

Kyrkan
- 1. Tredje trosartikeln: Den Helige Andes verksamhet Ī▒Jag tror p? en helig, allm?nnelig kyrka, de heligas samfundĪ▒ Wednesday, October 20, 2010
- 2. Ordens betydelse ? F?rsamling, gr. Ekklesia, Ī▒kallad utĪ▒. F?rsamlingen ?r kallad ut ur v?rlden, utanf?r l?gret, till ett liv med Kristus. ? Kyrka, gr. kyriakhe, Ī▒Tillh?r HerrenĪ▒. Ordet kyrka anv?nds som synonym till ordet f?rsamling (ekklesia). Skriver man Kyrkan med stort K s? avser man den v?rldsvida f?rsamlingen. ? Kyrka. Byggnad som ?r helgad ?t Herren. Byggnadens historiska urprung kommer fr?n hemmen vid medelhavet. ? Guds rike. Ett vidare begrepp ?n den v?rldsvida kyrkan. Den inbegriper hela Guds rike i himlen och p? jorden. Vi ber att det skall komma till v?rt liv i Fader V?r b?nen. Wittenbergs stadskyrkas altartavla, Lukas Cranach. Wednesday, October 20, 2010
- 3. F?rsamlingen ?r Kristi Kropp (1. Kor. 12:27) ? Kristi v?rldsvida f?rsamling eller Kyrkan ?r Ī▒en, helig, allm?nnelig och apostoliskĪ▒ (Niceanska ? En, eftersom trosbek?nnelsen) Kristus ?r en. ? Helig, eftersom Kristus ?r helig ? Allm?nnelig, eftersom den tillh?r alla troende. ? Apostolisk, eftersom den h?ller sig till den apostoliska l?ran. Ī▒.. alla ?r ni ett i KristusĪ▒. Gal. 3:28 Wednesday, October 20, 2010
- 4. Kristi f?rsamlingskropp ?verskrider gr?nser av tid och rum ? Medlemmarna i f?rsamlings-kroppen ?r av tv? slag a) den triumferande kyrkan (ecclesia triumphans, de heliga som kommit fram, Hebr. 12:1) b) den k?mpande kyrkan (ecclesia militans, den kyrka som i tiden k?mpar mot synden, v?rlden och dj?vulen.) Wednesday, October 20, 2010
- 5. Corpus permixtum Ī▒en blandad kyrkaĪ▒ ? I f?rsamlingen h?r i tiden ?r de (Augustinus) sant heliga och skrymtarna blandade (Ī▒?kerns ogr?sĪ▒ Matt. 13:24-30). Endast Gud kan slutligen avg?ra r?tt. ? Med v?ra ler?gon f?r vi inte skilja eller undanskuffa ur f?rsamlingen de som har en r?tt bek?nnelse och som k?mpar p? omv?ndelsens v?g. ? Ī▒Med k?rlekens ?gonĪ▒ skall vi betrakta alla d?pta och bek?nnande som kristna, Ī▒med trons ?gonĪ▒ betraktar vi endast de som kristna som Gud har f?rklarat r?ttf?rdiga inf?r himmelsens domstol. I denna tid kan vi endast se med k?rlekens ?gon. (Enligt Luther) ? Vi ?r skyldiga att fullt ut ?lska alla kristna eftersom Gud har ?lskat oss utan villkor. Wednesday, October 20, 2010
