Los tumores del estroma gastrointestinal (GIST) son tumores poco frecuentes del tracto gastrointestinal. Pertenecen al grupo de los sarcomas y representan menos del 3% de las neoplasias gastrointestinales. Los GIST se caracterizan por la expresiÃģn de la proteÃna CD117 y generalmente son exofÃticos y bien delimitados cuando se observan mediante tomografÃa computarizada. El tratamiento para GIST no resecables, recurrentes o metastÃĄsicos incluye el uso de imatinib u otros inhibidores de tirosina kinasa.
Este documento describe los tumores del estroma gastrointestinal (GIST), los cuales se originan de las cÃĐlulas madre que se diferencian a cÃĐlulas intersticiales de Cajal. Los GIST representan el 2% de los tumores gastrointestinales y ocurren con mÃĄs frecuencia entre las 4a y 6a dÃĐcadas de vida. El diagnÃģstico se realiza mediante biopsia e inmunohistoquÃmica para marcadores como CD117. El tratamiento principal es la resecciÃģn quirÚrgica completa, aunque tambiÃĐn existen opciones de tratamiento mÃĐdico con inhibidores de
Los tumores del estroma gastrointestinal (GIST) son sarcomas poco comunes que se originan de las cÃĐlulas marcapaso en la pared del tracto gastrointestinal. Se caracterizan por ser tumores submucosos que expresan la proteÃna KIT. El tratamiento para GIST localizado es la cirugÃa, mientras que para GIST metastÃĄsico o localmente avanzado la opciÃģn es el tratamiento con imatinib, un inhibidor de la tirosina quinasa del receptor KIT. La supervivencia de pacientes con GIST ha mejorado significativamente con el descubrimiento e implementaciÃģn del
O documento discute o tumor estromal gastrointestinal (GIST), incluindo sua localizaçÃĢo, causas, sintomas, diagnÃģstico e tratamentos. O GIST começa nas cÃĐlulas do sistema nervoso que regulam a digestÃĢo e pode ocorrer em qualquer parte do trato gastrointestinal. Os principais tratamentos incluem cirurgia para remover o tumor, terapia alvo com medicamentos e estudos de novos tratamentos.
Gastrointestinal stromal tumor (GIST) dr ridu kumar sharmaRidu Kumar Sharma
Ėý
GISTs are the most common mesenchymal tumors of the GI tract. They are driven by mutations in c-Kit and PDGFR genes. Surgery is the main treatment for localized disease, while imatinib is effective systemic therapy for advanced or metastatic GISTs. Imatinib targets the c-Kit mutation to inhibit tumor growth with acceptable toxicity. Tumor size and mitotic index are prognostic factors used for risk stratification. Ongoing research is exploring additional targeted therapies to treat GISTs.
Gastrointestinal stromal tumors (GISTs) arise from interstitial cells of Cajal in the gastrointestinal tract. Pathogenic mutations in KIT or PDGFRA genes drive tumor growth in most GISTs. GISTs most commonly occur in the stomach and small intestine. Microscopically, GISTs demonstrate spindle or epithelioid cell morphologies and strongly express KIT (CD117). Surgical resection is the primary treatment, while the tyrosine kinase inhibitor imatinib is effective for advanced or metastatic disease. Tumor size, mitotic rate, and site determine prognosis, with small intestinal GISTs having the worst outcomes.
Gastrointestinal stromal tumors (GISTs) are rare mesenchymal tumors that arise from interstitial cells of Cajal in the gastrointestinal tract. GISTs most commonly present in the stomach and small intestine in patients in their late 60s, and median size is 5 cm. While small GISTs are often asymptomatic, larger tumors can cause vague symptoms like abdominal pain or bleeding. Diagnosis involves biopsy or excision of nodules over 2 cm. Immunohistochemistry shows 95% of GISTs are positive for CD117. Prognosis depends on tumor size, mitotic rate, and location. Treatment involves surgery for resectable localized disease and imatinib for advanced or metastatic
Los GISTomas son tumores del estroma gastrointestinal que ocurren a lo largo del tracto digestivo. Se presentan principalmente en el estÃģmago y pueden causar hemorragia, dolor abdominal u obstrucciÃģn. Son neoplasias mesenquimatosas submucosas que se originan en las cÃĐlulas intersticiales de Cajal. Su diagnÃģstico se realiza mediante estudios de imagen como la tomografÃa computarizada.
The document discusses a case of a 46-year-old female with gastrointestinal stromal tumors (GIST), emphasizing the rarity of GIST and the significance of c-kit mutations in treatment. Surgical resection is highlighted as the first-line approach for resectable GIST, while imatinib mesylate is the standard treatment for unresectable or metastatic cases. The document also outlines treatment protocols and outcomes for adjuvant and neoadjuvant therapies.
Presentation1, radiological imaging of gastro intestinal stromal tumour(gist).Abdellah Nazeer
Ėý
This document summarizes radiological imaging of gastrointestinal stromal tumors (GISTs). It describes GISTs as the most common mesenchymal tumors of the GI tract, occurring most often in older adults. Imaging findings are discussed for various modalities including CT, MRI, US, and PET. Characteristic features include soft tissue masses arising from the GI tract wall. Larger tumors may show necrosis, hemorrhage, or cystic changes. Imaging can also detect metastatic lesions or tumor response to chemotherapy.
