Procalcitonin
•Download as DOCX, PDF•
6 likes•3,246 views

Chỉ điểm tình trạng nhiễm khuẩn































More Related Content
What's hot (20)
Viewers also liked (13)











Similar to Procalcitonin (20)




















More from Nguy·ªÖn H·∫°nh (15)















Procalcitonin
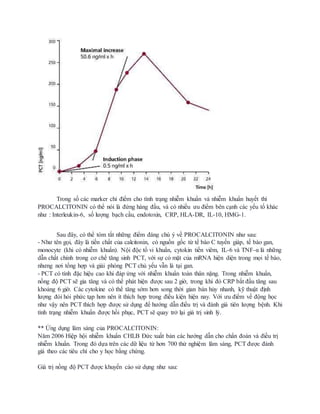
- 1. Trong s·ªë c√°c marker ch·ªâ ƒëi·ªÉm cho t√¨nh tr·∫°ng nhi·ªÖm khu·∫©n v√† nhi·ªÖm khu·∫©n huy·∫øt th√¨ PROCALCITONIN c√≥ th·ªÉ n√≥i l√† ƒë·ª©ng h√†ng ƒë·∫ßu, v√† c√≥ nhi·ªÅu ∆∞u ƒëi·ªÉm b√™n c·∫°nh c√°c y·∫øu t·ªë kh√°c nh∆∞ : Interleukin-6, s·ªë l∆∞·ª£ng b·∫°ch c·∫ßu, endotoxin, CRP, HLA-DR, IL-10, HMG-1. Sau ƒë√¢y, c√≥ th·ªÉ t√≥m t·∫Øt nh·ªØng ƒëi·ªÉm ƒë√°ng ch√∫ √Ω v·ªÅ PROCALCITONIN nh∆∞ sau: - Nh∆∞ t√™n g·ªçi, ƒë√¢y l√† ti·ªÅn ch·∫•t c·ªßa calcitonin, c√≥ ngu·ªìn g·ªëc t·ª´ t·∫ø b√†o C tuy·∫øn gi√°p, t·∫ø b√†o gan, monocyte (khi c√≥ nhi·ªÖm khu·∫©n). N·ªôi ƒë·ªôc t·ªë vi khu·∫©n, cytokin ti·ªÅn vi√™m, IL-6 v√† TNF-Œ± l√† nh·ªØng d·∫´n ch·∫•t ch√≠nh trong c∆° ch·∫ø tƒÉng sinh PCT, v·ªõi s·ª± c√≥ m·∫∑t c·ªßa mRNA hi·ªán di·ªán trong m·ªçi t·∫ø b√†o, nh∆∞ng n∆°i t·ªïng h·ª£p v√† gi·∫£i ph√≥ng PCT ch·ªß y·∫øu v·∫´n l√† t·∫°i gan. - PCT c√≥ t√≠nh ƒë·∫∑c hi·ªáu cao khi ƒë√°p ·ª©ng v·ªõi nhi·ªÖm khu·∫©n to√†n th√¢n n·∫∑ng. Trong nhi·ªÖm khu·∫©n, n·ªìng ƒë·ªô PCT s·∫Ω gia tƒÉng v√† c√≥ th·ªÉ ph√°t hi·ªán ƒë∆∞·ª£c sau 2 gi·ªù, trong khi ƒë√≥ CRP b·∫Øt ƒë·∫ßu tƒÉng sau kho·∫£ng 6 gi·ªù. C√°c cytokine c√≥ th·ªÉ tƒÉng s·ªõm h∆°n song th·ªùi gian b√°n h·ªßy nhanh, k·ªπ thu·∫≠t ƒë·ªãnh l∆∞·ª£ng ƒë√≤i h·ªèi ph·ª©c t·∫°p h∆°n n√™n √≠t th√≠ch h·ª£p trong ƒëi·ªÅu ki·ªán hi·ªán nay. V·ªõi ∆∞u ƒëi·ªÉm v·ªÅ ƒë·ªông h·ªçc nh∆∞ v·∫≠y n√™n PCT th√≠ch h·ª£p ƒë∆∞·ª£c s·ª≠ d·ª•ng ƒë·ªÉ h∆∞·ªõng d·∫´n ƒëi·ªÅu tr·ªã v√† ƒë√°nh gi√° ti√™n l∆∞·ª£ng ≤˙·ªán≥Û. Khi t√¨nh tr·∫°ng nhi·ªÖm khu·∫©n ƒë∆∞·ª£c h·ªìi ph·ª•c, PCT s·∫Ω quay tr·ªü l·∫°i gi√° tr·ªã sinh l√Ω. ** ·ª®ng d·ª•ng l√¢m s√†ng c·ªßa PROCALCITONIN: NƒÉm 2006 Hi·ªáp h·ªôi nhi·ªÖm khu·∫©n CHLB ƒê·ª©c xu·∫•t b·∫£n c√°c h∆∞·ªõng d·∫´n cho ch·∫©n ƒëo√°n v√† ƒëi·ªÅu tr·ªã nhi·ªÖm khu·∫©n. Trong ƒë√≥ d·ª±a tr√™n c√°c d·ªØ li·ªáu t·ª´ h∆°n 700 th·ª≠ nghi·ªám l√¢m s√†ng, PCT ƒë∆∞·ª£c ƒë√°nh gi√° theo c√°c ti√™u ch√≠ cho y h·ªçc b·∫±ng ch·ª©ng. Gi√° tr·ªã n·ªìng ƒë·ªô PCT ƒë∆∞·ª£c khuy·∫øn c√°o s·ª≠ d·ª•ng nh∆∞ sau:
- 2. Giá trị bình thường: PCT < 0,05 ng/ml Giá trị PCT < 0,10ng/ml: Không chỉ định dùng kháng sinh Giá trị PCT < 0,25ng/ml: Không khuyến cáo dùng kháng sinh, nếu trị liệu giảm xuống mức này thì tiếp tục dùng cho hiệu quả. Giá trị PCT > 0,25ng/ml: Khuyến cáo sử dụng kháng sinh. Giá trị PCT > 0,50 ng/ml: Chỉ định kháng sinh là bắt buộc. Giá trị PCT 0,50 - 2,0 (ng/ml): Nhiễm khuẩn do đáp ứng viêm hệ thống tương đối, nguyên nhân có thể là chấn thương, phẫu thuật sau chấn thương, sốc tim... Giá trị PCT 2,0 - 10 (ng/ml): Đáp ứng viêm hệ thống nghiêm trọng (SIRS), nguyên nhân bởi nhiễm trùng hệ thống và nhiễm khuẩn huyết, chưa có suy đa tạng. Giá trị PCT > 10 ng/ml: Đáp ứng viêm hệ thống sâu do nhiễm khuẩn huyết nghiêm trọng hoặc sốc nhiễm khuẩn. Trong nhi khoa PCT giúp chẩn đoán sớm nhiễm khuẩn xâm lấn với độ chính xác cao ( sốt <12 giờ), đặc biệt là nhiễm khuẩn toàn thân nặng de dọa mạng sống của trẻ. Ngoài ra, PCT còn được chứng minh tiên lượng được biến chứng, diễn biến của nhiễm khuẩn huyết. PCT có thể còn giúp phân biệt giữa nhiễm khuẩn huyết và SIRS, phân biệt giữa nhiễm khuẩn và thải ghép... Ngoài ra trong ứng dụng trị liệu kháng sinh dựa trên giám sát nồng độ PCT, các nhà nghiên cứu về PCT cũng khuyến cáo : Trường hợp 1: Ngừng kháng sinh nếu: a. Nồng độ PCT giảm <0,1 ng/ml Tình trạng lâm sàng cải thiện đáng kể b. Trường hợp 2:Đổi kháng sinh khác nếu: Nồng độ PCT không giảm và Triệu chứng lâm sàng tồn tại hoặc tăng thêm dấu hiệu nhiễm trùng. c. Trường hợp 3:Tiếp tục kháng sinh đang dùng nếu: Triệu chứng lâm sàng được cải thiện Nồng độ PCT không ứng với trường hợp 1 và 2. Nguồn: 1. medscape: Procalcitonin: Uses in the Clinical Laboratory for the Diagnosis of Sepsis 2. procalcitonin.com 3. Khoa khóa sinh, BV Bạch Mai Hà Nôi. 4. Bệnh viện Đa khoa MEDLATEC.