- 6. Kyrkan eller f?rsamlingen ?r fr?lsningens gemenskap Guds kyrkas fasta grundval, dess sk?ld och v?rn i strid ?r Herren Jesus Kristus, Guds Son fr?n evig tid. (Sionsharpan 68) "Jag har f?tt all makt i himlen och p? jorden. G? d?rf?r ut och g?r alla folk till l?rjungar! D?p dem i Faderns och Sonens och den helige Andes namn och l?r dem att h?lla allt vad jag har befallt er. Och se, jag ?r med er alla dagar intill tidens slutĪ▒ Ī▒...Men kyrkan ?r de heligas samfund, i vilket evangelium rent f?rkunnas och sakramenten r?tt f?rvaltas... En tro, ett dop, en Gud som ?r allas Fader etc. (Ef. 4:5--6). Augsburgska bek?nnelsen (CA 7): Wednesday, October 20, 2010
- 7. Att f?renas med f?rsamlingen ?r att f?renas med fr?lsningen ? Dopet ?r Kristus-d?rren till f?rsamlingens gemenskap. Genom tron tar vi emot dopets g?va varje dag. I Fornkyrkan var dopsk?len placerad vid kyrkans d?rr och man gick via den in i fr?lsningens gemenskap. ? Ocks? med m?nga andra ord vittnade han och uppmanade dem: "L?t er fr?lsas fr?n detta bortv?nda sl?kte." De som d? tog emot hans ord d?ptes, och s? ?kade antalet l?rjungar den dagen med omkring tre tusen.Ī▒ (Apg. 2:40-41). ? Ī▒Den som tror och blir d?pt skall bli fr?lst, men den som inte tror skall bli f?rd?md.Ī▒ (Mark. 16:16) Dopet ?r Kristus-d?rren till fr?lsningen och ? Gud har f?renat dopet med sitt l?fte. nattvardsgemenskapen. Bild: Muonio kyrkas altare Guds Ord ger dopet dess kraft. Ī▒N?r Ordet kommer till ?mnet blir det ett sakrament.Ī▒ (Augustinus). Wednesday, October 20, 2010
- 8. Kyrkans makt (ius ecclesia) ? Kyrklig makt (nycklamakten) betyder att f?rsamlingen har r?tt att predika Ordet och f?rvalta sakramenten samt kalla och ins?tta herdar f?r f?rsamlingen. ? Makten har getts f?r att evangeliet skall utspridas (dop- och missionsbefallningen) och villol?ror bek?mpas. ? Denna makt har varje f?rsamling. Dessutom har varje kristen f?tt fullmakt att predika evangeliet i sin n?romgivning. ? Enskilda kristna kan inte Evangeliets l?senyckel anv?nda bindenyckeln. ?ven befriar fr?n synd. apostlarna anv?nde dem Bindenyckeln inneb?r att man tillsammans med f?rsamlingen. binds i synden och f?r inte Anv?ndningen av bindenyckeln komma till nattvarden. tillh?r pastorn och Bindenyckeln ?r en allvarlig f?rsamlingen (1 Kor. 5:3-4; Matt. varning och kallelese till omv?ndelse fr?n den v?g som 18:17). leder till f?rd?rv. Wednesday, October 20, 2010
- 9. Kyrkan ?r en bek?nnande gemenskap L?rans grund: ? Bibeln L?ran: ? De gammalkyrkliga trosbek?nnelserna Nicenska-, apostoliska- och Athanasianska trosbek?nnelsen ? De lutherska bek?nnelseskrifterna Wednesday, October 20, 2010
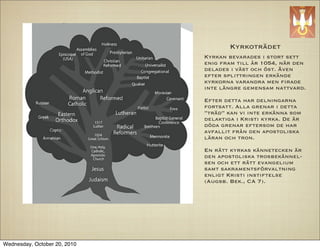
