SBRT depending on their risk level. For medically inoperable patients, imaging includes PET/CT and pathology confirmation if possible. Pulmonary function tests and cardiac evaluation are done. Tumor characteristics like size and location are assessed. During simulation, immobilization and respiratory motion management techniques like 4DCT are used to accurately define the tumor and organs at risk.18-09-2020 CT CORONARY ANGIOGRAM Dr.Sowmya.Dr.BGJ.pptx.pptx
18-09-2020 CT CORONARY ANGIOGRAM Dr.Sowmya.Dr.BGJ.pptx.pptxMANU38331
?
CT coronary angiography can provide detailed images of the coronary arteries. It has high temporal and spatial resolution allowing visualization of small coronary arteries. The technique uses ECG gating and retrospective reconstruction to achieve motion-free images. Various pathologies like stenosis, anomalies, plaques and bypass grafts can be evaluated. Image quality can be affected by artifacts from calcium, stents or irregular heart rates.Monitoring_New (1).pptx
Monitoring_New (1).pptxNehaMasarkar1
?
Monitoring in anaesthesia is important to assess the patient's physiological status and response to interventions. Basic monitoring includes clinical assessments while advanced monitoring uses instruments. Instrumental monitoring can assess the cardiovascular, respiratory, temperature, central nervous, and neuromuscular systems. Electrocardiography, blood pressure monitoring, capnography, pulse oximetry, and central nervous system monitors like the bispectral index and entropy are commonly used advanced monitoring methods. Each method has advantages and limitations that should be considered during anaesthesia.CECT NECK NECK ANGIOGRAPHY CAROTID ANGIOGRAPHY
CECT NECK NECK ANGIOGRAPHY CAROTID ANGIOGRAPHYRMC
?
Neck angiography cect neck angiography carotid angiography
CT scan neck angiography
Carotid angiography useful for medical radiology students thank you process explain in simple language for more content like this presentation Aortic acceleration as a noninvasive index of left ventricular contractility ...
Aortic acceleration as a noninvasive index of left ventricular contractility ...Scintica Instrumentation
?
Key topics covered during this webinar include:
Evaluating cardiac contractility using mean or peak aortic acceleration
Investigating cardiac relaxation using mitral peak early velocity to peak atrial velocity ratio
Interpreting myocardial perfusion capacity through coronary flow reserve at baseline and with disease or other conditions
How Doppler Flow Velocity measurements can be used in translational research from mice to mammals
In a recent ground-breaking publication in Scientific Reports by Nature Research, Perez et al. highlight the use of noninvasive blood flow velocity measurements to quantify cardiac contractility as a surrogate to +dP/dt max. The article titled ˇ°Aortic acceleration as a noninvasive index of left ventricular contractility in the mouseˇ± describes an alternate methodology to what is highly considered the gold standard for evaluating cardiac contractility and relaxation in preclinical research. The acute and terminal nature of acquiring +dP/dt using invasive blood pressure catheters is less than ideal, so finding a noninvasive surrogate is of great interest to the scientific research community.
Utilizing a Doppler Flow Velocity System (DFVS) from Indus Instruments, Dr. Reddy and his group show that peak acceleration in the ascending aorta can be used in place of invasive LVP catheters. This novel technique enables serial measurements in the same animal, which reduces animal-to-animal variability, allows for the use of fewer subjects, and decreases data collection time.
Please join us during our upcoming webinar on March 4th, 2021 at 11am EST to hear Dr. Reddy present his findings with a LIVE Q&A session at the end.
References:
Perez, J.E.T., Ortiz-Urbina, J., Heredia, C.P. et al. Aortic acceleration as a noninvasive index of left ventricular contractility in the mouse. Sci Rep 11, 536 (2021)Ct scan
Ct scanA.Muhammad Rezky Sulfajri
?
CT-SCAN provides concise summaries of medical documents. This document discusses the history and evolution of computed tomography (CT) scanning technology. It begins with definitions of CT scanning and diagrams of early CT scanner designs. It then summarizes the key developments, including the invention of CT scanning by Godfrey Hounsfield in 1971, the installation of the first CT prototype, and improvements in processing time. The document outlines the generations of CT scanners from first to fifth generation and describes advances in multi-slice and multi-detector array technologies. It concludes with examples of clinical applications and cases imaged with various CT techniques.Aortic acceleration as a noninvasive index of left ventricular contractility ...
