
































More Related Content
Similar to chiarimalformationcpc-170629145030.pptx (20)
More from vuanh1603 (12)










Recently uploaded (20)



















chiarimalformationcpc-170629145030.pptx
- 1. Chiari Malformation Dr.Usman Haqqani Resident Neurosurgery B LRH PESHAWAR
- 2. Case scenerio • A 34 year old female presents to the opd with progressive weakness in both her arms associated with intermittent bilateral shoulder pain .She has not noticed any functional impairment and is still working normally.On further asking she admits she has intermittent headaches over the lower occipital area and aggravates with coughing and sneezing.
- 3. examination • On physical examination, she has no neurologic deficits other than • Reduced of sensitivity to hot and cold sensation over her arms • Numbness and tingling over arms • Loss of muscle strength in her right shoulder and hand which could not be appreciated very clearly.
- 4. History based differential diagnosis
- 7. Post op day 4
- 8. Review in Opd at 6 months • Power Right arm had improved from 4/5 to 5/5. • No occipital headaches with coughing and straining • No other neurological deficit
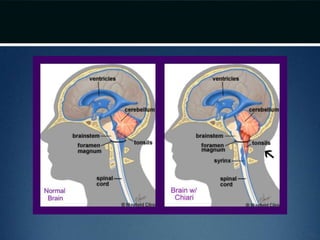
- 9. Introduction • Chiari malformations are pathological herniations of the hindbrain through the foramen magnum and into the cervical spinal canal. • 1890s – Hans Chiari, pathologist described four congenital malformations • Majority are congenital; but can be acquired as well  secondary CIM
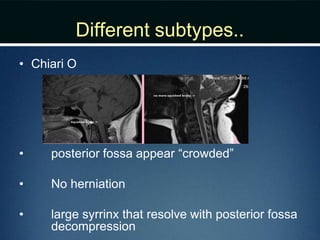
- 10. Different subtypes.. • Chiari O • posterior fossa appear “crowded” • No herniation • large syrrinx that resolve with posterior fossa decompression
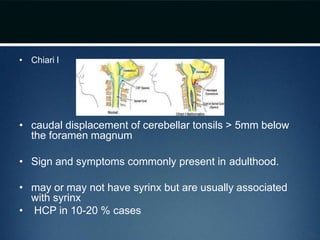
- 11. • Chiari I • caudal displacement of cerebellar tonsils > 5mm below the foramen magnum • Sign and symptoms commonly present in adulthood. • may or may not have syrinx but are usually associated with syrinx • HCP in 10-20 % cases
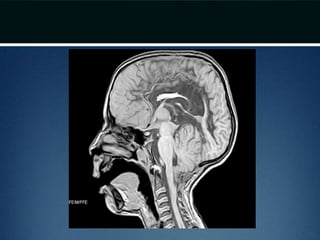
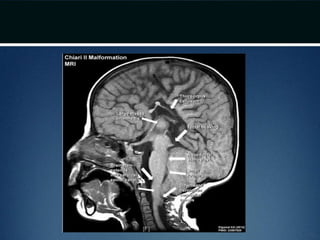
- 14. • Chiari II • caudal migration of cerebellar vermis • almost always occurs in patients with neural tube defects (myelomeningocele and encephalocele) • syrinx is common • HCP in 90% cases
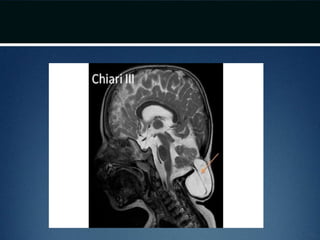
- 17. • Chiari III • rare and extreme form of hindbrain hernia • <1% occurrence • has low occipital and high cervical sacs containing significant portions of the cerebellum and brainstem. • Hydrocephalus is common and severe neurological and developmental problems present
- 19. • Chiari IV • cerebellar hypoplasia or aplasia • not a form of hindbrain hernia • its inclusion is hence debatable
- 21. Chiari I Malformation • Theory: Difficulty in rapidly equilibriating the CSF pressure wave seen during the Valsalva maneuver • Prolonged intracranial hypertension relative to intraspinal compartment  downward migration of the cerebellar tonsils  obstruction of normal CSF flow from 4th ventricle to cervical subarachnoid space  CIM • Obstruction of Foramen of Magendie by arachnoid veils or septation might also lead to the same