- 10. Kyrkotr?det Kyrkan bevarades i stort sett enig fram till ?r 1054, n?r den delades i v?st och ?st. ?ven efter splittringen erk?nde kyrkorna varandra men ?rade inte l?ngre gemensam nattvard. Efter detta har delningarna fortsatt. Alla grenar i detta Ī▒tr?dĪ▒ kan vi inte erk?nna som delaktiga i Kristi kyrka. De ?r d?da grenar eftersom de har avfallit fr?n den apostoliska l?ran och tron. En r?tt kyrkas k?nnetecken ?r den apostoliska trosbek?nnel- sen och ett r?tt evangelium samt sakramentsf?rvaltning enligt Kristi instiftelse (Augsb. Bek., CA 7). Wednesday, October 20, 2010
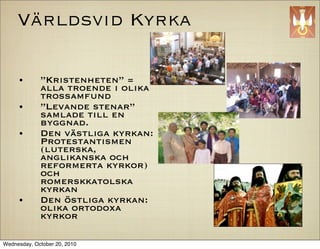
- 11. V?rldsvid Kyrka ? Ī▒KristenhetenĪ▒ = alla troende i olika trossamfund ? Ī▒Levande stenarĪ▒ samlade till en byggnad. ? Den v?stliga kyrkan: Protestantismen (luterska, anglikanska och reformerta kyrkor) och romerskkatolska kyrkan ? Den ?stliga kyrkan: olika ortodoxa kyrkor Wednesday, October 20, 2010
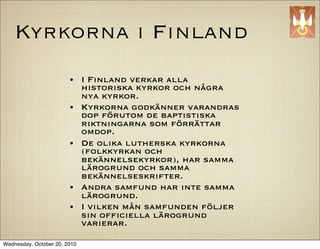
- 12. Kyrkorna i Finland ? I Finland verkar alla historiska kyrkor och n?gra nya kyrkor. ? Kyrkorna godk?nner varandras dop f?rutom de baptistiska riktningarna som f?rr?ttar omdop. ? De olika lutherska kyrkorna (folkkyrkan och bek?nnelsekyrkor), har samma l?rogrund och samma bek?nnelseskrifter. ? Andra samfund har inte samma l?rogrund. ? I vilken m?n samfunden f?ljer sin of?ciella l?rogrund varierar. Wednesday, October 20, 2010
- 13. Splittring, sekter och schismer De?nition av termer Enligt Bibelns helhetsbild ?r Kristi f?rsamlingskropp den som har samlats ihop Gr. ”─”╔”ų”Ž”ę”ė”┴”ę”╔”┴”╔, ”┴”╔”č”┼”ę”┼”╔?, ”ę”ų”╔”ę”╠”┴, dikastasia, genom det apostloliska evangeliet. Den kan heresia, skisma inte ramla s?nder i delar men fr?n den kan sekter utg? som f?ljer falska l?ror. Splittring, oenighet, dikastasia. Ī▒St? skildĪ▒, Ī▒tudelningĪ▒, Ī▒splittringĪ▒. (Dika = Guds Ord Ī▒kallar och samlarĪ▒ av alla folk itu; stasis = st?, station). (Gal. 5:20)). till den enda Kristi kropp som ?nns. Ordet Sekt, parti, heresia. NT anv?nder detta bygger nya gemenskaper p? evangeliets ord om sekt, parti och skolbildningar. (Apg. grund. 5:17, 1 Kor. 11:19). Fr?n ordet haireo, Ī▒er?vra, r?da ?verĪ▒, Ī▒antagen ?sikt, L?rom?ssiga grupper som uppstiger mot uppfattningĪ▒ (speciellt avvikande ?sikt), Ī▒Kristi l?raĪ▒ inom f?rsamlingen ?r k?ttets Ī▒?loso?sk skolaĪ▒. Ursprungligen ett verk och d?rmed synd. P? samma s?tt ?r det sv?rmiskt fenomen och n?got man g?r f?r att tj?na sig sj?lv. Heresier har synd att av illvilja h?lla sig ?tskilld om man undantryckt den h?lsosamma l?ran. har samma l?ra. (Gal. 5:19-20). Schism, skisma. Ī▒..F?rst och fr?mst h?r jag Det fanns olika ?sikter och man kunde ta att det f?rekommer stridigheter (skismata) bland er, n?r ni m?ts i f?rsamlingen, och miste redan p? apostlarnas tid. Allt detta var delvis tror jag att det ?r s?. Partier inte synd. Den apostoliska Ī▒v?genĪ▒ och (heireseis) m?ste ?nnas bland