
















































![Anteromedial pneumothorax
(Anteromedial Recess)
AP chest X-ray showing right
pneumothorax with complete lung collapse.
Transverse CT confirms this finding.
The classical appearance in the upright
position is the presence of radiolucent air
and the absence of lung markings between
the shrunken lung and the parietal pleura.
In the supine ventilated patient, gravity and
the effects lung disease often give rise to a
different appearance of the so-called
‘supine pneumothorax’. The pneumothorax
is usually anteromedial or sub-pulmonic
causing lucent upper quadrants of the
abdomen, sharp superior surfaces of the
diaphragm, the deep sulcus sign, and
visualization of the inferior surface of
consolidated lung.[9] Less often, the
pneumothorax is apical, lateral (displaces
the minor fissure from the chest wall), or
posteromedial. False-positive appearances
may occur from skin folds, overlying
tubing/dressing/lines, and prior chest tube
tracks.](https://image.slidesharecdn.com/pm34-131015032853-phpapp01/85/Pm34-50-320.jpg)










































More Related Content
What's hot (20)
Viewers also liked (20)


















Pm34 胸部x線写真の読影⑤
- 1. Point Master 34 胸部X線写真の読影⑤ ABCDEFプロトコール 外傷性気胸を中心に ( 胸写 CT EFAST)
- 2. Case1 32歳女性: 呼吸苦 ショック ER portable
- 3. Case1 32歳女性: 呼吸苦 ショック A) ER portable 挿管(-) B) 左第3-7肋骨骨折がみられる。また、左胸部に軽度の皮下気腫を認め る。(頸部は提示されていない) C) 左側 CP angle は dull です。 D) 気管?右左気管支とも激しく右方に偏移。 E) 縦隔は極端に右側へ偏位している(圧排されている) 。心拡大なし。左 右の心辺縁および、下大静脈もスムーズに追え、左右肺門部の拡大は ありません。 F) 左側胸壁から肺が虚脱し、左横隔膜が下方に偏移している。 Chest X-ray of left-sided pneumothorax (seen on the right in this image). The left thoracic cavity is partly filled with air occupying the pleural space. The mediastinum is shifted to the opposite side
- 4. Case1 32歳女性: 呼吸苦 ショック
- 5. Case1 32歳女性: 呼吸苦 ショック Q1 診断は? A1 ① 左緊張性気胸 ② 左第3-7肋骨骨折 Q2 直ちに行わなければならない処置は? A2 緊急胸腔ドレナージ
- 6. Case1 32歳女性: 呼吸苦 ショック Q1 診断は? A1 ① 左緊張性気胸 ② 左第3-7肋骨骨折 Q2 直ちに行わなければならない処置は? A2 緊急胸腔ドレナージ
- 7. Case1 32歳女性: 呼吸苦 ショック Q1 診断は? A1 ① 左緊張性気胸 ② 左第3-7肋骨骨折 Q2 直ちに行わなければならない処置は? A2 緊急胸腔ドレナージ
- 8. Case1 32歳女性: 呼吸苦 ショック Q1 診断は? A1 ① 左緊張性気胸 ② 左第3-7肋骨骨折 Q2 直ちに行わなければならない処置は? A2 緊急胸腔ドレナージ (チェストチューブ挿入または緊急脱気)
- 9. Case2 30歳女性: 呼吸苦 ショック 【主訴】 呼吸苦 【現病歴】 ? ? ? ? ? バイクで走行中に濡れていた路面でスリップし、転倒。 左側胸部痛と呼吸苦あり。 血圧は 160/90 mmHg 脈拍は120 /min. SpO2は85%。 GCS:14(V4)。 ドクターヘリで現場へ向かったあなたは、触診で皮下腫 を認めた。
- 10. Case2 30歳女性: 呼吸苦 ショック
- 11. Case2 30歳女性: 呼吸苦 ショック まずすべき事は何か? 【解答】 チェストチューブ挿入 または緊急脱気
- 12. Case2 30歳女性: 呼吸苦 ショック まずすべき事は何か? 【解答】 チェストチューブ挿入 または緊急脱気
- 13. Case2 30歳女性: 呼吸苦 ショック 【経過】 ? ? ? 32Frのチェストチューブを挿入した。 少量の血と脱気を確認した。 SpO2の改善が認められない。
- 14. Case2 30歳女性: 呼吸苦 ショック SpO2の改善が認められないのはなぜか? 【解答】 開放性気胸だから
- 15. Case2 30歳女性: 呼吸苦 ショック SpO2の改善が認められないのはなぜか? 【解答】 開放性気胸だから