- 22. • Conditions artificially lowering the intraspinal pressure relative to ICP like lumboperitoneal shunt – iatrogenic/acquired • Some derailment on chromosomes 9 and 15
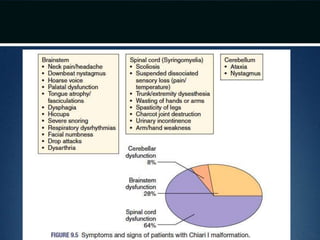
- 23. Clinical Presentation • S&S related to brainstem compression • S&S related to cerebellar compression • S&S related to spinal cord dysfunction secondary to syringomyelia
- 26. Clinical Presentations.. • Non radicular occipital or cervical pain • Dysesthesias in the C2 dermatome • Neckpain and headache - exacerbated on exertion or by coughing or sneezing (valsalva induced) • Non verbal children  irritability, crying, failure to thrive, opisthotonos
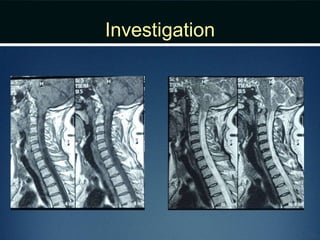
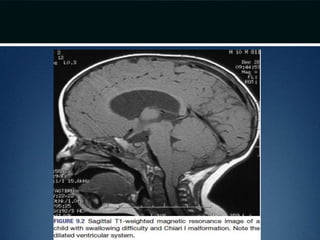
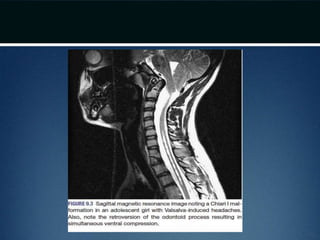
- 27. Diagnosis • MRI – Craniovertebral junction and entire spinal cord • 50-75% patients have syringomyeliasyrinx • CT – bony abnormality; plain films for evaluating stability issues • Dynamic MRI (cine MRI) – for CSF flow around the CVJ
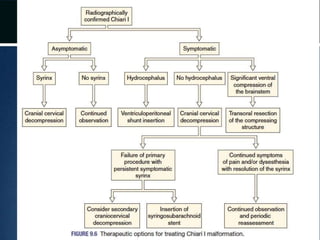
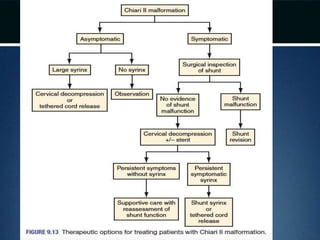
- 29. Treatment • Treatment is different for symptomatic and non syptomatic patients • No medical treatment • Observation in asymptomatic patients without an associated syrinx • Surgery: for symptomatic patients and asymptomatic patients with syrinx
- 30. Treatment • 10% patients with CIM – associated hydrocephalus – CSF diversionary shunt or ETV as the initial form of therapy • Symptomatic ventral compression out of proportion to dorsal compression  ventral decompression (transoral odontoid resection)
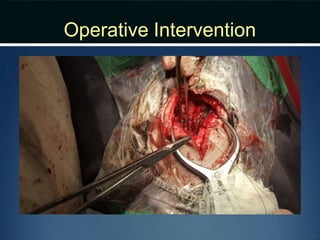
- 31. • Most common surgical procedure: Posterior fossa decompression • Goal: enlarge posterior fossa to recreate cisterna magna, thereby permitting normal flow of CSF • Syrinx decrease in size and does not require direct Rx in majority after this
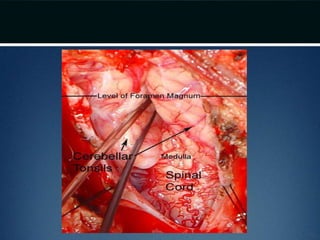
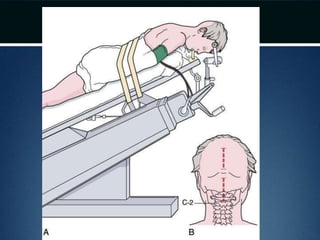
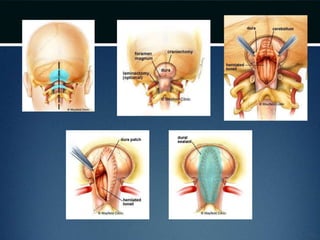
- 32. Posterior fossa decompression.. • Prone position and neck flexed • Incision from below inion to the spinous process of C2 • Avascular plane (nuchal ligament) b/t paraspinous muscles followed down to bone and subperiosteal dissection performed • Moderate suboccipital craniectomy, width of the foramen magnum followed by removal of posterior arch of atlas
- 33. Posterior fossa decompression.. • Dura opened • Arachnoid adhesions obstructing flow removed and the floor of the 4th ventricle examined • Portion of occipital pericranium harvested through a separate incision and duroplasty performed
- 37. Posterior fossa decompression.. result • Encouraging result in long term follow up • Early treatment tends toward better outcomes • ~85% patients – relief of head and neck pain esp. if valsalva induced • Associated syrinx decrease in size or collapse in majority • If no improvement in symptoms and size of syrinx in 6 months  reexploration with coagulation or resection of a cerebellar tonsil
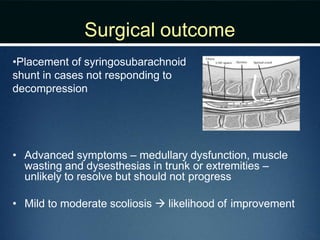