Aortic acceleration as a noninvasive index of left ventricular contractility ...Scintica Instrumentation
?
More from MMCRADIOLOGY1 (7)
Nursing process33.ppt for new student of nursing program
Nursing process33.ppt for new student of nursing programMMCRADIOLOGY1
?
this presentation is for nursing students brain mri.pdf of Afghan Society of Radiology Technologist
brain mri.pdf of Afghan Society of Radiology TechnologistMMCRADIOLOGY1
?
brain mri by Afghan Radiographer society and for Radiology Students hedayat sehat jama for medical student of kabul
hedayat sehat jama for medical student of kabulMMCRADIOLOGY1
?
this presentation is made by our studentx-ray and ct scan registration sheet for the year of 2024t
x-ray and ct scan registration sheet for the year of 2024tMMCRADIOLOGY1
?
for x ray and ct pt registration 
abdominalctscan-150924143513-lva1-app6891.pdf
abdominalctscan-150924143513-lva1-app6891.pdfMMCRADIOLOGY1
?
An abdominal CT scan uses x-rays to create detailed cross-sectional images of the abdomen. During the test, the patient lies still on a table that slides into a scanner, which rotates an x-ray beam around the body. Images are created as "slices" and can be combined to form 3D models. An abdominal CT scan is used to detect various abdominal abnormalities such as masses, tumors, infections, kidney stones, and issues affecting the liver, gallbladder, or pancreas. Abnormal results could indicate cancers, organ problems, appendicitis, aneurysms, or other issues requiring follow-up.Incident and Complaint Reporting Documentation Quality - Tips for Channel Par...
Incident and Complaint Reporting Documentation Quality - Tips for Channel Par...MMCRADIOLOGY1
?
The document provides documentation quality tips for channel partners reporting incidents or complaints to GE Healthcare (GEHC) through incident reporting webforms. It emphasizes the importance of providing a clear and detailed problem description to help GEHC understand and assess the incident. Tips include sticking to facts, avoiding assumptions, and ensuring safety flags and device usage are accurately reported. The role of channel partners in timely incident reporting is also discussed.Recently uploaded (18)
computer classification for computer hardware.pptx
computer classification for computer hardware.pptxleonsaifullah
?
computer classification for computer hardware¸´żĚŇ»Ě׼ÓÄô󿵿ĽµĎŃÇ´óѧ±Ďҵ֤łÉĽ¨µĄĐĹ·âµČ˛ÄÁĎ×îÇżąĄÂÔ
¸´żĚŇ»Ě׼ÓÄô󿵿ĽµĎŃÇ´óѧ±Ďҵ֤łÉĽ¨µĄĐĹ·âµČ˛ÄÁĎ×îÇżąĄÂÔtaqyed
?
ÔÚĎßżěËٲą°ěĽÓÄô󱾿ƱĎҵ֤ˇ˘Ë¶ĘżÎÄĆľÖ¤Ę飬ąşÂňĽÓÄĂ´óѧλ֤ˇľqޱ1954292140ˇżżµżĽµĎŃÇ´óѧOfferŁ¬ĽÓÄĂ´ó´óѧÎÄĆľÔÚĎßąşÂňˇŁ¸ß·ÂŐ滹ԼÓÄĂ´óÎÄĆľÖ¤ĘéşÍÍâżÇŁ¬¶¨ÖĆĽÓÄô󿵿ĽµĎŃÇ´óѧłÉĽ¨µĄşÍĐŷ⡣´ćµµżÉ˛éѧŔúConcordia±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄô󿵿ĽµĎŃÇ´óѧ±Ďҵ֤(Concordia±Ďҵ֤Ęé)ˇľqޱ1954292140ˇżŃ§Î»ČĎ֤Ҫ¶ŕľĂżµżĽµĎŃÇ´óѧoffer/ѧλ֤łÉĽ¨µĄĎę˝âϸ˝Úˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľöżµżĽµĎŃÇ´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣±Ďҵ֤¶ŞĘ§ÔőĂ´ąşÂňĽÓÄĂ´óÎÄĆľąşÂňŁ¬ĽÓÄĂ´óÎÄĆľ¶¨ÖĆŁ¬ĽÓÄô󿵿ĽµĎŃÇ´óѧÎÄĆľ˛ą°ěˇľqޱ1954292140ˇż×¨ŇµÔÚĎ߶¨ÖĆĽÓÄĂ´ó´óѧÎÄĆľ±Ďҵ֤°ěŔíŁ¬¶¨×öĽÓÄô󱾿ĆÎÄĆľŁ¬ˇľqޱ1954292140ˇż¸´ÖĆĽÓÄĂ´óConcordia University completion letterˇŁ
ČçąűÄúÔÚÓ˘ˇ˘ĽÓˇ˘ĂŔˇ˘°Äˇ˘Ĺ·Ö޵ČÁôѧąýłĚÖĐ»ň»ŘąúşóŁş
1ˇ˘ÔÚĐŁĆÚĽäŇň¸÷ÖÖÔŇňδÄÜËłŔű±Ďҵˇ¶ConcordiałÉĽ¨µĄą¤ŇŐĎę˝âˇ·ˇľQ/WeChatŁş1954292140ˇżˇ¶Buy Concordia University TranscriptżěËŮ°ěŔíżµżĽµĎŃÇ´óѧ˝ĚÓý˛żŃ§ŔúČĎÖ¤Ęé±ĎҵÎÄĆľÖ¤Ę顷Ł¬Äò»µ˝ąŮ·˝±Ďҵ֤Ł»
2ˇ˘Ăć¶Ô¸¸Ä¸µÄŃąÁ¦Ł¬ĎŁÍűľˇżěÄõ˝Ł»
3ˇ˘˛»ÇĺłţČĎÖ¤Á÷łĚŇÔĽ°˛ÄÁϸĂČçşÎ׼±¸Ł»
4ˇ˘»ŘąúʱĽäşÜł¤Ł¬ÍüĽÇ°ěŔíŁ»
5ˇ˘»ŘąúÂíÉĎľÍŇŞŐŇą¤×÷ˇ¶ŐýĘ˝łÉĽ¨µĄżµżĽµĎŃÇ´óѧ±Ďҵ֤Ńů±ľˇ·ˇľqޱ1954292140ˇżˇ¶±Ďҵ֤łÉĽ¨µĄĐĹ·âµČ˛ÄÁĎ×îÇżąĄÂÔConcordiaąşÂň±Ďҵ֤ˇ·°ě¸řÓĂČ˵ĄÎ»ż´Ł»ˇˇˇˇ
6ˇ˘ĆóĘÂҵµĄÎ»±ŘĐëŇŞÇó°ěŔíµÄŁ»
7ˇ˘ĐčŇŞ±¨żĽą«ÎńÔ±ˇ˘ąşÂňĂâË°łµˇ˘Âäת»§żÚˇ˘ÉęÇëÁôѧÉú´´Ňµ»ů˝đˇŁ
ĽÓÄĂ´óÎÄĆľżµżĽµĎŃÇ´óѧłÉĽ¨µĄŁ¬Concordia±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄô󿵿ĽµĎŃÇ´óѧ±Ďҵ֤(Concordia±Ďҵ֤Ęé)ˇľqޱ1954292140ˇżąúÍⱾżĆofferÔÚĎßÖĆ×÷żµżĽµĎŃÇ´óѧoffer/ѧλ֤ѧ·ÖÎŢ·¨±ĎҵÔőĂ´°ěŁżˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľöżµżĽµĎŃÇ´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣
ˇľqޱ1954292140ˇż°ěŔíżµżĽµĎŃÇ´óѧ±Ďҵ֤(Concordia±Ďҵ֤Ęé)2025ÄęÔÚĎßąşÂňˇľqޱ1954292140ˇżżµżĽµĎŃÇ´óѧoffer/ѧλ֤ˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ĽÓÄô󿵿ĽµĎŃÇ´óѧ±Ďҵ֤(Concordia±Ďҵ֤Ęé)ąúÍâ´óѧ±Ďҵ֤
ĚŘĘâÔŇňµĽÖÂÎŢ·¨±ĎҵŁ¬Ň˛żÉŇÔÁŞĎµÎŇĂÇ°ďÄú°ěŔíĎŕąŘ˛ÄÁĎŁş
Ł±ŁşÔÚżµżĽµĎŃÇ´óѧąŇżĆÁËŁ¬˛»Ďë¶ÁÁËŁ¬łÉĽ¨˛»ŔíĎëÔőĂ´°ěŁżŁżŁż