Gastrointestinal stromal tumors (GISTs) are rare tumors that originate from the gastrointestinal tract. They most commonly occur in the stomach. Surgical resection is the primary treatment, but molecular targeted therapy with imatinib is also used in advanced or unresectable cases. Imatinib has improved outcomes by reducing recurrence rates after surgery or controlling tumor growth. Ongoing clinical trials are further evaluating the neoadjuvant and adjuvant uses of imatinib to improve prognosis.
Presentation1, radiological imaging of anal carcinoma.Abdellah Nazeer
Ėý
1) MRI is the preferred imaging modality for staging anal carcinoma due to its ability to accurately assess the size and extent of primary tumors as well as lymph node involvement.
2) Anal carcinoma is typically staged according to tumor size (T-stage), lymph node involvement (N-stage), and presence of distant metastases (M-stage). MRI allows for evaluation of these factors.
3) Additional imaging with PET/CT may be used to detect distant metastases and better define lymph node involvement, potentially changing staging in 20% of cases and treatment planning in 3-5% of cases.
Caso clÃnico tumor del estroma gastrointestinal- dr juradoMelissa Solis
Ėý
Este caso clÃnico describe el restablecimiento del trÃĄnsito gastrointestinal de un paciente de 21 aÃąos que previamente habÃa sufrido una exerÃĐsis de tumor pÃĐlvico y colostomÃa. El paciente fue sometido a una cirugÃa para restablecer la continuidad intestinal y cerrar la colostomÃa mediante una anastomosis terminoterminal. PresentÃģ complicaciones postoperatorias como infecciÃģn de herida quirÚrgica que requiriÃģ tratamiento antibiÃģtico. Finalmente evolucionÃģ de manera satisfactoria.
Este documento resume informaciÃģn sobre tumores del estroma gastrointestinal. Estos tumores se originan de cÃĐlulas precursoras como las cÃĐlulas intestinales de Cajal y cÃĐlulas musculares lisas. Generalmente son tratados quirÚrgicamente y con imatinib como terapia adyuvante o para enfermedad avanzada. La resistencia a imatinib puede tratarse con sunitinib u otras opciones.
The document discusses several studies by Dubecz et al. on trends in adenocarcinoma (adeno-CA) incidence and esophageal cancer (EC) cure and resection rates in the modern era. It notes increasing adeno-CA incidence rates over time, higher rates in white men, stage-by-stage incidence data, and modern cure rates for localized and regional EC from resection. Resection rates for non-metastatic EC in the US are presented from several data sources, along with median lymph nodes removed and percentage of patients with adequate lymph node dissection.
Stent Presentation at STS 2009 San franciscodubeczattila
Ėý
This study evaluated the use of self-expanding metal stents, plastic stents, and hybrid stents to treat 133 patients with malignant and benign esophageal diseases over an 8-year period at a single institution. Stent placement was successful in relieving obstruction in 91% of patients with a median hospital stay of 1 day. Complications included migration in 9.7% of cases, impaction in 13% requiring endoscopic disimpaction, and tumor ingrowth in 5.2% of uncovered metal stents. Stent placement was found to be a generally safe, quick, and reliable procedure for palliating malignant esophageal obstructions.
High resolution manometry (HRM) can provide useful functional information for evaluating patients experiencing recurrent symptoms after failed fundoplication surgery. The study evaluated 28 patients with various symptoms using HRM and compared results to healthy controls. HRM revealed high residual lower esophageal sphincter pressures, low rates of LES relaxation, and high intrabolus pressures in the neo-high pressure zone for most patients experiencing post-fundoplication dysphagia. HRM allows detailed analysis of complex esophageal pathology to provide insight for clinical decision making.
High Resolution Manometry Introduction2dubeczattila
Ėý
High-resolution manometry uses a catheter with 36 solid-state pressure sensors spaced 1 cm apart to measure esophageal motility. It provides 2D and 3D spatial-temporal plots of pressure data along the esophagus. Classic achalasia shows no peristalsis and impaired lower esophageal sphincter relaxation, while other primary motility disorders like jackhammer esophagus have high amplitude contractions over 180 mmHg with double peaks and prolonged contractions over 6 seconds. HRM allows diagnosis of different motility disorders based on patterns of peristalsis, LES relaxation, and contraction amplitudes.
Der Fallbericht beschreibt eine 49-jÃĪhrige Patientin, die nach einer laparoskopischen Cholezystektomie mit einer intraabdominellen Blutung und darauf folgender Reoperation aufgrund eines Pseudoaneurysmas des Arteria cystica konfrontiert war. Nach der Behandlung und Entfernung des Pseudoaneurysmas verlief der post-operative Verlauf unauffÃĪllig, und die Patientin wurde schlieÃlich beschwerdefrei entlassen. Hemobilie stellt eine seltene Komplikation nach Cholezystektomie dar, die gegebenenfalls einen chirurgischen Eingriff erforderlich macht, wenn die interventionelle Therapie nicht mÃķglich ist.
Gallengangverletzungen Nach Cholezystektomie 2007 ÃķCk Graz Finaldubeczattila
Ėý
Die Studie beleuchtet die Rate von Gallengangsverletzungen nach Cholezystektomie mit einer HÃĪufigkeit von 1,6% bei 2850 untersuchten Operationen. Es wird diskutiert, dass visuelle Illusionen und der Schwierigkeitsgrad der Operationen hÃĪufige Fehlerursachen sind und dass intraoperative Cholangiographie als prÃĪventive Strategie dienen kann. Auch wenn die Raten konstant bleiben, ist eine Verbesserung der chirurgischen Techniken notwendig, um diese Komplikationen zu verringern.