- 16. 開放性気胸 Sucking Chest Wound ? 胸壁に穴があき、胸腔が大気と交通することにより生じる気 胸。 穴が大きくて空気が通過しやすい場合には、吸気時の陰圧に よって開通部より空気が胸腔に入り、呼気時には開通部より 出て行くため、肺の換気が不十分となり低酸素血症に陥る。 ? チェストチューブのみでは処置不十分 ! ? Q どうする? (JPTEC) 開放創に対して3辺テーピング(JPTEC)。
- 17. 開放性気胸 Sucking Chest Wound ? 胸壁に穴があき、胸腔が大気と交通することにより生じる気 胸。 穴が大きくて空気が通過しやすい場合には、吸気時の陰圧に よって開通部より空気が胸腔に入り、呼気時には開通部より 出て行くため、肺の換気が不十分となり低酸素血症に陥る。 ? チェストチューブのみでは処置不十分 ! ? Q どうする? (JPTEC) 開放創に対して3辺テーピング(JPTEC)
- 18. 開放性気胸 Sucking Chest Wound ? 胸壁に穴があき、胸腔が大気と交通することにより生じる気 胸。 穴が大きくて空気が通過しやすい場合には、吸気時の陰圧に よって開通部より空気が胸腔に入り、呼気時には開通部より 出て行くため、肺の換気が不十分となり低酸素血症に陥る。 ? チェストチューブのみでは処置不十分 ! ? Q どうする? (JPTEC) A 開放創に対して3辺テーピング(JPTEC) 開放創に対して3辺テーピング(JPTEC)
- 19. 3辺テーピング
- 20. 3辺テーピング
- 22. Case3 28歳/男性
- 29. Case4 32歳/男性
- 36. Case4 32歳/男性 ? 呼吸苦の原因として最も可能性が高い のは? ? ? 【解答】 再膨張性肺水腫 虚脱率の大きな気胸、脱気まで日数が経 過している気胸は再膨張性肺水腫のリス クが高い。
- 37. Case 5 22歳/女性 【主訴】 呼吸苦?前胸部痛 【既往歴】 気管支喘息 【現病歴】 ? ? ? 2日前から感冒症状あり。 今日の朝から喘息発作あり。 発作中に急に前胸部痛あり。
- 38. Case 5 22歳/女性
- 40. Case 5 22歳/女性 診断は何でしょうか? 【解答】 縦隔気肿
- 41. Case 5 22歳/女性
- 43. Case 6 19歳/男性: 胸部単纯写真异常
- 44. Case 6 19歳/男性: 胸部単纯写真异常
- 45. 19歳/男性: 胸部単纯写真异常
- 46. Case 6 19歳/男性: 胸部単纯写真异常 A) 立位PA B) 左頚部?左側胸部にも皮下気腫と思われる透過性亢進域がある。 C) 両側 CP angle は sharp です。 D) 気管?右左気管支とも異常はない。 E) 食道左縁や下行大動脈に沿って線状の透過性亢進が見られ、縦隔気肿 が疑われる。 F) 右肺尖部には境界明瞭な線状影がある。 【診断】(特発性)縦隔気肿、皮下気腫、右奇静脈葉
- 47. 特発性縦隔気肿 特発性のものは稀であり、ERを受診する患者の30,000人に1人、入院患者の 800~42,000人に1人の割合と報告されている。 症状としては、胸痛(89%)、呼吸苦(67%)、頚部痛(11%)、頚部腫脹?嗄声 (共に6%)、嚥下困難感(3%)がある。身体所見では皮下気腫が最も多く、特 に初期には頚部で顕著であり徐々に胸部まで拡がる。Hamman音(聴診上、 心拍動に合わせて聞こえるcrunching/bubbling音;『バリバリ、ボコボコ』)も 特徴的である。 特発性であれば通常1週間もすれば自然治癒し、後遺症を残すことは殆どな い。この症例でも頚部痛?呼吸苦が初期症状であり、痛みは徐々に胸部に拡 がった。Hamman音も聴取し、典型的な病歴?身体所見を呈した。喫煙歴や非 合法ドラッグの使用歴、喘息の既往もなかった。約1週間の経過観察後、軽快 し退院した。 【参考文献】 ?Andrew E. Newcomb, C. Peter Clarke. Spontaneous pneumomediastinum; A benign curiosity or a significant problem? CHEST 2005;128:3298-3302
- 48. Supine Pneumothorax Distribution of pneumothorax in the supine and semirecumbent critically ill adult. Tocino IM, Miller MH, Fairfax WR. AJR Am J Roentgenol. 1985 May;144(5):901-5. Although a number of radiologic signs of pneumothorax in the supine patient have been reported, the frequency of involvement of various pleural recesses has not been emphasized. In 88 critically ill patients with 112 pneumothoraces, the anteromedial (38%) and subpulmonic (26%) recesses were the most commonly involved in the supine and semirecumbent position. In this study, 30% of pneumothoraces were not initially detected by the clinician or radiologist, and half of these progressed to tension pneumothorax. Knowledge of the most common recesses involved in pneumothorax and aggressive use of additional radiographic views, including computed tomography, should increase detection of pneumothoraces in critically ill patients.