2Łş´ňËă»ŘąúÁËŁ¬ŐŇą¤×÷µÄʱşňŁ¬ĐčŇŞĚáą©ČĎÖ¤ˇ¶ConcordiałÉĽ¨µĄąşÂň°ěŔíżµżĽµĎŃÇ´óѧ±Ďҵ֤Ęé·¶±ľˇ·ˇľQ/WeChatŁş1954292140ˇżBuy Concordia University Diplomaˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·ÓĐÎÄƾȴµĂ˛»µ˝ČĎÖ¤ˇŁÓÖ¸ĂÔőĂ´°ěŁżŁżŁżĽÓÄĂ´ó±Ďҵ֤ąşÂňŁ¬ĽÓÄĂ´óÎÄĆľąşÂňŁ¬
3Łş»ŘąúÁËŐŇą¤×÷Ă»ÓĐżµżĽµĎŃÇ´óѧÎÄĆľÔőĂ´°ěŁżÓбľżĆČ´ŇŞÇó˶ʿÓÖÔőĂ´°ěŁż
°ďÄú˝âľöÔÚĽÓÄô󿵿ĽµĎŃÇ´óѧδ±ĎҵÄŃĚ⣨Concordia UniversityŁ©ÎÄĆľąşÂňˇ˘±Ďҵ֤ąşÂňˇ˘´óѧÎÄĆľąşÂňˇ˘´óѧ±Ďҵ֤ąşÂňˇ˘ÂňÎÄĆľˇ˘ČŐş«ÎÄĆľˇ˘Ó˘ąú´óѧÎÄĆľˇ˘ĂŔąú´óѧÎÄĆľˇ˘°ÄÖŢ´óѧÎÄĆľˇ˘ĽÓÄĂ´ó´óѧÎÄĆľŁ¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧÎÄĆľˇ˘ĐÂÎ÷ŔĽ´óѧÎÄĆľˇ˘°®¶űŔĽÎÄĆľˇ˘Î÷°ŕŃŔÎÄĆľˇ˘µÂąúÎÄĆľˇ˘˝ĚÓý˛żČĎÖ¤Ł¬Âň±Ďҵ֤Ł¬±Ďҵ֤ąşÂňŁ¬Âň´óѧÎÄĆľŁ¬ąşÂňČŐş«±Ďҵ֤ˇ˘Ó˘ąú´óѧ±Ďҵ֤ˇ˘ĂŔąú´óѧ±Ďҵ֤ˇ˘°ÄÖŢ´óѧ±Ďҵ֤ˇ˘ĽÓÄĂ´ó´óѧ±Ďҵ֤Ł¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧ±Ďҵ֤ˇ˘ĐÂÎ÷ŔĽ´óѧ±Ďҵ֤ˇ˘°®¶űŔĽ±Ďҵ֤ˇ˘Î÷°ŕŃŔ±Ďҵ֤ˇ˘µÂąú±Ďҵ֤Ł¬»ŘąúÖ¤Ă÷Ł¬ÁôĐĹÍřČĎÖ¤Ł¬ÁôĐĹČĎÖ¤°ěŔíŁ¬Ń§ŔúČĎÖ¤ˇŁ´Ó¶řÍęłÉľÍҵˇŁ
Ö÷ÓŞĎîÄżŁş
1ˇ˘Őćʵ˝ĚÓý˛żąúÍâѧŔúѧλČĎÖ¤ˇ¶ĽÓÄĂ´ó±ĎҵÎÄĆľÖ¤ĘéżěËŮ°ěŔíżµżĽµĎŃÇ´óѧŃĐľżÉúѧŔúÎÄĆľˇ·ˇľqޱ1954292140ˇżˇ¶ÂŰÎÄĂ»ąýżµżĽµĎŃÇ´óѧŐýĘ˝łÉĽ¨µĄˇ·Ł¬˝ĚÓý˛ż´ćµµŁ¬˝ĚÓý˛żÁô·ţÍřŐľ100%żÉ˛é.
2ˇ˘°ěŔíConcordia±Ďҵ֤Ł¬¸ÄłÉĽ¨µĄˇ¶Concordia±Ďҵ֤Ă÷°ěŔíżµżĽµĎŃÇ´óѧÔÚĎß°ěŔíÎÄĆľˇ·ˇľQ/WeChatŁş1954292140ˇżBuy Concordia University Certificatesˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·Ł¬żµżĽµĎŃÇ´óѧOfferˇ˘ÔÚ¶ÁÖ¤Ă÷ˇ˘Ń§Éúż¨ˇ˘Đŷ⡢֤Ă÷ĐŵČČ«ĚײÄÁĎŁ¬´Ó·Ŕαµ˝ÓˇË˘Ł¬´Óˮӡµ˝¸ÖÓˇĚ̽𣬸߾«·Â¶Č¸úѧУ԰ć100%Ďŕͬ.
3ˇ˘ŐćʵʹąÝČĎÖ¤Ł¨Ľ´ÁôѧČËÔ±»ŘąúÖ¤Ă÷Ł©Ł¬ĘąąÝ´ćµµżÉͨąý´óĘąąÝ˛éŃŻČ·ČĎ.
4ˇ˘ÁôĐĹÍřČĎÖ¤Ł¬ąúĽŇרҵČ˲ĹČĎÖ¤ÖĐĐÄ°ä·˘ČëżâÖ¤Ę飬ÁôĐĹÍř´ćµµżÉ˛é.
ˇ¶żµżĽµĎŃÇ´óѧѧλČĎÖ¤ÖŞşőĽÓÄĂ´ó±Ďҵ֤Ęé°ěŔíConcordiaѧŔúČĎÖ¤Ö¤ĘéąşÂňˇ·ˇľqޱ1954292140ˇżŃ§Î»Ö¤1:1ÍęĂŔ»ąÔşŁÍâ¸÷´óѧ±Ďҵ˛ÄÁĎÉϵŤŇŐŁşË®ÓˇŁ¬ŇőÓ°µ×ÎĆŁ¬¸ÖÓˇLOGOĚĚ˝đĚĚŇřŁ¬LOGOĚĚ˝đĚĚŇř¸´şĎÖصţˇŁÎÄ×ÖÍĽ°¸¸ˇµńˇ˘Ľ¤ąâŔŘÉ䡢×ĎÍâÓ«ąâˇ˘Î¸С˘¸´Óˇ·ŔαµČ·Ŕαą¤ŇŐˇŁ
ÔÚ¶ÁÖ¤Ă÷°ěŔíĽÓÄĂ´óÎÄĆľżµżĽµĎŃÇ´óѧłÉĽ¨µĄˇľqޱ1954292140ˇż¸´żĚłÉĽ¨µĄĽÓÄô󿵿ĽµĎŃÇ´óѧ±Ďҵ֤(Concordia±Ďҵ֤Ęé)ѧŔúČĎ֤ѧżĆŔŕ±đ żµżĽµĎŃÇ´óѧ±Ďҵ֤°ěŔíŁ¬°ě˶ʿѧλ֤ĽÓÄô󿵿ĽµĎŃÇ´óѧÎÄĆľ°ěŔíŁ¬ĽÓÄô󿵿ĽµĎŃÇ´óѧłÉĽ¨µĄ°ěŔíşÍŐćʵÁôĐĹČĎÖ¤ˇ˘Áô·ţČĎÖ¤ˇ˘żµżĽµĎŃÇ´óѧѧŔúČĎÖ¤ˇŁŃ§ÔşÎÄĆľ¶¨ÖĆŁ¬żµżĽµĎŃÇ´óѧ԰ćÎÄĆľ˛ą°ěŁ¬É¨ĂčĽţÎÄĆľ¶¨×öŁ¬100%ÎÄĆľ¸´żĚˇŁˇľqޱ1954292140ˇżBuy Concordia University DiplomaąşÂňĂŔąú±Ďҵ֤Ł¬ąşÂňÓ˘ąú±Ďҵ֤Ł¬ąşÂň°ÄÖޱĎҵ֤Ł¬ąşÂňĽÓÄĂ´ó±Ďҵ֤Ł¬ŇÔĽ°µÂąú±Ďҵ֤Ł¬ąşÂň·¨ąú±Ďҵ֤Ł¨qޱ1954292140Ł©ąşÂňşÉŔĽ±Ďҵ֤ˇ˘ąşÂňČđĘż±Ďҵ֤ˇ˘ąşÂňČŐ±ľ±Ďҵ֤ˇ˘ąşÂňş«ąú±Ďҵ֤ˇ˘ąşÂňĐÂÎ÷ŔĽ±Ďҵ֤ˇ˘ąşÂňĐÂĽÓƱĎҵ֤ˇ˘ąşÂňÎ÷°ŕŃŔ±Ďҵ֤ˇ˘ąşÂňÂíŔ´Î÷ŃDZĎҵ֤µČˇŁ°üŔ¨Á˱ľżĆ±Ďҵ֤Ł¬Ë¶Ęż±Ďҵ֤ˇŁ
ÁôĐĹČĎÖ¤µÄ×÷ÓĂŁş
1. Éí·ÝČĎÖ¤ŁşÁôĐĹČĎÖ¤żÉŇÔÖ¤Ă÷ÄăµÄÁôѧľŔúĘÇŐćʵµÄŁ¬ÇŇÄă»ńµĂµÄѧŔú»ňѧλĘÇŐýąćÇŇľąýČĎÖ¤µÄˇŁŐâ¶ÔÓÚһЩÓĂČ˵ĄÎ»Ŕ´ËµŁ¬ÓČĆäĘǶÔÁôѧľŔúÓи߶ČŇŞÇóµÄą«ËľŁ¨Čçżçąúą«Ëľ»ňąúÄڸ߶˹«ËľŁ©Ł¬ŐâĘÇ·ÇłŁÖŘŇŞµÄŇ»¸öĆľÖ¤ˇŁ
רҵĆŔ¶¨ŁşÁôĐĹČĎÖ¤˛»˝öČĎÖ¤ÄăµÄѧλ֤Ę飬»ą»á¶ÔÄăµÄËůѧרҵ˝řĐĐĆŔ¶¨ˇŁŐâÓĐÖúÓÚչʾÄăµÄѧĘő±łľ°Ł¬ĚرđĘǶÔÓÚąúÄÚą«Ëľ¶řŃÔŁ¬ÄÜą»ÇĺłţÁË˝âÄăËůѧרҵµÄˮƽşÍĽŰÖµˇŁ
ąúĽŇČ˲ſâČëżâŁşČĎÖ¤şóŁ¬ÄăµÄĐĹϢ˝«±»ÄÉČëąúĽŇČ˲ſ⣬˛˘ÇŇżÉŇÔÔÚąúĽŇČ˲ĹÍřµČƽ̨ÉĎչʾŁ¬ą©°üŔ¨500Çżą«ËľµČ´óĐÍą«ËľĚôѡşÍƸÓĂČ˲šŁŐâ¶ÔÓڻعúŐŇą¤×÷ĚرđĘÇ˝řČë´óą«ËľŁ¬ľßÓĐ·ÇłŁ»ýĽ«µÄ×÷ÓáŁ
2. ÁôĐĹČĎÖ¤¶ÔľÍҵµÄşĂ´¦
Ěá¸ßľşŐůÁ¦ŁşÍ¨ąýÁôĐĹČĎÖ¤Ł¬ÓČĆäĘǶÔÄăËůѧרҵµÄČĎÖ¤Ł¬żÉŇÔ´ó´óĚá¸ßÄăÔÚąúÄÚÇóְʱµÄľşŐůÁ¦ˇŁĐí¶ŕą«Ëľ¶ÔÁôѧÉú±łľ°şÍËůѧרҵÓкܸߵÄŇŞÇóŁ¬ČĎÖ¤şóµÄĐĹϢÄÜą»°ďÖúą«ËľżěËŮʶ±đ·űşĎĚőĽţµÄşňѡČˡŁInstrucciones en manual de amplificador de audio k8060 en pdf
Instrucciones en manual de amplificador de audio k8060 en pdfMariaNievesPrez
?
Amplificador de audio montaje en kit con planos y explicaciones para su implementaci¨®n en casa.Es preciso adquirir disipador aparte.Microtek Household Wires ¨C Safe & Durable Wires for Your Home
Microtek Household Wires ¨C Safe & Durable Wires for Your Homemicrotekindia00
?
Microtek provides top-quality household wires in India to keep your home safe and powered. Our wires are strong, long-lasting, and made with the best materials to prevent overheating and electrical issues.
Read More: https://www.microtek.in/product/electricals/household-wires
ĽÓÄĂ´ó±Ďҵ֤ąşÂň(¶ŕÂ׶ŕ´óѧłÉĽ¨µĄ)±«°Őł§łŇÎÄƾѧŔúČĎÖ¤
ĽÓÄĂ´ó±Ďҵ֤ąşÂň(¶ŕÂ׶ŕ´óѧłÉĽ¨µĄ)±«°Őł§łŇÎÄƾѧŔúČĎÖ¤taqyed
?
°ě±ľżĆѧλ֤ĽÓÄĂ´óÎÄĆľ¶ŕÂ׶ŕ´óѧłÉĽ¨µĄŁżˇľqޱ1954292140ˇż¸´żĚłÉĽ¨µĄĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧ±Ďҵ֤(UTSG±Ďҵ֤Ęé)ŐćʵżÉ˛éѧŔúČĎÖ¤ ¶ŕÂ׶ŕ´óѧ±Ďҵ֤°ěŔíŁ¬Ń§ĐŁŐýʽ¼ȡ֪ͨĘéĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧÎÄĆľ°ěŔíŁ¬ĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧłÉĽ¨µĄ°ěŔíşÍŐćʵÁôĐĹČĎÖ¤ˇ˘Áô·ţČĎÖ¤ˇ˘¶ŕÂ׶ŕ´óѧѧŔúČĎÖ¤ˇŁŃ§ÔşÎÄĆľ¶¨ÖĆŁ¬¶ŕÂ׶ŕ´óѧ԰ćÎÄĆľ˛ą°ěŁ¬É¨ĂčĽţÎÄĆľ¶¨×öŁ¬100%ÎÄĆľ¸´żĚˇŁˇľqޱ1954292140ˇżBuy St. George campus DiplomaąşÂňĂŔąú±Ďҵ֤Ł¬ąşÂňÓ˘ąú±Ďҵ֤Ł¬ąşÂň°ÄÖޱĎҵ֤Ł¬ąşÂňĽÓÄĂ´ó±Ďҵ֤Ł¬ŇÔĽ°µÂąú±Ďҵ֤Ł¬ąşÂň·¨ąú±Ďҵ֤Ł¨qޱ1954292140Ł©ąşÂňşÉŔĽ±Ďҵ֤ˇ˘ąşÂňČđĘż±Ďҵ֤ˇ˘ąşÂňČŐ±ľ±Ďҵ֤ˇ˘ąşÂňş«ąú±Ďҵ֤ˇ˘ąşÂňĐÂÎ÷ŔĽ±Ďҵ֤ˇ˘ąşÂňĐÂĽÓƱĎҵ֤ˇ˘ąşÂňÎ÷°ŕŃŔ±Ďҵ֤ˇ˘ąşÂňÂíŔ´Î÷ŃDZĎҵ֤µČˇŁ°üŔ¨Á˱ľżĆ±Ďҵ֤Ł¬Ë¶Ęż±Ďҵ֤ˇŁ
ČçąűÄúÔÚÓ˘ˇ˘ĽÓˇ˘ĂŔˇ˘°Äˇ˘Ĺ·Ö޵ČÁôѧąýłĚÖĐ»ň»ŘąúşóŁş