This document provides an overview of essentials for manuscript review, including how to organize a manuscript, use statistics, identify types of studies and levels of evidence, address bias, interpret results, and write an abstract, introduction, methods, discussion, and conclusion. It discusses key aspects of each section and how to effectively review a submitted manuscript.
This document describes the steps of a surgical procedure involving the duodenum, pancreas, stomach, and other abdominal organs. Key steps include:
1) Kocherization to mobilize the duodenum and expose surrounding structures.
2) Bursectomy and dissection of surrounding tissues to further expose vessels.
3) Division of vessels including the right gastric and gastroduodenal arteries.
4) Transection of the duodenum and dissection of the pancreas and surrounding lymph nodes.
5) Distal pancreatectomy and esophagojejunostomy to reconstruct the digestive tract.
Das Dokument behandelt die Appendizitis, einschlieÃlich Anatomie, Epidemiologie, Ãtiologie und Diagnostik. Es hebt die Inzidenz, Risikofaktoren, pathologische Befunde sowie die Diagnostik und TherapiemÃķglichkeiten hervor. AuÃerdem werden Komplikationen und die Herausforderungen bei der Diagnose und Behandlung der Krankheit beschrieben.
Gastrointestinal stromal tumor (GIST) dr ridu kumar sharmaRidu Kumar Sharma
Ėý
GISTs are the most common mesenchymal tumors of the GI tract. They are driven by mutations in c-Kit and PDGFR genes. Surgery is the main treatment for localized disease, while imatinib is effective systemic therapy for advanced or metastatic GISTs. Imatinib targets the c-Kit mutation to inhibit tumor growth with acceptable toxicity. Tumor size and mitotic index are prognostic factors used for risk stratification. Ongoing research is exploring additional targeted therapies to treat GISTs.
Gastrointestinal stromal tumors (GISTs) arise from interstitial cells of Cajal in the gastrointestinal tract. Pathogenic mutations in KIT or PDGFRA genes drive tumor growth in most GISTs. GISTs most commonly occur in the stomach and small intestine. Microscopically, GISTs demonstrate spindle or epithelioid cell morphologies and strongly express KIT (CD117). Surgical resection is the primary treatment, while the tyrosine kinase inhibitor imatinib is effective for advanced or metastatic disease. Tumor size, mitotic rate, and site determine prognosis, with small intestinal GISTs having the worst outcomes.
Gastrointestinal stromal tumors (GISTs) are rare mesenchymal tumors that arise from interstitial cells of Cajal in the gastrointestinal tract. GISTs most commonly present in the stomach and small intestine in patients in their late 60s, and median size is 5 cm. While small GISTs are often asymptomatic, larger tumors can cause vague symptoms like abdominal pain or bleeding. Diagnosis involves biopsy or excision of nodules over 2 cm. Immunohistochemistry shows 95% of GISTs are positive for CD117. Prognosis depends on tumor size, mitotic rate, and location. Treatment involves surgery for resectable localized disease and imatinib for advanced or metastatic
Los GISTomas son tumores del estroma gastrointestinal que ocurren a lo largo del tracto digestivo. Se presentan principalmente en el estÃģmago y pueden causar hemorragia, dolor abdominal u obstrucciÃģn. Son neoplasias mesenquimatosas submucosas que se originan en las cÃĐlulas intersticiales de Cajal. Su diagnÃģstico se realiza mediante estudios de imagen como la tomografÃa computarizada.
The document discusses a case of a 46-year-old female with gastrointestinal stromal tumors (GIST), emphasizing the rarity of GIST and the significance of c-kit mutations in treatment. Surgical resection is highlighted as the first-line approach for resectable GIST, while imatinib mesylate is the standard treatment for unresectable or metastatic cases. The document also outlines treatment protocols and outcomes for adjuvant and neoadjuvant therapies.
Presentation1, radiological imaging of gastro intestinal stromal tumour(gist).Abdellah Nazeer
Ėý
This document summarizes radiological imaging of gastrointestinal stromal tumors (GISTs). It describes GISTs as the most common mesenchymal tumors of the GI tract, occurring most often in older adults. Imaging findings are discussed for various modalities including CT, MRI, US, and PET. Characteristic features include soft tissue masses arising from the GI tract wall. Larger tumors may show necrosis, hemorrhage, or cystic changes. Imaging can also detect metastatic lesions or tumor response to chemotherapy.
Gastrointestinal stromal tumors (GISTs) are rare tumors that originate from the gastrointestinal tract. They most commonly occur in the stomach. Surgical resection is the primary treatment, but molecular targeted therapy with imatinib is also used in advanced or unresectable cases. Imatinib has improved outcomes by reducing recurrence rates after surgery or controlling tumor growth. Ongoing clinical trials are further evaluating the neoadjuvant and adjuvant uses of imatinib to improve prognosis.
Presentation1, radiological imaging of anal carcinoma.Abdellah Nazeer
Ėý
1) MRI is the preferred imaging modality for staging anal carcinoma due to its ability to accurately assess the size and extent of primary tumors as well as lymph node involvement.
2) Anal carcinoma is typically staged according to tumor size (T-stage), lymph node involvement (N-stage), and presence of distant metastases (M-stage). MRI allows for evaluation of these factors.
3) Additional imaging with PET/CT may be used to detect distant metastases and better define lymph node involvement, potentially changing staging in 20% of cases and treatment planning in 3-5% of cases.