- 49. Supine Pneumothorax Pneumothorax in supine patient Dr Yuranga Weerakkody and Dr Vinod G Maller et al. A pneumothorax does not display classical signs when a patient is positioned supine for a chest radiograph. Instead, it may be demonstrated by looking for the following signs: ? relative lucency of the involved - basilar hyperlucency ? deep, sometimes tongue like costophrenic sulcus - deep sulcus sign ? anteromedial pneumothorax (earliest location) increased sharpness of the adjacent mediastinal margin and diaphragm increased sharpness of the cardiac borders ? visualization of the anterior costophrenic sulcus - double diaphragm sign ? visualization of the inferior edge of the collapsed lung above the diaphragm ? depression of the ipsilateral hemidiaphragm- depression of diaphragm
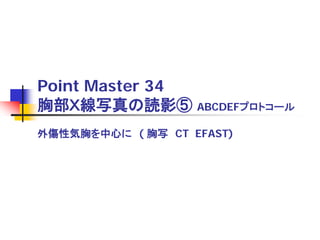
- 50. Anteromedial pneumothorax (Anteromedial Recess) AP chest X-ray showing right pneumothorax with complete lung collapse. Transverse CT confirms this finding. The classical appearance in the upright position is the presence of radiolucent air and the absence of lung markings between the shrunken lung and the parietal pleura. In the supine ventilated patient, gravity and the effects lung disease often give rise to a different appearance of the so-called ‘supine pneumothorax’. The pneumothorax is usually anteromedial or sub-pulmonic causing lucent upper quadrants of the abdomen, sharp superior surfaces of the diaphragm, the deep sulcus sign, and visualization of the inferior surface of consolidated lung.[9] Less often, the pneumothorax is apical, lateral (displaces the minor fissure from the chest wall), or posteromedial. False-positive appearances may occur from skin folds, overlying tubing/dressing/lines, and prior chest tube tracks.
- 53. Medial Stripe Sign 縦隔?心陰影の左側に沿って 透亮影が大動脈弓を越えて続 く。 Sign of LUL(left upper lobe) collapse -looks like an "air crescent", where hyperexpanded superior segment of LLL surrounds aortic arch - lucent stripe between the medial edge of the collpased segment and the aortic arch. The is lower lube that has been pulled up by the collpased lung (Luftsichel Sign)
- 54. Deep Sulcus Sign Chest X-ray demonstrating the deep sulcus sign suggestive of left anterior pneumothorax in a supine ventilated patient.
- 55. Deep Sulcus Sign
- 62. Safe Triangle The 'safe triangle' for inserting a chest drain. The most common position for chest tube insertion is in the midaxillary line, through the ‘safe triangle’ . This position minimizes risk to underlying structures such as the viscera and internal mammary artery and avoids damage to muscle and breast tissue resulting in unsightly scarring. A more posterior position may be chosen if suggested by the presence of a loculated collection. While this is relatively safe, it is not the preferred site as it is more uncomfortable for the patient to lie on after insertion and there is more risk of the drain kinking.