1ˇ˘ÔÚĐŁĆÚĽäŇň¸÷ÖÖÔŇňδÄÜËłŔű±Ďҵˇ¶UTSGłÉĽ¨µĄą¤ŇŐĎę˝âˇ·ˇľQ/WeChatŁş1954292140ˇżˇ¶Buy St. George campus TranscriptżěËŮ°ěŔí¶ŕÂ׶ŕ´óѧ˝ĚÓý˛żŃ§ŔúČĎÖ¤Ęé±ĎҵÎÄĆľÖ¤Ę顷Ł¬Äò»µ˝ąŮ·˝±Ďҵ֤Ł»
2ˇ˘Ăć¶Ô¸¸Ä¸µÄŃąÁ¦Ł¬ĎŁÍűľˇżěÄõ˝Ł»
3ˇ˘˛»ÇĺłţČĎÖ¤Á÷łĚŇÔĽ°˛ÄÁϸĂČçşÎ׼±¸Ł»
4ˇ˘»ŘąúʱĽäşÜł¤Ł¬ÍüĽÇ°ěŔíŁ»
5ˇ˘»ŘąúÂíÉĎľÍŇŞŐŇą¤×÷ˇ¶ŐýĘ˝łÉĽ¨µĄ¶ŕÂ׶ŕ´óѧÎÄĆľşÍѧλ֤µÄÇř±đˇ·ˇľqޱ1954292140ˇżˇ¶ÎÄĆľąşÂňUTSGżÉ˛éÁôĐĹČĎÖ¤ˇ·°ě¸řÓĂČ˵ĄÎ»ż´Ł»ˇˇˇˇ
6ˇ˘ĆóĘÂҵµĄÎ»±ŘĐëŇŞÇó°ěŔíµÄŁ»
7ˇ˘ĐčŇŞ±¨żĽą«ÎńÔ±ˇ˘ąşÂňĂâË°łµˇ˘Âäת»§żÚˇ˘ÉęÇëÁôѧÉú´´Ňµ»ů˝đˇŁ
ĽÓÄĂ´óÎÄĆľ¶ŕÂ׶ŕ´óѧłÉĽ¨µĄŁ¬UTSG±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧ±Ďҵ֤(UTSG±Ďҵ֤Ęé)ˇľqޱ1954292140ˇż±Ďҵ֤łÉĽ¨µĄĐĹ·âµČ˛ÄÁĎ×îÇżąĄÂÔ¶ŕÂ׶ŕ´óѧoffer/ѧλ֤ÎÄĆľ°ěŔíˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľö¶ŕÂ׶ŕ´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣
ĽÓÄĂ´óÎÄĆľąşÂňŁ¬ĽÓÄĂ´óÎÄĆľ¶¨ÖĆŁ¬ĽÓÄĂ´óÎÄĆľ˛ą°ěˇŁ×¨ŇµÔÚĎ߶¨ÖĆĽÓÄĂ´ó´óѧÎÄĆľŁ¬¶¨×öĽÓÄô󱾿ĆÎÄĆľŁ¬ˇľqޱ1954292140ˇż¸´ÖĆĽÓÄĂ´óSt. George campus completion letterˇŁÔÚĎßżěËٲą°ěĽÓÄô󱾿ƱĎҵ֤ˇ˘Ë¶ĘżÎÄĆľÖ¤Ę飬ąşÂňĽÓÄĂ´óѧλ֤ˇ˘¶ŕÂ׶ŕ´óѧOfferŁ¬ĽÓÄĂ´ó´óѧÎÄĆľÔÚĎßąşÂňˇŁ¸ß·ÂŐ滹ԼÓÄĂ´óÎÄĆľÖ¤ĘéşÍÍâżÇŁ¬¶¨ÖĆĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧłÉĽ¨µĄşÍĐŷ⡣ĽŮÎÄĆľ»ŘąúŐŇą¤×÷UTSG±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧ±Ďҵ֤(UTSG±Ďҵ֤Ęé)ˇľqޱ1954292140ˇżÔÚĎßÖĆ×÷ĽŮѧλ֤¶ŕÂ׶ŕ´óѧoffer/ѧλ֤×öŇ»¸öÔÚĎß±ľżĆÎÄĆľˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľö¶ŕÂ׶ŕ´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣
ĚŘĘâÔŇňµĽÖÂÎŢ·¨±ĎҵŁ¬Ň˛żÉŇÔÁŞĎµÎŇĂÇ°ďÄú°ěŔíĎŕąŘ˛ÄÁĎŁş
Ł±ŁşÔÚ¶ŕÂ׶ŕ´óѧąŇżĆÁËŁ¬˛»Ďë¶ÁÁËŁ¬łÉĽ¨˛»ŔíĎëÔőĂ´°ěŁżŁżŁż
2Łş´ňËă»ŘąúÁËŁ¬ŐŇą¤×÷µÄʱşňŁ¬ĐčŇŞĚáą©ČĎÖ¤ˇ¶UTSGłÉĽ¨µĄąşÂň°ěŔí¶ŕÂ׶ŕ´óѧ±Ďҵ֤Ęé·¶±ľˇ·ˇľQ/WeChatŁş1954292140ˇżBuy St. George campus Diplomaˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·ÓĐÎÄƾȴµĂ˛»µ˝ČĎÖ¤ˇŁÓÖ¸ĂÔőĂ´°ěŁżŁżŁżĽÓÄĂ´ó±Ďҵ֤ąşÂňŁ¬ĽÓÄĂ´óÎÄĆľąşÂňŁ¬
3Łş»ŘąúÁËŐŇą¤×÷Ă»ÓжŕÂ׶ŕ´óѧÎÄĆľÔőĂ´°ěŁżÓбľżĆČ´ŇŞÇó˶ʿÓÖÔőĂ´°ěŁż
°ďÄú˝âľöÔÚĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧδ±ĎҵÄŃĚ⣨St. George campusŁ©ÎÄĆľąşÂňˇ˘±Ďҵ֤ąşÂňˇ˘´óѧÎÄĆľąşÂňˇ˘´óѧ±Ďҵ֤ąşÂňˇ˘ÂňÎÄĆľˇ˘ČŐş«ÎÄĆľˇ˘Ó˘ąú´óѧÎÄĆľˇ˘ĂŔąú´óѧÎÄĆľˇ˘°ÄÖŢ´óѧÎÄĆľˇ˘ĽÓÄĂ´ó´óѧÎÄĆľŁ¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧÎÄĆľˇ˘ĐÂÎ÷ŔĽ´óѧÎÄĆľˇ˘°®¶űŔĽÎÄĆľˇ˘Î÷°ŕŃŔÎÄĆľˇ˘µÂąúÎÄĆľˇ˘˝ĚÓý˛żČĎÖ¤Ł¬Âň±Ďҵ֤Ł¬±Ďҵ֤ąşÂňŁ¬Âň´óѧÎÄĆľŁ¬ąşÂňČŐş«±Ďҵ֤ˇ˘Ó˘ąú´óѧ±Ďҵ֤ˇ˘ĂŔąú´óѧ±Ďҵ֤ˇ˘°ÄÖŢ´óѧ±Ďҵ֤ˇ˘ĽÓÄĂ´ó´óѧ±Ďҵ֤Ł¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧ±Ďҵ֤ˇ˘ĐÂÎ÷ŔĽ´óѧ±Ďҵ֤ˇ˘°®¶űŔĽ±Ďҵ֤ˇ˘Î÷°ŕŃŔ±Ďҵ֤ˇ˘µÂąú±Ďҵ֤Ł¬»ŘąúÖ¤Ă÷Ł¬ÁôĐĹÍřČĎÖ¤Ł¬ÁôĐĹČĎÖ¤°ěŔíŁ¬Ń§ŔúČĎÖ¤ˇŁ´Ó¶řÍęłÉľÍҵˇŁ
Ö÷ÓŞĎîÄżŁş
1ˇ˘Őćʵ˝ĚÓý˛żąúÍâѧŔúѧλČĎÖ¤ˇ¶ĽÓÄĂ´ó±ĎҵÎÄĆľÖ¤ĘéżěËŮ°ěŔí¶ŕÂ׶ŕ´óѧąúÍâ±Ďҵ֤łÉĽ¨µĄµÄ°ěŔíÁ÷łĚˇ·ˇľqޱ1954292140ˇżˇ¶ÂŰÎÄĂ»ąý¶ŕÂ׶ŕ´óѧŐýĘ˝łÉĽ¨µĄˇ·Ł¬˝ĚÓý˛ż´ćµµŁ¬˝ĚÓý˛żÁô·ţÍřŐľ100%żÉ˛é.
2ˇ˘°ěŔíUTSG±Ďҵ֤Ł¬¸ÄłÉĽ¨µĄˇ¶UTSG±Ďҵ֤Ă÷°ěŔí¶ŕÂ׶ŕ´óѧ±Ďҵ֤Ę鲻ĽűÁËÔőĂ´°ěˇ·ˇľQ/WeChatŁş1954292140ˇżBuy St. George campus Certificatesˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·Ł¬¶ŕÂ׶ŕ´óѧOfferˇ˘ÔÚ¶ÁÖ¤Ă÷ˇ˘Ń§Éúż¨ˇ˘Đŷ⡢֤Ă÷ĐŵČČ«ĚײÄÁĎŁ¬´Ó·Ŕαµ˝ÓˇË˘Ł¬´Óˮӡµ˝¸ÖÓˇĚ̽𣬸߾«·Â¶Č¸úѧУ԰ć100%Ďŕͬ.
3ˇ˘ŐćʵʹąÝČĎÖ¤Ł¨Ľ´ÁôѧČËÔ±»ŘąúÖ¤Ă÷Ł©Ł¬ĘąąÝ´ćµµżÉͨąý´óĘąąÝ˛éŃŻČ·ČĎ.
4ˇ˘ÁôĐĹÍřČĎÖ¤Ł¬ąúĽŇרҵČ˲ĹČĎÖ¤ÖĐĐÄ°ä·˘ČëżâÖ¤Ę飬ÁôĐĹÍř´ćµµżÉ˛é.
ˇ¶¶ŕÂ׶ŕ´óѧ˝ŇĂŘĽÓÄĂ´ó±Ďҵ֤Ęé°ěŔíUTSGѧŔúÖ¤ĘéÁôѧÉúˇ·ˇľqޱ1954292140ˇżŃ§Î»Ö¤1:1ÍęĂŔ»ąÔşŁÍâ¸÷´óѧ±Ďҵ˛ÄÁĎÉϵŤŇŐŁşË®ÓˇŁ¬ŇőÓ°µ×ÎĆŁ¬¸ÖÓˇLOGOĚĚ˝đĚĚŇřŁ¬LOGOĚĚ˝đĚĚŇř¸´şĎÖصţˇŁÎÄ×ÖÍĽ°¸¸ˇµńˇ˘Ľ¤ąâŔŘÉ䡢×ĎÍâÓ«ąâˇ˘Î¸С˘¸´Óˇ·ŔαµČ·Ŕαą¤ŇŐˇŁ
ˇľqޱ1954292140ˇż°ěŔí¶ŕÂ׶ŕ´óѧ±Ďҵ֤(UTSG±Ďҵ֤Ęé)ѧλ֤ĘéąşÂňˇľqޱ1954292140ˇż¶ŕÂ׶ŕ´óѧoffer/ѧλ֤ˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ĽÓÄĂ´ó¶ŕÂ׶ŕ´óѧ±Ďҵ֤(UTSG±Ďҵ֤Ęé)Đ޸ijɼ¨µĄ
ÁôĐĹČĎÖ¤µÄ×÷ÓĂŁş
1. Éí·ÝČĎÖ¤ŁşÁôĐĹČĎÖ¤żÉŇÔÖ¤Ă÷ÄăµÄÁôѧľŔúĘÇŐćʵµÄŁ¬ÇŇÄă»ńµĂµÄѧŔú»ňѧλĘÇŐýąćÇŇľąýČĎÖ¤µÄˇŁŐâ¶ÔÓÚһЩÓĂČ˵ĄÎ»Ŕ´ËµŁ¬ÓČĆäĘǶÔÁôѧľŔúÓи߶ČŇŞÇóµÄą«ËľŁ¨Čçżçąúą«Ëľ»ňąúÄڸ߶˹«ËľŁ©Ł¬ŐâĘÇ·ÇłŁÖŘŇŞµÄŇ»¸öĆľÖ¤ˇŁ
רҵĆŔ¶¨ŁşÁôĐĹČĎÖ¤˛»˝öČĎÖ¤ÄăµÄѧλ֤Ę飬»ą»á¶ÔÄăµÄËůѧרҵ˝řĐĐĆŔ¶¨ˇŁŐâÓĐÖúÓÚչʾÄăµÄѧĘő±łľ°Ł¬ĚرđĘǶÔÓÚąúÄÚą«Ëľ¶řŃÔŁ¬ÄÜą»ÇĺłţÁË˝âÄăËůѧרҵµÄˮƽşÍĽŰÖµˇŁ
ąúĽŇČ˲ſâČëżâŁşČĎÖ¤şóŁ¬ÄăµÄĐĹϢ˝«±»ÄÉČëąúĽŇČ˲ſ⣬˛˘ÇŇżÉŇÔÔÚąúĽŇČ˲ĹÍřµČƽ̨ÉĎչʾŁ¬ą©°üŔ¨500Çżą«ËľµČ´óĐÍą«ËľĚôѡşÍƸÓĂČ˲šŁŐâ¶ÔÓڻعúŐŇą¤×÷ĚرđĘÇ˝řČë´óą«ËľŁ¬ľßÓĐ·ÇłŁ»ýĽ«µÄ×÷ÓáŁMicrosoft Office 365 Crack + Product Key Latest
Microsoft Office 365 Crack + Product Key Latesthassanjameelrt45
?
https://pcpronew.com/dn/
Imagine transforming your workflow with a tool designed for unmatched office crack download excellence and robust crack office 365 ..Computer Hardware and its classification .pptx
Computer Hardware and its classification .pptxleonsaifullah
?
Computer Hardware and its classification International-Standard-Case-Studies-in-IoT.pptx
International-Standard-Case-Studies-in-IoT.pptxQuennieTGura
?
The Current IoT Landscape: Fragmentation and the Need for Standards
Diverse ecosystem: devices, platforms, protocols, and applications.
Fragmentation hinders interoperability and scalability.
Standards promote interoperability, security, and efficiency.