Caso clÃnico tumor del estroma gastrointestinal- dr juradoMelissa Solis
Ėý
Este caso clÃnico describe el restablecimiento del trÃĄnsito gastrointestinal de un paciente de 21 aÃąos que previamente habÃa sufrido una exerÃĐsis de tumor pÃĐlvico y colostomÃa. El paciente fue sometido a una cirugÃa para restablecer la continuidad intestinal y cerrar la colostomÃa mediante una anastomosis terminoterminal. PresentÃģ complicaciones postoperatorias como infecciÃģn de herida quirÚrgica que requiriÃģ tratamiento antibiÃģtico. Finalmente evolucionÃģ de manera satisfactoria.
Este documento resume informaciÃģn sobre tumores del estroma gastrointestinal. Estos tumores se originan de cÃĐlulas precursoras como las cÃĐlulas intestinales de Cajal y cÃĐlulas musculares lisas. Generalmente son tratados quirÚrgicamente y con imatinib como terapia adyuvante o para enfermedad avanzada. La resistencia a imatinib puede tratarse con sunitinib u otras opciones.
The document discusses several studies by Dubecz et al. on trends in adenocarcinoma (adeno-CA) incidence and esophageal cancer (EC) cure and resection rates in the modern era. It notes increasing adeno-CA incidence rates over time, higher rates in white men, stage-by-stage incidence data, and modern cure rates for localized and regional EC from resection. Resection rates for non-metastatic EC in the US are presented from several data sources, along with median lymph nodes removed and percentage of patients with adequate lymph node dissection.
Stent Presentation at STS 2009 San franciscodubeczattila
Ėý
This study evaluated the use of self-expanding metal stents, plastic stents, and hybrid stents to treat 133 patients with malignant and benign esophageal diseases over an 8-year period at a single institution. Stent placement was successful in relieving obstruction in 91% of patients with a median hospital stay of 1 day. Complications included migration in 9.7% of cases, impaction in 13% requiring endoscopic disimpaction, and tumor ingrowth in 5.2% of uncovered metal stents. Stent placement was found to be a generally safe, quick, and reliable procedure for palliating malignant esophageal obstructions.
High resolution manometry (HRM) can provide useful functional information for evaluating patients experiencing recurrent symptoms after failed fundoplication surgery. The study evaluated 28 patients with various symptoms using HRM and compared results to healthy controls. HRM revealed high residual lower esophageal sphincter pressures, low rates of LES relaxation, and high intrabolus pressures in the neo-high pressure zone for most patients experiencing post-fundoplication dysphagia. HRM allows detailed analysis of complex esophageal pathology to provide insight for clinical decision making.
High Resolution Manometry Introduction2dubeczattila
Ėý
High-resolution manometry uses a catheter with 36 solid-state pressure sensors spaced 1 cm apart to measure esophageal motility. It provides 2D and 3D spatial-temporal plots of pressure data along the esophagus. Classic achalasia shows no peristalsis and impaired lower esophageal sphincter relaxation, while other primary motility disorders like jackhammer esophagus have high amplitude contractions over 180 mmHg with double peaks and prolonged contractions over 6 seconds. HRM allows diagnosis of different motility disorders based on patterns of peristalsis, LES relaxation, and contraction amplitudes.
Der Fallbericht beschreibt eine 49-jÃĪhrige Patientin, die nach einer laparoskopischen Cholezystektomie mit einer intraabdominellen Blutung und darauf folgender Reoperation aufgrund eines Pseudoaneurysmas des Arteria cystica konfrontiert war. Nach der Behandlung und Entfernung des Pseudoaneurysmas verlief der post-operative Verlauf unauffÃĪllig, und die Patientin wurde schlieÃlich beschwerdefrei entlassen. Hemobilie stellt eine seltene Komplikation nach Cholezystektomie dar, die gegebenenfalls einen chirurgischen Eingriff erforderlich macht, wenn die interventionelle Therapie nicht mÃķglich ist.
Gallengangverletzungen Nach Cholezystektomie 2007 ÃķCk Graz Finaldubeczattila
Ėý
Die Studie beleuchtet die Rate von Gallengangsverletzungen nach Cholezystektomie mit einer HÃĪufigkeit von 1,6% bei 2850 untersuchten Operationen. Es wird diskutiert, dass visuelle Illusionen und der Schwierigkeitsgrad der Operationen hÃĪufige Fehlerursachen sind und dass intraoperative Cholangiographie als prÃĪventive Strategie dienen kann. Auch wenn die Raten konstant bleiben, ist eine Verbesserung der chirurgischen Techniken notwendig, um diese Komplikationen zu verringern.
This document provides an overview of essentials for manuscript review, including how to organize a manuscript, use statistics, identify types of studies and levels of evidence, address bias, interpret results, and write an abstract, introduction, methods, discussion, and conclusion. It discusses key aspects of each section and how to effectively review a submitted manuscript.
This document describes the steps of a surgical procedure involving the duodenum, pancreas, stomach, and other abdominal organs. Key steps include:
1) Kocherization to mobilize the duodenum and expose surrounding structures.
2) Bursectomy and dissection of surrounding tissues to further expose vessels.
3) Division of vessels including the right gastric and gastroduodenal arteries.
4) Transection of the duodenum and dissection of the pancreas and surrounding lymph nodes.
5) Distal pancreatectomy and esophagojejunostomy to reconstruct the digestive tract.
Das Dokument behandelt die Appendizitis, einschlieÃlich Anatomie, Epidemiologie, Ãtiologie und Diagnostik. Es hebt die Inzidenz, Risikofaktoren, pathologische Befunde sowie die Diagnostik und TherapiemÃķglichkeiten hervor. AuÃerdem werden Komplikationen und die Herausforderungen bei der Diagnose und Behandlung der Krankheit beschrieben.
