




























































More Related Content
Similar to TRIPLE PHASE CT TECHNIQUE for ct scan technicians .pdf (20)
More from MMCRADIOLOGY1 (8)






Recently uploaded (20)




















TRIPLE PHASE CT TECHNIQUE for ct scan technicians .pdf
- 2. The AFGHANISTAN RADIOGRAPHERS SOCIETY (ARS) is a non- profit organization, set up by professional societies that represent radiographers in the geographic continent Afghanistan. The role of the ARS is to represent, promote and develop the profession of radiographers in Afghanistan, within the whole range of medical imaging, nuclear medicine and radiotherapy. Over ons
- 3. The Triple phase CT scan of the abdomen is a screening test for carcinoma in the abdominal cavity. Use for early disease detection. This is the most accurate test available for detecting Hepatocellular carcinoma pancreatic cancer as well as problems in the kidneys, spleen, adrenal glands, gall bladder and abdominal lymph nodes. INTRODUCTION
- 4. Largest internal organ and largest gland Lies under diaphragm in the right upper abdomen and mid abdomen and extend into left upper abdomen Shape- wedge , base to right, apex to left Extension- from 5th ICS the Rt MCL down to costal margin Measurement-12-15cms coronally and 15-20 cms transversely Weight- 1800gms in males, 1400gms in females INTRODUCTION TO LIVER
- 6. LOBES OF LIVER ’é¦ Liver is divided into right and left lobes by falciform ligament. ’é¦ The right lobe also has two miner lobes ’é¦ Caudate lobe ’é¦ Quadrate lobe
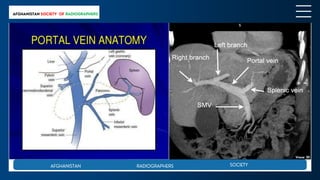
- 20. RADIOLOGICAL ANATOMY OF LIVER IN CT
- 25. ’āś Pre-contrast ŌĆō deferred in follow up/ metastasis ’āś Arterial phase of contrast enhancement ’āśPortal phase of contrast enhancement ’āśVenous phase ŌĆō equilibrium ’āśAbdominal CT completed to iliac crest level ’āś haemangioma suspected-additional delayed images to assess for filling of haemangioma TECHNIQUE
- 26. ŌĆó Non-ionic contrast ŌĆó Serum creatinine ŌĆó EGFR-estimated glomerular filtration rate ŌĆó Contrast dose- 1.5 r 2 ml/kg max 150 ml ŌĆó Rate of injection- 4 ml/sec at 300psi ŌĆó Iv cannula-18 -20 Gage ŌĆó Multislice CT- reduce contrast dose REQUIRMENTS
- 27. Consent: ’ü«Empty stomach -fasting for 6 hrs. ’ü«Previous intravenous contrast injections? ’ü«Any side effects or reaction due to contrast media? ’ü«Diabetic? ’ü«Renal abnormalities? ’ü«Periods allergies? ’ü« Thyroid abnormalities? ’ü«Pregnancy or breast feeding? ’ü«Any medication using? ’ü«Dialysis?
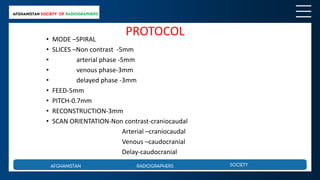
- 28. PROTOCOL ŌĆó MODE ŌĆōSPIRAL ŌĆó SLICES ŌĆōNon contrast -5mm ŌĆó arterial phase -5mm ŌĆó venous phase-3mm ŌĆó delayed phase -3mm ŌĆó FEED-5mm ŌĆó PITCH-0.7mm ŌĆó RECONSTRUCTION-3mm ŌĆó SCAN ORIENTATION-Non contrast-craniocaudal Arterial ŌĆōcraniocaudal Venous ŌĆōcaudocranial Delay-caudocranial
- 29. PROTOCOL ŌĆó TIMING OF SCAN---ARTERIAL ŌĆō bolus tracking 18 -25 sec PORTAL -45 sec VENOUS -65 sec DELAY-5 MIN ŌĆó COLLIMATION-- spatial resolution /image noise ŌĆó TABLE SPEED --- 15 MM/rotation ŌĆó Kvp/mAs ---120/225 ŌĆó FOV ----- 350mm ŌĆó FILTERS-B30S MEDIUM SMOOOTH ŌĆó High quality , large volume, reasonable radiation dose to obtain 3D multiplanar images in single breath hold
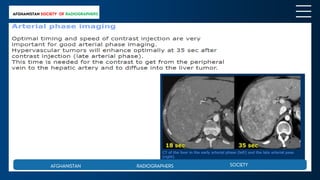
- 30. ARTERIAL PHASE scan during injection : arterial phase ,highlight the lesions in or around the artery leading into the liver ŌĆó Arterial phase of scanning method- performed approximately 30 secs after the contrast injection is initiated and is most accurately determined by using bolus tracking software (eg Smart prep) to monitor the level of contrast enhancement in the aorta and automatically triggering the scan when it reaches a predetermined level of enhancement (eg 120 HU) ŌĆó 5mm-post contrast-top to bottom of liver for arterial phase ,2.5mm recon ŌĆó Excellent hepatic arterial opacification with minimally contrast in portal vein.
- 31. ŌĆó Hypervascular lesions like HCC, Focal nodular hyperplasia, Adenoma, haemangioma enhance during the arterial phase and appear hyperdense ŌĆó Arterial phase images are also used for pre operative evaluation of arterial vasculature through the use of MIPs and 3D reconstructions
- 32. ŌĆó Early arterial phase: 15-20 sec or immediately after bolus ŌĆó Late arterial phase: 35-40 sec or 20 sec after bolus ŌĆó Demarcation of vessels enhancement of hypervascular- elisions, stomach ŌĆó Normal parenchyma is supplied for 80% by portal vein and only for 20 % by hepatic artery ŌĆó Normal parenchyma will enhance maximally in the hepatic venous phase at 65-75 sec and only a little bit in the late arterial phase 18-35 secs
- 34. ’āśScan during injection or shortly after : ’āś portal venous phase, show lesions in or around the portal vein ’āśPortal venous phase performed 70-90 secs post contrast and hypovascular lesions appear hypodense and hypervascular lesions appears isodense (same density as surrounding liver) ’āśSCAN METHOD- 5mm with 2.5 mm recon 80 sec delay , scan the entire abdomen in this acquisition (top of liver to spleen) ’āśHypovascular lesions like- metastasis , cysts and abscesses ’āśHypovascular mets- colon PORTAL VENOUS PHASE
- 36. ŌĆó Delayed scan after injection : allow soft tissue to absorb contrast and highlights changes in tissues ŌĆó Delayed scan through kidney at 3mins ŌĆó Delayed phase performed 5-10 mins post contrast and used to characterise the lesions ŌĆó hemangiomas slow to enhance and some HCC appear hypodense due to washout ŌĆó SCAN METHOD- 5mm with 2.5 recon 3mins from injection (top of liver to bottom of kidneys) DELAYED PHASE
- 37. ŌĆó ENHANCEMENT OF- fibrotic lesions, still enhancement of kidney and urinary collecting system ŌĆó DETECTION OF ŌĆō liver cholangiocarcinoma, ŌĆó fibrotic mets, kidney- TCC