Lack of standardization leads to increased costs and slower adoption rates.
Example: Smart home devices from different manufacturers often cannot communicate seamlessly.

Microtek Home UPS ¨C Best Power Backup Solutions in India
Microtek Home UPS ¨C Best Power Backup Solutions in Indiamicrotekindia00
?
Microtek provides top-quality Home UPS in India, keeping your home powered during outages. With advanced technology and reliable performance, Microtek Home UPS ensures a smooth power supply for all your needs.
Read More:https://www.microtek.in/product/power-backup-solutions/home-invertersMost Trusted Home Automation Company in India- Jasmine Smart Homes
Most Trusted Home Automation Company in India- Jasmine Smart Homessanskar01021985
?
Jasmine Smart Homes specializes in providing state-of-the-art smart home solutions that enhance comfort, security, and energy efficiency. Our products include smart lighting systems, automated thermostats, security cameras, and a virtual home assistant for seamless control of your home environment.
https://jasminesmarthomes.com/Ň»±Čһ԰ćĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤Ł¨±«µţ°ä±Ďҵ֤Ę飩ČçşÎ°ěŔí
Ň»±Čһ԰ćĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤Ł¨±«µţ°ä±Ďҵ֤Ę飩ČçşÎ°ěŔítaqyed
?
2025ÄęĐ°ć±Ďҵ֤ĘéĽÓÄĂ´óÎÄĆľ˛»Áе߸çÂ×±ČŃÇ´óѧłÉĽ¨µĄŁżˇľqޱ1954292140ˇż¸´żĚłÉĽ¨µĄĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤(UBC±Ďҵ֤Ęé)±Ďҵ֤°ěŔí ˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤°ěŔíŁ¬ÎÄĆľąşÂňĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧÎÄĆľ°ěŔíŁ¬ĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧłÉĽ¨µĄ°ěŔíşÍŐćʵÁôĐĹČĎÖ¤ˇ˘Áô·ţČĎÖ¤ˇ˘˛»Áе߸çÂ×±ČŃÇ´óѧѧŔúČĎÖ¤ˇŁŃ§ÔşÎÄĆľ¶¨ÖĆŁ¬˛»Áе߸çÂ×±ČŃÇ´óѧ԰ćÎÄĆľ˛ą°ěŁ¬É¨ĂčĽţÎÄĆľ¶¨×öŁ¬100%ÎÄĆľ¸´żĚˇŁˇľqޱ1954292140ˇżBuy The University of British Columbia DiplomaąşÂňĂŔąú±Ďҵ֤Ł¬ąşÂňÓ˘ąú±Ďҵ֤Ł¬ąşÂň°ÄÖޱĎҵ֤Ł¬ąşÂňĽÓÄĂ´ó±Ďҵ֤Ł¬ŇÔĽ°µÂąú±Ďҵ֤Ł¬ąşÂň·¨ąú±Ďҵ֤Ł¨qޱ1954292140Ł©ąşÂňşÉŔĽ±Ďҵ֤ˇ˘ąşÂňČđĘż±Ďҵ֤ˇ˘ąşÂňČŐ±ľ±Ďҵ֤ˇ˘ąşÂňş«ąú±Ďҵ֤ˇ˘ąşÂňĐÂÎ÷ŔĽ±Ďҵ֤ˇ˘ąşÂňĐÂĽÓƱĎҵ֤ˇ˘ąşÂňÎ÷°ŕŃŔ±Ďҵ֤ˇ˘ąşÂňÂíŔ´Î÷ŃDZĎҵ֤µČˇŁ°üŔ¨Á˱ľżĆ±Ďҵ֤Ł¬Ë¶Ęż±Ďҵ֤ˇŁ
ČçąűÄúÔÚÓ˘ˇ˘ĽÓˇ˘ĂŔˇ˘°Äˇ˘Ĺ·Ö޵ČÁôѧąýłĚÖĐ»ň»ŘąúşóŁş
1ˇ˘ÔÚĐŁĆÚĽäŇň¸÷ÖÖÔŇňδÄÜËłŔű±Ďҵˇ¶UBCłÉĽ¨µĄą¤ŇŐĎę˝âˇ·ˇľQ/WeChatŁş1954292140ˇżˇ¶Buy The University of British Columbia TranscriptżěËŮ°ěŔí˛»Áе߸çÂ×±ČŃÇ´óѧ˝ĚÓý˛żŃ§ŔúČĎÖ¤Ęé±ĎҵÎÄĆľÖ¤Ę顷Ł¬Äò»µ˝ąŮ·˝±Ďҵ֤Ł»
2ˇ˘Ăć¶Ô¸¸Ä¸µÄŃąÁ¦Ł¬ĎŁÍűľˇżěÄõ˝Ł»
3ˇ˘˛»ÇĺłţČĎÖ¤Á÷łĚŇÔĽ°˛ÄÁϸĂČçşÎ׼±¸Ł»
4ˇ˘»ŘąúʱĽäşÜł¤Ł¬ÍüĽÇ°ěŔíŁ»
5ˇ˘»ŘąúÂíÉĎľÍŇŞŐŇą¤×÷ˇ¶ŐýĘ˝łÉĽ¨µĄ˛»Áе߸çÂ×±ČŃÇ´óѧŐćʵżÉ˛éѧŔúČĎÖ¤ˇ·ˇľqޱ1954292140ˇżˇ¶±Ďҵ֤ąşÂňUBCłÉĽ¨µĄÎ¸йâ±ęˇ·°ě¸řÓĂČ˵ĄÎ»ż´Ł»ˇˇˇˇ
6ˇ˘ĆóĘÂҵµĄÎ»±ŘĐëŇŞÇó°ěŔíµÄŁ»
7ˇ˘ĐčŇŞ±¨żĽą«ÎńÔ±ˇ˘ąşÂňĂâË°łµˇ˘Âäת»§żÚˇ˘ÉęÇëÁôѧÉú´´Ňµ»ů˝đˇŁ
ĽÓÄĂ´óÎÄĆľ˛»Áе߸çÂ×±ČŃÇ´óѧłÉĽ¨µĄŁ¬UBC±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤(UBC±Ďҵ֤Ęé)ˇľqޱ1954292140ˇż±Ďҵ֤Ę鲻ĽűÁËÔőĂ´°ě˛»Áе߸çÂ×±ČŃÇ´óѧoffer/ѧλ֤ÄÄŔďżÉŇÔ°ěÔÚĎßÖĆ×÷±ľżĆÎÄĆľˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľö˛»Áе߸çÂ×±ČŃÇ´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣
ĽÓÄĂ´óÎÄĆľąşÂňŁ¬ĽÓÄĂ´óÎÄĆľ¶¨ÖĆŁ¬ĽÓÄĂ´óÎÄĆľ˛ą°ěˇŁ×¨ŇµÔÚĎ߶¨ÖĆĽÓÄĂ´ó´óѧÎÄĆľŁ¬¶¨×öĽÓÄô󱾿ĆÎÄĆľŁ¬ˇľqޱ1954292140ˇż¸´ÖĆĽÓÄĂ´óThe University of British Columbia completion letterˇŁÔÚĎßżěËٲą°ěĽÓÄô󱾿ƱĎҵ֤ˇ˘Ë¶ĘżÎÄĆľÖ¤Ę飬ąşÂňĽÓÄĂ´óѧλ֤ˇ˘˛»Áе߸çÂ×±ČŃÇ´óѧOfferŁ¬ĽÓÄĂ´ó´óѧÎÄĆľÔÚĎßąşÂňˇŁ¸ß·ÂŐ滹ԼÓÄĂ´óÎÄĆľÖ¤ĘéşÍÍâżÇŁ¬¶¨ÖĆĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧłÉĽ¨µĄşÍĐŷ⡣¸´żĚŇ»Ě×ÎÄĆľ¶ŕÉŮĂ×UBC±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤(UBC±Ďҵ֤Ęé)ˇľqޱ1954292140ˇż±Ďҵ֤ĘéÓ°±ľ˛»Áе߸çÂ×±ČŃÇ´óѧoffer/ѧλ֤¶¨ÖĆѧŔúÎÄĆľˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľö˛»Áе߸çÂ×±ČŃÇ´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣
ĚŘĘâÔŇňµĽÖÂÎŢ·¨±ĎҵŁ¬Ň˛żÉŇÔÁŞĎµÎŇĂÇ°ďÄú°ěŔíĎŕąŘ˛ÄÁĎŁş
Ł±ŁşÔÚ˛»Áе߸çÂ×±ČŃÇ´óѧąŇżĆÁËŁ¬˛»Ďë¶ÁÁËŁ¬łÉĽ¨˛»ŔíĎëÔőĂ´°ěŁżŁżŁż
2Łş´ňËă»ŘąúÁËŁ¬ŐŇą¤×÷µÄʱşňŁ¬ĐčŇŞĚáą©ČĎÖ¤ˇ¶UBCłÉĽ¨µĄąşÂň°ěŔí˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤Ęé·¶±ľˇ·ˇľQ/WeChatŁş1954292140ˇżBuy The University of British Columbia Diplomaˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·ÓĐÎÄƾȴµĂ˛»µ˝ČĎÖ¤ˇŁÓÖ¸ĂÔőĂ´°ěŁżŁżŁżĽÓÄĂ´ó±Ďҵ֤ąşÂňŁ¬ĽÓÄĂ´óÎÄĆľąşÂňŁ¬
3Łş»ŘąúÁËŐŇą¤×÷Ă»Óв»Áе߸çÂ×±ČŃÇ´óѧÎÄĆľÔőĂ´°ěŁżÓбľżĆČ´ŇŞÇó˶ʿÓÖÔőĂ´°ěŁż
°ďÄú˝âľöÔÚĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧδ±ĎҵÄŃĚ⣨The University of British ColumbiaŁ©ÎÄĆľąşÂňˇ˘±Ďҵ֤ąşÂňˇ˘´óѧÎÄĆľąşÂňˇ˘´óѧ±Ďҵ֤ąşÂňˇ˘ÂňÎÄĆľˇ˘ČŐş«ÎÄĆľˇ˘Ó˘ąú´óѧÎÄĆľˇ˘ĂŔąú´óѧÎÄĆľˇ˘°ÄÖŢ´óѧÎÄĆľˇ˘ĽÓÄĂ´ó´óѧÎÄĆľŁ¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧÎÄĆľˇ˘ĐÂÎ÷ŔĽ´óѧÎÄĆľˇ˘°®¶űŔĽÎÄĆľˇ˘Î÷°ŕŃŔÎÄĆľˇ˘µÂąúÎÄĆľˇ˘˝ĚÓý˛żČĎÖ¤Ł¬Âň±Ďҵ֤Ł¬±Ďҵ֤ąşÂňŁ¬Âň´óѧÎÄĆľŁ¬ąşÂňČŐş«±Ďҵ֤ˇ˘Ó˘ąú´óѧ±Ďҵ֤ˇ˘ĂŔąú´óѧ±Ďҵ֤ˇ˘°ÄÖŢ´óѧ±Ďҵ֤ˇ˘ĽÓÄĂ´ó´óѧ±Ďҵ֤Ł¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧ±Ďҵ֤ˇ˘ĐÂÎ÷ŔĽ´óѧ±Ďҵ֤ˇ˘°®¶űŔĽ±Ďҵ֤ˇ˘Î÷°ŕŃŔ±Ďҵ֤ˇ˘µÂąú±Ďҵ֤Ł¬»ŘąúÖ¤Ă÷Ł¬ÁôĐĹÍřČĎÖ¤Ł¬ÁôĐĹČĎÖ¤°ěŔíŁ¬Ń§ŔúČĎÖ¤ˇŁ´Ó¶řÍęłÉľÍҵˇŁ
Ö÷ÓŞĎîÄżŁş
1ˇ˘Őćʵ˝ĚÓý˛żąúÍâѧŔúѧλČĎÖ¤ˇ¶ĽÓÄĂ´ó±ĎҵÎÄĆľÖ¤ĘéżěËŮ°ěŔí˛»Áе߸çÂ×±ČŃÇ´óѧѧλ֤ĘéąşÂňˇ·ˇľqޱ1954292140ˇżˇ¶ÂŰÎÄĂ»ąý˛»Áе߸çÂ×±ČŃÇ´óѧŐýĘ˝łÉĽ¨µĄˇ·Ł¬˝ĚÓý˛ż´ćµµŁ¬˝ĚÓý˛żÁô·ţÍřŐľ100%żÉ˛é.