A 29-year-old woman had been chronically treated for Crohn's disease for years based on a biopsy suggesting a mild case. However, during a surgery, a retained surgical sponge was discovered in her small intestine that had been there since a previous surgery, causing her symptoms. A review of previous samples found threads from the sponge. It is believed the sponge had migrated through her intestines without causing an open wound. Her true diagnosis was misdiagnosed Crohn's disease due to the retained foreign body.
The document summarizes WHO's perspective on proposed reforms to Hungary's health insurance system. The WHO has two main concerns: 1) There is no logical link between the problems identified in Hungary's system and the solution of introducing competitive private health insurance. 2) Analyzing the system using labels like "Beveridge" and "Bismarck" is outdated and misleading. The WHO believes the reforms will greatly increase costs without clear benefits and that Hungary should learn from countries with similar systems rather than those proposed as models.
1. Gastro i ntestinal is Stromal is Tumor ok Dr.Dubecz Attila SE SebÃĐszeti TanszÃĐk â FÅvÃĄrosi ÃnkormÃĄnyzat Szent IstvÃĄn KÃģrhÃĄz SebÃĐszeti OsztÃĄly SebÃĐszeti TovÃĄbbkÃĐpzÅ ElÅadÃĄs 200 6 mÃĄjus 24.
2. A GI traktus leggyakoribb non-epithelialis ( mesench y mal is/ s tromal is ) tumor ai GIST fogalma: Mazur ÃĐs C lark (1983) Mazur MT , Clark HB Gastric stromal tumors. Reappraisal of histogenesis. Am J Surg Pathol. 1983 Sep;7(6):507-19. GIST: TerminolÃģgia
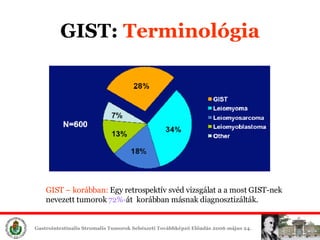
3. GIST: TerminolÃģgia GIST â korÃĄbban: Egy retrospektÃv svÃĐd vizsgÃĄlat a a most GIST-nek nevezett tumorok 72%- ÃĄt korÃĄbban mÃĄsnak diagnosztizÃĄltÃĄk.
4. GIST : EpidemiolÃģgia Incidencia: 1,5-2 / 100.000 lakos Median koreloszlÃĄs: 55-65 ÃĐv Leggyakoribb benignus GI daganat Leggyakoribb mesenchymalis GI daganat A prim er GI rÃĄkok 0, 1 -3,5 % -ÃĄt teszik ki 1.adeocc, 2. lymphoma 3.GIST Ffi>nÅ 1,5x
6. GIST: ąĘēđģŲīĮąôÃģēĩūąēđ GIST: mÃĄs daganatos betegsÃĐgekhez is tÃĄrsulhat A betegek 10-18%-ÃĄnÃĄl mÃĄsodik, harmadik daganat Carney-triÃĄsz : GIST & extra-adrenal paraganglionoma, tÞdÅ-chondroma Carney JA (1999) Neurofibromatosis (Recklinghausen) GenotÃpus: NF1
7. GIST: ąĘēđģŲīĮąôÃģēĩūąēđ 1986 -ban egy retrov à rus t ( HZ4-FeSV) izolÃĄltÃĄk macska fibrosarcom ÃĄbÃģl A HZ4-FeSV v iral is genom ja egy Új on k o gÃĐ n t tartalmazott: ez a v-kit A v-kit c ellular is megfelelÅje: c -kit A c-kit egy 145 kD transmembrÃĄn t i ro zin- kin ÃĄzt / receptor t kÃģdol: ez a KIT Nature 1988 Sep 1;335(6185):88-9