er, f?r att det Ī▒vandringenĪ▒ var ?nd? norm enligt vilken Gud skall visa sig vilka det ?r som h?ller provet. ledde dem som var av annan ?sikt. (Fil. 3:15-18). (1 Kor. 11:18). En l?ra som avviker fr?n Bibelns l?ra Dj?vulen, satan, gr. Diabolos. Hebr. splittrar alltid en f?rsamling. Det Ī▒?klagare (i domstol), den som hindrar och Ī▒?tskiljerĪ▒ (diabolos) fr?n Guds Ords bedrar p? ett l?mskt s?tt. Gr. Ī▒den som h?lsosamma l?ra. kastar ?tskilltĪ▒, Ī▒motst?ndareĪ▒, Ī▒konspirat?rĪ▒ (to plot against). Wednesday, October 20, 2010
- 14. Bliv kvar i broderlig k?rlek ? Var innerligt tillgivna varandra i broderlig k?rlek. ?vertr?ffa varandra i ?msesidig hedersbevisningĪ▒ (Rom. 12:10) ? Ī▒Lev i endr?kt med varandra. T?nk inte p? det som ?r h?gt utan h?ll er till det som ?r ringa. Var inte sj?lvkloka. .Ī▒ Rom. 12:16 ? Ī▒Br?der, bli kvar i brodersk?rleken.Ī▒ (Hebr. 13:1) ? Ī▒G?r d?rf?r allt ni kan f?r att i er tro visa dygd,.. i gudsfruktan broderlig k?rlek och i k?rleken till br?derna k?rlek till alla m?nniskor. Ī▒ (2. Petr. 1:6-7) ? Ī▒Ty liksom kroppen ?r en och har m?nga lemmar, men kroppens alla lemmar - och de ?r m?nga - utg?r en kropp, s? ?r det ocks? med Kristus. I en Ande har vi alla blivit d?pta f?r att h?ra till en kropp, vare sig vi ?r judar eller greker, slavar eller fria, och alla har vi f?tt en och samme Ande utgjuten ?ver oss. Kroppen best?r ju inte av en enda lem utan av m?nga.Ī▒ (1. Kor. 12:12-14). Wednesday, October 20, 2010
- 15. Sin enda grund har kyrkan 4. N?r l?gn och v?ld f?rmeras var ?r d? jordens salt? Vem hj?lper och vem helar vid v?rldens s?nderfall? M? kyrkan bli som fordom ett hj?rta och en sj?l, en fristad mitt i oron, f?r sanningen ett v?rn 5.Guds kyrka ?r gemenskap med Fadern och hans Son, det sk?dar hon och erfar i Andens kraft och n?d. Guds helgon och martyrer betygar det med blod. Omkring dem sjunger rymden d?r segerns 1. Sin enda grund har kyrkan i Kristus, Fr?lsaren. kyrka bor. Hon ?r hans egen byggnad, den nya skapelsen. I v?rlden som han l?ste fr?n m?rkret med sitt blod, blev hon den brud han kr?nte med evangelii ord. (Psalmboken 167, Samuel John Stone 2. Fast spridd i m?nga l?nder ?r kyrkan endast 1866. Svensk en och har en enda Herre och en bek?nnelse. ?vers?ttning Olov Av vatten f?dd och Ande till ett och samma Hartman 1981, en hopp, hon g?r till l?fteslandet med samma annan ?vers?ttning resekost. ?nns av Anna ?lander i 3. Med undran och med l?je ser v?rlden hur Sionsharpan 68) hon slits av tusen tvister s?nder och nekar sig Guds frid. Hur s?llsamt klingar orden i kyrkor utan fred om Herrens frid p? jorden, om Guds barmh?rtighet. Wednesday, October 20, 2010