2ˇ˘°ěŔíUBC±Ďҵ֤Ł¬¸ÄłÉĽ¨µĄˇ¶UBC±Ďҵ֤Ă÷°ěŔí˛»Áе߸çÂ×±ČŃÇ´óѧÔÚĎß°ěŔíÎÄĆľˇ·ˇľQ/WeChatŁş1954292140ˇżBuy The University of British Columbia Certificatesˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·Ł¬˛»Áе߸çÂ×±ČŃÇ´óѧOfferˇ˘ÔÚ¶ÁÖ¤Ă÷ˇ˘Ń§Éúż¨ˇ˘Đŷ⡢֤Ă÷ĐŵČČ«ĚײÄÁĎŁ¬´Ó·Ŕαµ˝ÓˇË˘Ł¬´Óˮӡµ˝¸ÖÓˇĚ̽𣬸߾«·Â¶Č¸úѧУ԰ć100%Ďŕͬ.
3ˇ˘ŐćʵʹąÝČĎÖ¤Ł¨Ľ´ÁôѧČËÔ±»ŘąúÖ¤Ă÷Ł©Ł¬ĘąąÝ´ćµµżÉͨąý´óĘąąÝ˛éŃŻČ·ČĎ.
4ˇ˘ÁôĐĹÍřČĎÖ¤Ł¬ąúĽŇרҵČ˲ĹČĎÖ¤ÖĐĐÄ°ä·˘ČëżâÖ¤Ę飬ÁôĐĹÍř´ćµµżÉ˛é.
ˇ¶˛»Áе߸çÂ×±ČŃÇ´óѧÎÄĆľÔÚĎßÖĆ×÷ĽÓÄĂ´ó±Ďҵ֤Ęé°ěŔíUBC±Ďҵ֤şÍѧλ֤µÄÇř±đˇ·ˇľqޱ1954292140ˇżŃ§Î»Ö¤1:1ÍęĂŔ»ąÔşŁÍâ¸÷´óѧ±Ďҵ˛ÄÁĎÉϵŤŇŐŁşË®ÓˇŁ¬ŇőÓ°µ×ÎĆŁ¬¸ÖÓˇLOGOĚĚ˝đĚĚŇřŁ¬LOGOĚĚ˝đĚĚŇř¸´şĎÖصţˇŁÎÄ×ÖÍĽ°¸¸ˇµńˇ˘Ľ¤ąâŔŘÉ䡢×ĎÍâÓ«ąâˇ˘Î¸С˘¸´Óˇ·ŔαµČ·Ŕαą¤ŇŐˇŁ
ˇľqޱ1954292140ˇż°ěŔí˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤(UBC±Ďҵ֤Ęé)°ěĂÜ·âłÉĽ¨µĄÉęÇëѧУˇľqޱ1954292140ˇż˛»Áе߸çÂ×±ČŃÇ´óѧoffer/ѧλ֤ˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ĽÓÄĂ´ó˛»Áе߸çÂ×±ČŃÇ´óѧ±Ďҵ֤(UBC±Ďҵ֤Ęé)łÉĽ¨µĄÓ°±ľ
ÁôĐĹČĎÖ¤µÄ×÷ÓĂŁş
1. Éí·ÝČĎÖ¤ŁşÁôĐĹČĎÖ¤żÉŇÔÖ¤Ă÷ÄăµÄÁôѧľŔúĘÇŐćʵµÄŁ¬ÇŇÄă»ńµĂµÄѧŔú»ňѧλĘÇŐýąćÇŇľąýČĎÖ¤µÄˇŁŐâ¶ÔÓÚһЩÓĂČ˵ĄÎ»Ŕ´ËµŁ¬ÓČĆäĘǶÔÁôѧľŔúÓи߶ČŇŞÇóµÄą«ËľŁ¨Čçżçąúą«Ëľ»ňąúÄڸ߶˹«ËľŁ©Ł¬ŐâĘÇ·ÇłŁÖŘŇŞµÄŇ»¸öĆľÖ¤ˇŁ
רҵĆŔ¶¨ŁşÁôĐĹČĎÖ¤˛»˝öČĎÖ¤ÄăµÄѧλ֤Ę飬»ą»á¶ÔÄăµÄËůѧרҵ˝řĐĐĆŔ¶¨ˇŁŐâÓĐÖúÓÚչʾÄăµÄѧĘő±łľ°Ł¬ĚرđĘǶÔÓÚąúÄÚą«Ëľ¶řŃÔŁ¬ÄÜą»ÇĺłţÁË˝âÄăËůѧרҵµÄˮƽşÍĽŰÖµˇŁ
ąúĽŇČ˲ſâČëżâŁşČĎÖ¤şóŁ¬ÄăµÄĐĹϢ˝«±»ÄÉČëąúĽŇČ˲ſ⣬˛˘ÇŇżÉŇÔÔÚąúĽŇČ˲ĹÍřµČƽ̨ÉĎչʾŁ¬ą©°üŔ¨500Çżą«ËľµČ´óĐÍą«ËľĚôѡşÍƸÓĂČ˲šŁŐâ¶ÔÓڻعúŐŇą¤×÷ĚرđĘÇ˝řČë´óą«ËľŁ¬ľßÓĐ·ÇłŁ»ýĽ«µÄ×÷ÓáŁBuy Jumbo UPS in India ¨C MicrotekˇŻs Powerful & Reliable Solutions
Buy Jumbo UPS in India ¨C MicrotekˇŻs Powerful & Reliable Solutionsmicrotekindia00
?
Looking for a strong and reliable UPS for big power needs? Microtek offers the best Jumbo UPS in India. Perfect for homes, offices, and industries, it gives long backup and protects your devices.Etendue of microLED: fundamental theory and applications
Etendue of microLED: fundamental theory and applicationsBrian Kim, PhD
?
Etendue of microLED for AR wearable glass
Ň»±Čһ԰ć(°Ő˛Ń±«±Ďҵ֤Ęé)¶ŕÂ׶඼»á´óѧ±Ďҵ֤ČçşÎ°ěŔí
Ň»±Čһ԰ć(°Ő˛Ń±«±Ďҵ֤Ęé)¶ŕÂ׶඼»á´óѧ±Ďҵ֤ČçşÎ°ěŔí taqyed
?