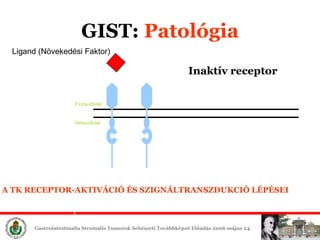
9. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ Extracellular Intracellular Ligand (NÃķvekedÃĐsi Faktor) Ina k t Ãv r eceptor A TK RECEPTOR-AKTIVÃCIà ÃS SZIGNÃLTRANSZDUKCIà LÃPÃSEI
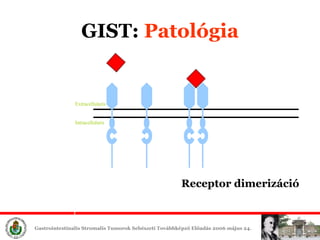
10. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ Ligand Extracellular is Intracellular is Receptor d imeriz ÃĄciÃģ
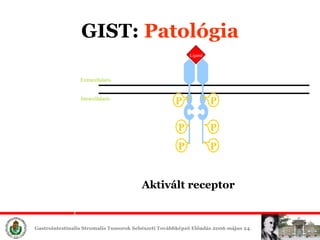
11. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ P P P P P P Extracellular is Intracellular is Receptor a uto- f os zf or i l ÃĄciÃģ ÃĐs aktivÃĄciÃģ
12. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ P P P P P P Extracellular is Intracellular is Ligand AktivÃĄlt receptor
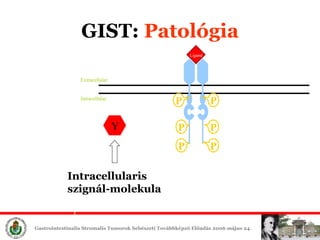
13. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ P P P P P P Extracellular Intracellular Ligand Y Intracellular is szignÃĄl-molekula
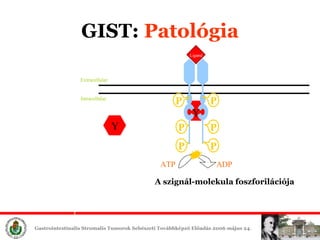
14. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ P P P P P P Extracellular Intracellular Ligand ATP ADP Y Y A szignÃĄl-molekula f os zforilÃĄciÃģja
15. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ P P P P P P Extracellular is Intracellular is P Ligand ATP ADP Y Y Y A szignÃĄl-molekula aktivÃĄciÃģja ÃĐs a jel-kaszkÃĄd beindulÃĄsa
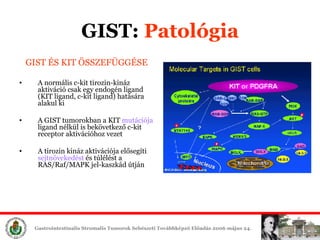
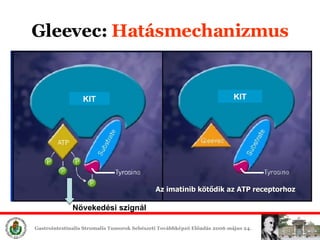
16. GIST: ąĘēđģŲīĮąôÃģēĩūąēđ GIST ÃS KIT ÃSSZEFÃGGÃSE A n orm ÃĄ l is c-kit t irozin-kinÃĄz aktivÃĄciÃģ csak egy endog ÃĐn ligand (KIT ligand, c-kit ligand) hatÃĄsÃĄra alakul ki A GIST tumorokban a KIT mutÃĄciÃģja ligand nÃĐlkÞl is bekÃķvetkezÅ c-kit receptor aktivÃĄciÃģhoz vezet A tirozin kinÃĄz aktivÃĄciÃģja elÅsegÃti sejtnÃķvekedÃĐst ÃĐs tÚlÃĐlÃĐst a RAS/Raf/MAPK jel-kaszkÃĄd ÚtjÃĄn
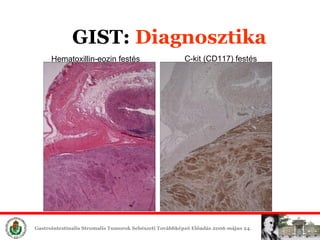
17. GIST: ąĘēđģŲīĮąôÃģēĩūąēđ GIST ÃS KIT ÃSSZEFÃGGÃSE CD117 antig ÃĐ n t majdnem az Ãķsszes GIST expresszÃĄlja szemben a GI traktus tÃķbbi tumorÃĄval A GIST -ekben a c -kit aktivÃĄciÃģ kb.80%-ban egy aktivÃĄlÃģ hatÃĄsÚ (gain-of-function) KIT gÃĐn mut ÃĄciÃģ eredmÃĐnye A GIST diagnÃģzisa a CD117 antigÃĐn immunhisztokÃĐmiai kimutatÃĄsÃĄn alapul
18. GIST: ąĘēđģŲīĮąôÃģēĩūąēđ GIST ÃS KIT ÃSSZEFÃGGÃSE A KIT szerepet jÃĄtszik: Hematopoesis Melanogenesis Cajal-f. interstitialis sejtek differentÃĄciÃģjÃĄban GI simaizomba beÃĄgyazva KIT+ sejtek hÃĄlÃģzata â Pacemaker â funkciÃģ
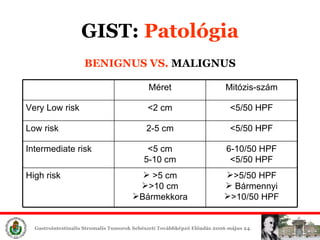
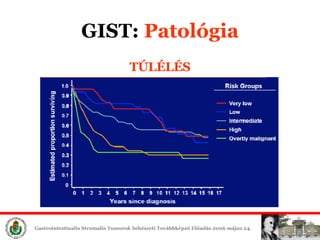
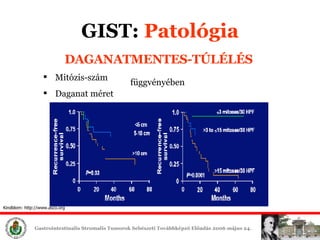