- 38. Surgical outcome •Placement of syringosubarachnoid shunt in cases not responding to decompression • Advanced symptoms – medullary dysfunction, muscle wasting and dysesthesias in trunk or extremities – unlikely to resolve but should not progress • Mild to moderate scoliosis  likelihood of improvement
- 40. Chiari II malformation • Caudal displacement of cerebellar vermis, lower brainstem and fourth ventricle seen exclusively in patients with myelomeningocele • Numerous other anomalies associated in various combinations – vertical straight sinus – large venous lakes in the tentorium – fenestrations in falx, which is often not well formed – gyri of left and right hemispheres interdigitate – “Chinese lettering” on axial MRI
- 41. Pathophysiology.. • Similar to CIM – difficulty in equilibrating dynamic CSF pulse pressure induced by valsalva • Leaking from myelomeningocele sac lowers intraspinal pressure
- 42. Clinical presentation.. • Pertaining to brainstem, cerebellar and spinal cord dysfunction • Usualy present in infancy/early childhood • Worst outcome if symptoms appear before 3 months age • Stridor, apnea and dysphagia resulting in aspiration  might cause death • Nystagmus – earliest sign of cerebellar dysfunction • Initial spinal cord symptoms (weakness, bowel and bladder dysfunction) – secondary to inadequate formation of the lower spinal cord
- 44. Diagnosis • MRI – cranial and spinal • Plain dynamic cervical spine radiographs  instability
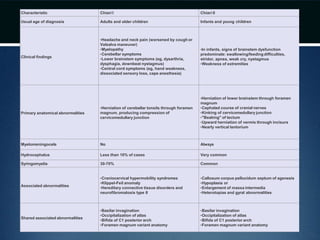
- 46. Characteristic Chiari I Chiari II Usual age of diagnosis Adults and older children Infants and young children Clinical findings •Headache and neck pain (worsened by cough or Valsalva maneuver) •Myelopathy •Cerebellar symptoms •Lower brainstem symptoms (eg, dysarthria, dysphagia, downbeat nystagmus) •Central cord symptoms (eg, hand weakness, dissociated sensory loss, cape anesthesia) •In infants, signs of brainstem dysfunction predominate: swallowing/feedingdifficulties, stridor, apnea, weak cry, nystagmus •Weakness of extremities Primary anatomical abnormalities •Herniation of cerebellar tonsils through foramen magnum, producing compression of cervicomedullary junction •Herniation of lower brainstem through foramen magnum •Cephalad course of cranial nerves •Kinking of cervicomedullary junction •"Beaking" of tectum •Upward herniation of vermis through incisura •Nearly vertical tentorium Myelomeningocele No Always Hydrocephalus Less than 10% of cases Very common Syringomyelia 30-70% Common Associated abnormalities •Craniocervical hypermobility syndromes •Klippel-Feil anomaly •Hereditary connective tissue disorders and neurofibromatosis type II •Callosum corpus pellucidum septum of agenesis •Hypoplasia or •Enlargement of massa intermedia •Heterotopias and gyral abnormalities Shared associated abnormalities •Basilar invagination •Occipitalization of atlas •Bifida of C1 posterior arch •Foramen magnum variant anatomy •Basilar invagination •Occipitalization of atlas •Bifida of C1 posterior arch •Foramen magnum variant anatomy
- 47. • Thank you!!