ÎÄĆľĽÓÄĂ´óÎÄĆľ¶ŕÂ׶඼»á´óѧłÉĽ¨µĄŁżˇľqޱ1954292140ˇż¸´żĚłÉĽ¨µĄĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧ±Ďҵ֤(TMU±Ďҵ֤Ęé)łÉĽ¨µĄCOPY ¶ŕÂ׶඼»á´óѧ±Ďҵ֤°ěŔíŁ¬Ń§Î»ČĎ֤Ҫ¶ŕľĂĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧÎÄĆľ°ěŔíŁ¬ĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧłÉĽ¨µĄ°ěŔíşÍŐćʵÁôĐĹČĎÖ¤ˇ˘Áô·ţČĎÖ¤ˇ˘¶ŕÂ׶඼»á´óѧѧŔúČĎÖ¤ˇŁŃ§ÔşÎÄĆľ¶¨ÖĆŁ¬¶ŕÂ׶඼»á´óѧ԰ćÎÄĆľ˛ą°ěŁ¬É¨ĂčĽţÎÄĆľ¶¨×öŁ¬100%ÎÄĆľ¸´żĚˇŁˇľqޱ1954292140ˇżBuy Toronto Metropolitan University DiplomaąşÂňĂŔąú±Ďҵ֤Ł¬ąşÂňÓ˘ąú±Ďҵ֤Ł¬ąşÂň°ÄÖޱĎҵ֤Ł¬ąşÂňĽÓÄĂ´ó±Ďҵ֤Ł¬ŇÔĽ°µÂąú±Ďҵ֤Ł¬ąşÂň·¨ąú±Ďҵ֤Ł¨qޱ1954292140Ł©ąşÂňşÉŔĽ±Ďҵ֤ˇ˘ąşÂňČđĘż±Ďҵ֤ˇ˘ąşÂňČŐ±ľ±Ďҵ֤ˇ˘ąşÂňş«ąú±Ďҵ֤ˇ˘ąşÂňĐÂÎ÷ŔĽ±Ďҵ֤ˇ˘ąşÂňĐÂĽÓƱĎҵ֤ˇ˘ąşÂňÎ÷°ŕŃŔ±Ďҵ֤ˇ˘ąşÂňÂíŔ´Î÷ŃDZĎҵ֤µČˇŁ°üŔ¨Á˱ľżĆ±Ďҵ֤Ł¬Ë¶Ęż±Ďҵ֤ˇŁ
ČçąűÄúÔÚÓ˘ˇ˘ĽÓˇ˘ĂŔˇ˘°Äˇ˘Ĺ·Ö޵ČÁôѧąýłĚÖĐ»ň»ŘąúşóŁş
1ˇ˘ÔÚĐŁĆÚĽäŇň¸÷ÖÖÔŇňδÄÜËłŔű±Ďҵˇ¶TMUłÉĽ¨µĄą¤ŇŐĎę˝âˇ·ˇľQ/WeChatŁş1954292140ˇżˇ¶Buy Toronto Metropolitan University TranscriptżěËŮ°ěŔí¶ŕÂ׶඼»á´óѧ˝ĚÓý˛żŃ§ŔúČĎÖ¤Ęé±ĎҵÎÄĆľÖ¤Ę顷Ł¬Äò»µ˝ąŮ·˝±Ďҵ֤Ł»
2ˇ˘Ăć¶Ô¸¸Ä¸µÄŃąÁ¦Ł¬ĎŁÍűľˇżěÄõ˝Ł»
3ˇ˘˛»ÇĺłţČĎÖ¤Á÷łĚŇÔĽ°˛ÄÁϸĂČçşÎ׼±¸Ł»
4ˇ˘»ŘąúʱĽäşÜł¤Ł¬ÍüĽÇ°ěŔíŁ»
5ˇ˘»ŘąúÂíÉĎľÍŇŞŐŇą¤×÷ˇ¶ŐýĘ˝łÉĽ¨µĄ¶ŕÂ׶඼»á´óѧѧŔúČĎÖ¤±¨¸ćˇ·ˇľqޱ1954292140ˇżˇ¶±Ďҵ֤ĘéÓ˘ÎÄ°ćTMUÔÚÄÄŔďÔÚĎßąşÂňѧʿѧλ֤Ę顷°ě¸řÓĂČ˵ĄÎ»ż´Ł»ˇˇˇˇ
6ˇ˘ĆóĘÂҵµĄÎ»±ŘĐëŇŞÇó°ěŔíµÄŁ»
7ˇ˘ĐčŇŞ±¨żĽą«ÎńÔ±ˇ˘ąşÂňĂâË°łµˇ˘Âäת»§żÚˇ˘ÉęÇëÁôѧÉú´´Ňµ»ů˝đˇŁ
ĽÓÄĂ´óÎÄĆľ¶ŕÂ׶඼»á´óѧłÉĽ¨µĄŁ¬TMU±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧ±Ďҵ֤(TMU±Ďҵ֤Ęé)ˇľqޱ1954292140ˇż·ÂÔěÔÚĎßÖĆ×÷±ľżĆÎÄĆľ¶ŕÂ׶඼»á´óѧoffer/ѧλ֤offer°ěŔíˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľö¶ŕÂ׶඼»á´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣
ĽÓÄĂ´óÎÄĆľąşÂňŁ¬ĽÓÄĂ´óÎÄĆľ¶¨ÖĆŁ¬ĽÓÄĂ´óÎÄĆľ˛ą°ěˇŁ×¨ŇµÔÚĎ߶¨ÖĆĽÓÄĂ´ó´óѧÎÄĆľŁ¬¶¨×öĽÓÄô󱾿ĆÎÄĆľŁ¬ˇľqޱ1954292140ˇż¸´ÖĆĽÓÄĂ´óToronto Metropolitan University completion letterˇŁÔÚĎßżěËٲą°ěĽÓÄô󱾿ƱĎҵ֤ˇ˘Ë¶ĘżÎÄĆľÖ¤Ę飬ąşÂňĽÓÄĂ´óѧλ֤ˇ˘¶ŕÂ׶඼»á´óѧOfferŁ¬ĽÓÄĂ´ó´óѧÎÄĆľÔÚĎßąşÂňˇŁ¸ß·ÂŐ滹ԼÓÄĂ´óÎÄĆľÖ¤ĘéşÍÍâżÇŁ¬¶¨ÖĆĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧłÉĽ¨µĄşÍĐŷ⡣ąúÍâ±Ďҵ֤łÉĽ¨µĄµÄ°ěŔíÁ÷łĚTMU±Ďҵ֤ˇľqޱ1954292140ˇż°ěŔíĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧ±Ďҵ֤(TMU±Ďҵ֤Ęé)ˇľqޱ1954292140ˇżŃ§Î»Ö¤Ęéµç×ÓÍĽÔÚĎ߶¨ÖĆ·ţÎń¶ŕÂ׶඼»á´óѧoffer/ѧλ֤ąúÍâѧλČĎÖ¤/±Ďҵ֤ąşÂňˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ˇŁ°ďÄă˝âľö¶ŕÂ׶඼»á´óѧѧŔúѧλČĎÖ¤ÄŃĚ⡣
ĚŘĘâÔŇňµĽÖÂÎŢ·¨±ĎҵŁ¬Ň˛żÉŇÔÁŞĎµÎŇĂÇ°ďÄú°ěŔíĎŕąŘ˛ÄÁĎŁş
Ł±ŁşÔÚ¶ŕÂ׶඼»á´óѧąŇżĆÁËŁ¬˛»Ďë¶ÁÁËŁ¬łÉĽ¨˛»ŔíĎëÔőĂ´°ěŁżŁżŁż
2Łş´ňËă»ŘąúÁËŁ¬ŐŇą¤×÷µÄʱşňŁ¬ĐčŇŞĚáą©ČĎÖ¤ˇ¶TMUłÉĽ¨µĄąşÂň°ěŔí¶ŕÂ׶඼»á´óѧ±Ďҵ֤Ęé·¶±ľˇ·ˇľQ/WeChatŁş1954292140ˇżBuy Toronto Metropolitan University Diplomaˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·ÓĐÎÄƾȴµĂ˛»µ˝ČĎÖ¤ˇŁÓÖ¸ĂÔőĂ´°ěŁżŁżŁżĽÓÄĂ´ó±Ďҵ֤ąşÂňŁ¬ĽÓÄĂ´óÎÄĆľąşÂňŁ¬
3Łş»ŘąúÁËŐŇą¤×÷Ă»ÓжŕÂ׶඼»á´óѧÎÄĆľÔőĂ´°ěŁżÓбľżĆČ´ŇŞÇó˶ʿÓÖÔőĂ´°ěŁż
°ďÄú˝âľöÔÚĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧδ±ĎҵÄŃĚ⣨Toronto Metropolitan UniversityŁ©ÎÄĆľąşÂňˇ˘±Ďҵ֤ąşÂňˇ˘´óѧÎÄĆľąşÂňˇ˘´óѧ±Ďҵ֤ąşÂňˇ˘ÂňÎÄĆľˇ˘ČŐş«ÎÄĆľˇ˘Ó˘ąú´óѧÎÄĆľˇ˘ĂŔąú´óѧÎÄĆľˇ˘°ÄÖŢ´óѧÎÄĆľˇ˘ĽÓÄĂ´ó´óѧÎÄĆľŁ¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧÎÄĆľˇ˘ĐÂÎ÷ŔĽ´óѧÎÄĆľˇ˘°®¶űŔĽÎÄĆľˇ˘Î÷°ŕŃŔÎÄĆľˇ˘µÂąúÎÄĆľˇ˘˝ĚÓý˛żČĎÖ¤Ł¬Âň±Ďҵ֤Ł¬±Ďҵ֤ąşÂňŁ¬Âň´óѧÎÄĆľŁ¬ąşÂňČŐş«±Ďҵ֤ˇ˘Ó˘ąú´óѧ±Ďҵ֤ˇ˘ĂŔąú´óѧ±Ďҵ֤ˇ˘°ÄÖŢ´óѧ±Ďҵ֤ˇ˘ĽÓÄĂ´ó´óѧ±Ďҵ֤Ł¨qޱ1954292140Ł©ĐÂĽÓĆ´óѧ±Ďҵ֤ˇ˘ĐÂÎ÷ŔĽ´óѧ±Ďҵ֤ˇ˘°®¶űŔĽ±Ďҵ֤ˇ˘Î÷°ŕŃŔ±Ďҵ֤ˇ˘µÂąú±Ďҵ֤Ł¬»ŘąúÖ¤Ă÷Ł¬ÁôĐĹÍřČĎÖ¤Ł¬ÁôĐĹČĎÖ¤°ěŔíŁ¬Ń§ŔúČĎÖ¤ˇŁ´Ó¶řÍęłÉľÍҵˇŁ
Ö÷ÓŞĎîÄżŁş
1ˇ˘Őćʵ˝ĚÓý˛żąúÍâѧŔúѧλČĎÖ¤ˇ¶ĽÓÄĂ´ó±ĎҵÎÄĆľÖ¤ĘéżěËŮ°ěŔí¶ŕÂ׶඼»á´óѧѧλ֤Ę鹤ŇŐĎę˝âˇ·ˇľqޱ1954292140ˇżˇ¶ÂŰÎÄĂ»ąý¶ŕÂ׶඼»á´óѧŐýĘ˝łÉĽ¨µĄˇ·Ł¬˝ĚÓý˛ż´ćµµŁ¬˝ĚÓý˛żÁô·ţÍřŐľ100%żÉ˛é.
2ˇ˘°ěŔíTMU±Ďҵ֤Ł¬¸ÄłÉĽ¨µĄˇ¶TMU±Ďҵ֤Ă÷°ěŔí¶ŕÂ׶඼»á´óѧ±Ďҵ֤Ńů±ľˇ·ˇľQ/WeChatŁş1954292140ˇżBuy Toronto Metropolitan University Certificatesˇ¶ŐýĘ˝łÉĽ¨µĄÂŰÎÄĂ»ąýˇ·Ł¬¶ŕÂ׶඼»á´óѧOfferˇ˘ÔÚ¶ÁÖ¤Ă÷ˇ˘Ń§Éúż¨ˇ˘Đŷ⡢֤Ă÷ĐŵČČ«ĚײÄÁĎŁ¬´Ó·Ŕαµ˝ÓˇË˘Ł¬´Óˮӡµ˝¸ÖÓˇĚ̽𣬸߾«·Â¶Č¸úѧУ԰ć100%Ďŕͬ.
3ˇ˘ŐćʵʹąÝČĎÖ¤Ł¨Ľ´ÁôѧČËÔ±»ŘąúÖ¤Ă÷Ł©Ł¬ĘąąÝ´ćµµżÉͨąý´óĘąąÝ˛éŃŻČ·ČĎ.
4ˇ˘ÁôĐĹÍřČĎÖ¤Ł¬ąúĽŇרҵČ˲ĹČĎÖ¤ÖĐĐÄ°ä·˘ČëżâÖ¤Ę飬ÁôĐĹÍř´ćµµżÉ˛é.