19. BENIGNUS VS. MALIGNUS Benignus â malignus ÃĄtalakulÃĄs fokozatos MÃĐg nagyon kis mÃĐretÅą(< 2 cm), alacsony mitÃģzis szÃĄmÚ GIST tumorok is adhatnak ÃĄttÃĐtet HosszÚ utÃĄnkÃķvetÃĐs esetÃĐn bÃĄrmely GIST malignizÃĄlÃģdhat A rezekÃĄlt tumorok 50%-a kiÚjulhat 5 ÃĐv alatt GIST : ąĘēđģŲīĮąôÃģēĩūąēđ
20. GIST : ąĘēđģŲīĮąôÃģēĩūąēđ BENIGNUS VS. MALIGNUS >5/50 HPF BÃĄrmennyi >10/50 HPF >5 cm >10 cm BÃĄrmekkora High risk 6-10/50 HPF <5/50 HPF <5 cm 5-10 cm Intermediate risk <5/50 HPF 2-5 cm Low risk <5/50 HPF <2 cm Very Low risk MitÃģzis-szÃĄm MÃĐret
39. GIST: SebÃĐszeti °ėąðģúąðąôÃĐēõ ElsÅdleges a mÅątÃĐti °ėąðģúąðąôÃĐēõ KÃmÃĐletes preparÃĄlÃĄs: szÃģrÃģdÃĄs! A teljes pseudocapsula eltÃĄvolÃtÃĄsa
40. GIST: SebÃĐszeti °ėąðģúąðąôÃĐēõ CÃĐl: a teljes rezekciÃģ 1-2 cm ÃĐp szÃĐl elÃĐg RadikÃĄlis mÅątÃĐt nem ad semmifÃĐle elÅnyt MikroszkÃģpikus (R1) pozitÃv rezekciÃģs szÃĐlek esetÃĐn: Re-rezekciÃģnak nincs elÅnye AdjuvÃĄns imatinib °ėąðģúąðąôÃĐēõ Lymphadenektomia ritkÃĄn indikÃĄlt
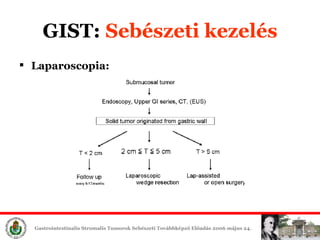
42. GIST: SebÃĐszeti °ėąðģúąðąôÃĐēõ Laparoscopia: lassan teret nyer: pl. gyomor-ÃĐk resectio DE! szÃģrÃģdÃĄs Nincs mÃĐg prospektÃv randomizÃĄlt tanulmÃĄny NCCN ajÃĄnlÃĄsban nem ajÃĄnlott , max. csak <2m-nÃĐl kisebb elvÃĄltozÃĄsokban JapÃĄnban gyakori, akÃĄr 5 cm <T<10 cm KonverziÃģ : kapszula-ruptÚra megelÅzÃĐse!!
43. EurÃģpai K ons z en z us K onferenc ia AjÃĄnlÃĄsok (Lugano , 2 004) Ann Oncol. 2005 Apr;16(4):566-78. NCCN Sarcoma Guideline (GIST) 2005 GIST: TerÃĄpiÃĄs protokoll
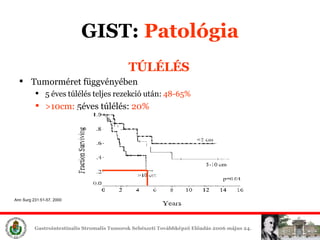
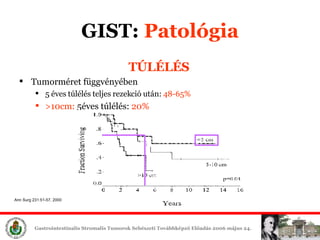
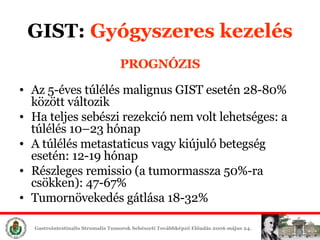
53. PROGNÃZIS Az 5- ÃĐves tÚlÃĐlÃĐs malign us GIST esetÃĐn 28 - 80% kÃķzÃķtt vÃĄltozik Ha teljes sebÃĐszi rezekciÃģ nem volt lehetsÃĐges: a tÚlÃĐlÃĐs 10â23 hÃģnap A tÚlÃĐlÃĐs metastatic us vagy kiÚjulÃģ betegsÃĐg esetÃĐn: 12 - 19 hÃģnap RÃĐszleges remissio (a tumormassza 50%-ra csÃķkken): 47-67% TumornÃķvekedÃĐs gÃĄtlÃĄsa 18-32% GIST: GyÃģgyszeres °ėąðģúąðąôÃĐēõ
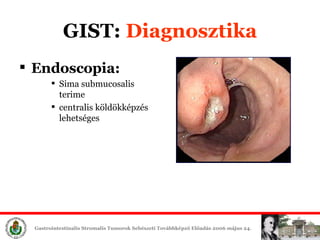
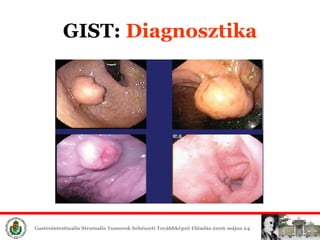
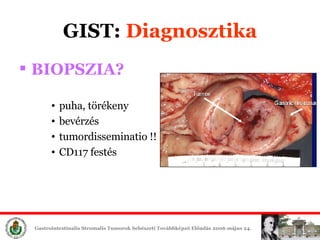
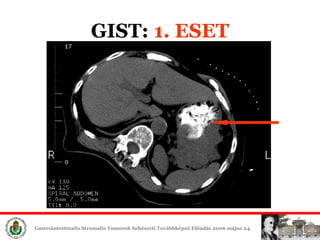
54. GIST: 1. ESET 69-ÃĐves nÅbeteg Panaszok : 3 hÃģnapos anorexia, felhasi fÃĄjdalom, -7kg Gastroscopia : tÃķrÃĐkeny, exophyticus terime a nagygÃķrbÞleten Biopszia : csak gyulladÃĄsos sejtek Hasi CT : 5x6cm-es terime
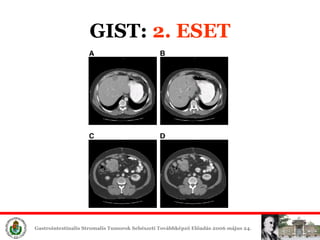
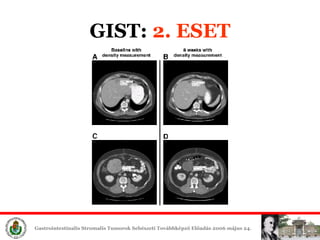
64. GIST: 3. ESET 57-ÃĐves fÃĐrfi Hasat teljesen kitÃķltÅ tumor Biopszia: CD117: GIST P.o. imatinib + gastric outlet obstr.miatt antiemeticum 2 nap alatt (!) vÃĄlasz, antiemeticum leÃĄllÃthatÃģ 6 hÃģnap alatt igen gyors tumormÃĐret csÃķkkenÃĐs 6.HÃģnap utÃĄn Újra nÃķvekedett, de folyadÃĐktartalmÚ
71. A CD117 negatÃv GIST ek egy csoportjÃĄban (max.2-3%) a P D GFRa (platelet derived growth factor receptor alpha - egy mÃĄsik tirozin-kinÃĄz ) gÃĐnen aktivÃĄlÃģ mutÃĄciÃģ van Egy vizsgÃĄlat 40 -bÅl 14 CD117 negatÃv GIST -ben talÃĄltak PDGFRa mutÃĄciÃģt, ami intracellularisan ua. hatÃĄst fejtette ki, mint a c-kit GIST: CD 117 negatÃv
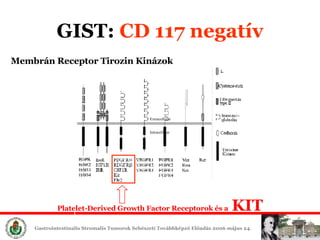
72. GIST : CD 117 negatÃv Extracellular Intracellular Membr ÃĄn Receptor T i ro zin Kin ÃĄzok Platelet-Derived Growth Factor Receptor ok ÃĐs a KIT
73. Az Imatinib hatÃĐkony lehet CD117 negatÃv, de PDGF R mutÃĄciÃģt mutatÃģ tumorok esetÃĐn is ElÅrehaladott, c-kit negat Ãv GIST -ben szenvedÅ betegek I matinib °ėąðģúąðąôÃĐēõÃĐt meg kell kezdeni PDGF R mutÃĄciÃģt mutatÃģ tumorok csak egy rÃĐsze I matinib-s z en zitÃv GIST: CD 117 negatÃv
74. Az OEP csak CD117 pozitivitÃĄs esetÃĐn tÃĄmogatja a Gleevec °ėąðģúąðąôÃĐēõt! GIST: CD 117 negatÃv
75. GIST: 5. ESET 58-ÃĐves fÃĐrfi 1978-ban ileum hamartoma miatt resectio Rendszeres CT kontroll AAA miatt: gyomor GIST HistolÃģgia revÃziÃģja: GIST exon 11 KIT mutÃĄciÃģ PET: mÃĄj ÃĐs intraabdomin. metastasisok MÅątÃĐt: gyomor resectio, de met. irresecabilis
76. GIST: 5. ESET SzÃķvettan: GIST AAA szignifikÃĄnsan nÃķvekedett, de onkol. inop.-nak ÃtÃĐltÃĐk 600mg/nap Gleevec, 3 hÃģnap utÃĄn partialis remissio Urgens mÅątÃĐt AAA ruptura miatt, mÅątÃĐti lelet: szÃĄmos csepleszmet., de szÃķvettan: necrosis Gleevec tovÃĄbb
77. GIST: 5. ESET 3 hÃģnap mÚlva Roux-Y-revÃziÃģ: multiplex perit.ÃĐs mÃĄj elvÃĄltozÃĄs, biopszia:hegszÃķvet, CD117 negatÃv Fontos a terÃĄpiÃĄs vÃĄlasz monitorozÃĄsa TerÃĄpiÃĄs nihilizmus nem megengedhetÅ
78. GIST: KÃĐrdÃĐsek Mi az adjuvÃĄns Gleevec szerepe R 0 -resectio utÃĄn? RezekÃĄbilisnak tÅąnÅ GIST neoadjuvÃĄns °ėąðģúąðąôÃĐēõe? Milyen hosszÚ legyen az adjuvÃĄns Gleevec °ėąðģúąðąôÃĐēõ? TÃķbb-szervi rezekciÃģ? Mi a helyzet a Gleevec non-respodereknÃĐl?
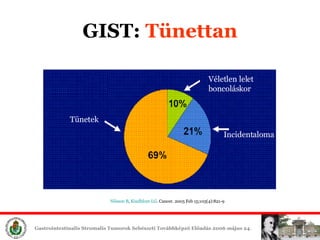
79. GIST: ÃsszefoglalÃĄs I. Leggyakoribb GI sarcoma Gyakran tÞnetmentes DiagnÃģzis: ImmunhisztokÃĐmia 98% CD117 + Minden GIST potenciÃĄlisan malignus MÃĐret, mitÃģzis-szÃĄm szerinti besorolÃĄs
81. GIST: Internet Az elÅadÃĄs ÃķsszefoglalÃģja letÃķlthetÅ a http://sebeszet.blogspot.com -rÃģl!
Editor's Notes
#2: Tisztelt hallgatÃģsÃĄg, tisztelt kollÃĐgÃĄk! ElÅadÃĄsomban a gastrointestinÃĄlis stromÃĄlis tumorokrÃģl beszÃĐlek. FelmerÞl a kÃĐrdÃĐs, hogy miÃĐrt kell ennek a tumortÃpusnak kÞlÃķn elÅadÃĄst szentelni. Ennek tÃķbb oka van.ElÅszÃķris