ˇ¶¶ŕÂ׶඼»á´óѧłÉĽ¨µĄ·¶±ľĽÓÄĂ´ó±Ďҵ֤Ęé°ěŔíTMU¸´żĚŇ»Ě×ÎÄĆľˇ·ˇľqޱ1954292140ˇżŃ§Î»Ö¤1:1ÍęĂŔ»ąÔşŁÍâ¸÷´óѧ±Ďҵ˛ÄÁĎÉϵŤŇŐŁşË®ÓˇŁ¬ŇőÓ°µ×ÎĆŁ¬¸ÖÓˇLOGOĚĚ˝đĚĚŇřŁ¬LOGOĚĚ˝đĚĚŇř¸´şĎÖصţˇŁÎÄ×ÖÍĽ°¸¸ˇµńˇ˘Ľ¤ąâŔŘÉ䡢×ĎÍâÓ«ąâˇ˘Î¸С˘¸´Óˇ·ŔαµČ·Ŕαą¤ŇŐˇŁ
ˇľqޱ1954292140ˇż°ěŔí¶ŕÂ׶඼»á´óѧ±Ďҵ֤(TMU±Ďҵ֤Ęé)ѧλ֤ĘéµÄÓ˘Îġľqޱ1954292140ˇż¶ŕÂ׶඼»á´óѧoffer/ѧλ֤ˇ˘ÁôĐŹٷ˝Ń§ŔúČĎÖ¤Ł¨ÓŔľĂ´ćµµŐćʵżÉ˛éŁ©˛ÉÓĂѧУ԰ćÖ˝Őš˘ĚŘĘ⹤ŇŐÍęČ«°´ŐŐÔ°ćŇ»±ČŇ»ÖĆ×÷ĽÓÄĂ´ó¶ŕÂ׶඼»á´óѧ±Ďҵ֤(TMU±Ďҵ֤Ęé)łÉĽ¨µĄŃů±ľ
ÁôĐĹČĎÖ¤µÄ×÷ÓĂŁş
1. Éí·ÝČĎÖ¤ŁşÁôĐĹČĎÖ¤żÉŇÔÖ¤Ă÷ÄăµÄÁôѧľŔúĘÇŐćʵµÄŁ¬ÇŇÄă»ńµĂµÄѧŔú»ňѧλĘÇŐýąćÇŇľąýČĎÖ¤µÄˇŁŐâ¶ÔÓÚһЩÓĂČ˵ĄÎ»Ŕ´ËµŁ¬ÓČĆäĘǶÔÁôѧľŔúÓи߶ČŇŞÇóµÄą«ËľŁ¨Čçżçąúą«Ëľ»ňąúÄڸ߶˹«ËľŁ©Ł¬ŐâĘÇ·ÇłŁÖŘŇŞµÄŇ»¸öĆľÖ¤ˇŁ
רҵĆŔ¶¨ŁşÁôĐĹČĎÖ¤˛»˝öČĎÖ¤ÄăµÄѧλ֤Ę飬»ą»á¶ÔÄăµÄËůѧרҵ˝řĐĐĆŔ¶¨ˇŁŐâÓĐÖúÓÚչʾÄăµÄѧĘő±łľ°Ł¬ĚرđĘǶÔÓÚąúÄÚą«Ëľ¶řŃÔŁ¬ÄÜą»ÇĺłţÁË˝âÄăËůѧרҵµÄˮƽşÍĽŰÖµˇŁ
ąúĽŇČ˲ſâČëżâŁşČĎÖ¤şóŁ¬ÄăµÄĐĹϢ˝«±»ÄÉČëąúĽŇČ˲ſ⣬˛˘ÇŇżÉŇÔÔÚąúĽŇČ˲ĹÍřµČƽ̨ÉĎչʾŁ¬ą©°üŔ¨500Çżą«ËľµČ´óĐÍą«ËľĚôѡşÍƸÓĂČ˲šŁŐâ¶ÔÓڻعúŐŇą¤×÷ĚرđĘÇ˝řČë´óą«ËľŁ¬ľßÓĐ·ÇłŁ»ýĽ«µÄ×÷ÓáŁCHEST CT SCAN PRESENTATION FOR NEW RADIOGRAPHERS AND CT SCAN TECHNICIANS .pptx
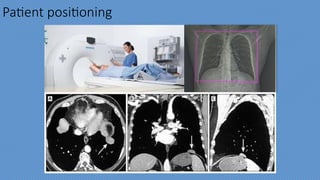
- 1. Chest CT scan Prepared By: RAHMATULLAH SULAIMAN KHAIL
- 2. Indication ? Chest Pain. ? Chest Trauma. ? Infection . ? Intra- thoracic Bleeding. ? Pulmonary embolism. ? Pneumonia . ? Suspected Tumor or mass. ? Assessment of interstitial lung disease. ? Minor fibrosis. ? Pregnancy . ? Hypersensitivity to iodinated contrast media (if contrast is used ). ? Renal failure. ? Heart disorder . Contra Indication
- 3. CT: Single stop Shop Chest ? Lungs ? Heart and great vessels ? Coronary arteries ? Chest wall and bones ? Tracheobronchial tree ? Esophagus ? Mediastinum ? Diaphragm Windows and reconstructions ? MIP (Maximum intensity Projection ? MinIP (minimum intensity projection ? VRT (Volume Rendering Technique ? MPR (Multi planar reformation) ? Soft tissue window ? Lung window ? Bone window
- 5. ? CEST for Routine ? HRCT ? Calcium scoring ? Thoracic CT angiography ? Pulmonary CT angiography ? Coronary CT angiography Overview of Chest CT-protocols
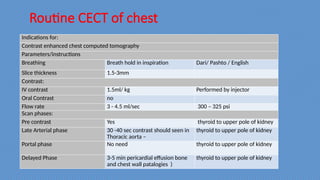
- 6. Routine CECT of chest Indications for: Contrast enhanced chest computed tomography Parameters/instructions Breathing Breath hold in inspiration Dari/ Pashto / English Slice thickness 1.5-3mm Contrast: IV contrast 1.5ml/ kg Performed by injector Oral Contrast no Flow rate 3 - 4.5 ml/sec 300 ¨C 325 psi Scan phases: Pre contrast Yes thyroid to upper pole of kidney Late Arterial phase 30 -40 sec contrast should seen in Thoracic aorta ¨C thyroid to upper pole of kidney Portal phase No need thyroid to upper pole of kidney Delayed Phase 3-5 min pericardial effusion bone and chest wall patalogies ) thyroid to upper pole of kidney
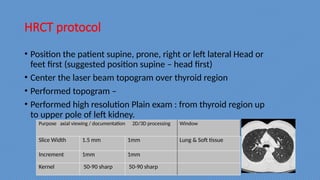
- 7. HRCT protocol Purpose axial viewing / documentation 2D/3D processing Window Slice Width 1.5 mm 1mm Lung & Soft tissue Increment 1mm 1mm Kernel 50-90 sharp 50-90 sharp ? Position the patient supine, prone, right or left lateral Head or feet first (suggested position supine ¨C head first) ? Center the laser beam topogram over thyroid region ? Performed topogram ¨C ? Performed high resolution Plain exam : from thyroid region up to upper pole of left kidney.
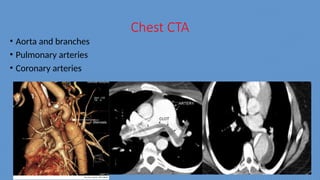
- 8. Chest CTA ? Aorta and branches ? Pulmonary arteries ? Coronary arteries
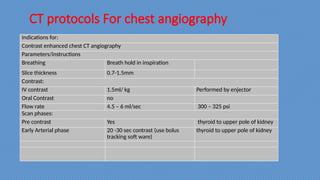
- 9. CT protocols For chest angiography Indications for: Contrast enhanced chest CT angiography Parameters/instructions Breathing Breath hold in inspiration Slice thickness 0.7-1.5mm Contrast: IV contrast 1.5ml/ kg Performed by enjector Oral Contrast no Flow rate 4.5 ¨C 6 ml/sec 300 ¨C 325 psi Scan phases: Pre contrast Yes thyroid to upper pole of kidney Early Arterial phase 20 -30 sec contrast (use bolus tracking soft ware) thyroid to upper pole of kidney
- 10. Bolus tracking soft ware ? The early arterial phase performed approximately 20-30 sec after contrast injection is initiated and is most accurately determine by using bolus tracking software (eg small prep) to monitor the level of contrast enhancement in the aorta and automatically triggering the scan when it reaches a pre determined level of enhancement (eg 120 HU)
- 11. Flow rate
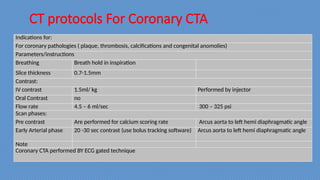
- 12. CT protocols For Coronary CTA Indications for: For coronary pathologies ( plaque, thrombosis, calcifications and congenital anomolies) Parameters/instructions Breathing Breath hold in inspiration Slice thickness 0.7-1.5mm Contrast: IV contrast 1.5ml/ kg Performed by injector Oral Contrast no Flow rate 4.5 ¨C 6 ml/sec 300 ¨C 325 psi Scan phases: Pre contrast Are performed for calcium scoring rate Arcus aorta to left hemi diaphragmatic angle Early Arterial phase 20 -30 sec contrast (use bolus tracking software) Arcus aorta to left hemi diaphragmatic angle Note Coronary CTA performed BY ECG gated technique
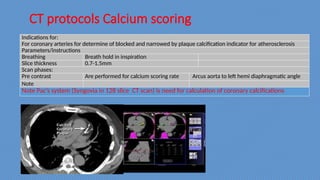
- 13. CT protocols Calcium scoring Indications for: For coronary arteries for determine of blocked and narrowed by plaque calcification indicator for atherosclerosis Parameters/instructions Breathing Breath hold in inspiration Slice thickness 0.7-1.5mm Scan phases: Pre contrast Are performed for calcium scoring rate Arcus aorta to left hemi diaphragmatic angle Note Note PacˇŻs system (Syngovia in 128 slice CT scan) is need for calculation of coronary calcifications
- 14. ECG Gated
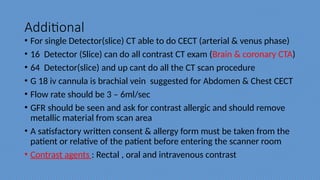
- 15. Additional ? For single Detector(slice) CT able to do CECT (arterial & venus phase) ? 16 Detector (Slice) can do all contrast CT exam (Brain & coronary CTA) ? 64 Detector(slice) and up cant do all the CT scan procedure ? G 18 iv cannula is brachial vein suggested for Abdomen & Chest CECT ? Flow rate should be 3 ¨C 6ml/sec ? GFR should be seen and ask for contrast allergic and should remove metallic material from scan area ? A satisfactory written consent & allergy form must be taken from the patient or relative of the patient before entering the scanner room ? Contrast agents : Rectal , oral and intravenous contrast
- 16. Thanks
Editor's Notes
- #8: Picture for pdaˇˇ