MSA update 2022.pdf
6 likes13,848 views

Kyoto Neurology ForumŻ©2022─Ļ9į┬10╚šŻ®żŪ╩╣ė├żĘż┐ź╣źķźżź╔żŪż╣Ż«







































More Related Content
What's hot (20)
Similar to MSA update 2022.pdf (20)


















More from Takayoshi Shimohata (20)




















MSA update 2022.pdf
- 2. Ż├ŻŽŻ╔ ķ_╩Š ╣PŅ^░k▒Ēš▀├¹Ż║ Ž┬«x ŽĒ┴╝ ▒Šųvč▌ż╦ķv▀BżĘķ_╩Šż╣ż┘żŁCOIķvéSż╦żóżļŲ¾śIż╚żĘżŲ ó┘ŅÖå¢Ż║ ż╩żĘ ó┌ųĻ▒Żėą?└¹ęµŻ║ ż╩żĘ ó█╠žįS╩╣ė├┴ŽŻ║ ż╩żĘ ó▄ųvč▌┴ŽŻ║ ż╩żĘ ó▌įŁĖÕ┴ŽŻ║ ż╩żĘ ó▐╩▄ėÜ蹊┐?╣▓═¼čąŠ┐┘MŻ║ źļź¾ź╔ź┘ź├ź» ó▀ŖXč¦╝─ĖČĮŻ║ ż╩żĘ óÓ╝─ĖČųvū∙╦∙╩¶Ż║ ż╩żĘ óß┘ø┤ŲĘż╩ż╔ż╬ł¾│ĻŻ║ ż╩żĘ │÷Ąõż╬ėø▌dż╬ż╩żżź╣źķźżź╔żŽŻ¼č▌š▀ż¼ū„│╔żĘż┐żŌż╬żŪż╣Ż«
- 4. GilmanĘųŅÉż╬ĮUŠĢ ? 1998─ĻŻ¼į\ČŽż╦ķvż╣żļĄ┌Ż▒╗ž║Ž═¼╔∙├„ ? 2008─ĻŻ¼į\ČŽż╦ķvż╣żļĄ┌Ż▓╗ž║Ž═¼╔∙├„ ? ź©źėźŪź¾ź╣ż╦╗∙ż┼ż»żŌż╬żŪżŽż╩ż»Ż¼ź©źŁź╣źč®`ź╚? ź¬źįź╦ź¬ź¾ż╚żĘżŲū„│╔żĄżņż┐Ż«
- 5. 14─ĻķgżŪ├„żķż½ż╦ż╩ż├ż┐å¢Ņ}ĄŃ ó┘ įńŲ┌ż╦į\ČŽż╣żļĖąČ╚ż╦ż½ż▒żŲżżżļŻ« │§į\Ģrż╬MSAį\ČŽż╬ĖąČ╚żŽŻ¼possible MSAżŪ 41ŻźŻ¼probable MSA żŪ18ŻźŻ©Osaki Y, et al. Mov Disord. 2009Ż® ó┌ źņź▄ź╔źčŻ║Ąų┐╣ąįż╬Č©┴xż¼ż╩żżŻ«ėąä┐└²ż¼┤µį┌ż╣żļŻ« ó█ ĪĖred flagsŻ©į\ČŽż“ų¦│ųż╣żļĒŚ─┐Ż®Ī╣ż¬żĶżėĪĖį\ČŽż“ų¦│ų żĘż╩żżĒŚ─┐Ī╣żŽżĄż▐żČż▐ż╩å¢Ņ}ż“║¼żÓŻ«Ī’ ó▄ į\ČŽż╬š²┤_ąįż¼Ą═żżŻ« Ī’ ó▌ į\ČŽż╬ż┐żßż╬Ś╩¢╦ż╦Ė─╔Ųż╬ėÓĄžż¼żóżļŻ«
- 6. 1. Ų╩Ś╩└²żŪŚ╩ėæżĄżņż┐żŌż╬żŪżŽż╩żżŻ« 2. ├„┤_ż╩Č©┴xż¼ż╩żżŻ« 3. MSA-C ż╦īØż╣żļ red flags ż¼ż╩żżŻ« 4. MSA-Pż╚PDż╬Ķaäeż╦ėąė├ż└ż¼Ż¼PSPż╩ż╔ ╦¹ż╬╝▓╗╝ż╚ż╬Ķaäeż╦ż¬ż▒żļėąė├ąįżŽ▓╗├„Ż« ó█ red flagsżŽżĄż▐żČż▐ż╩å¢Ņ}ż“║¼żÓ Red flags: į\ČŽż“ų¦│ųż╣żļĒŚ─┐
- 7. 1. ╣┼ĄõĄ─ż╩═Ķ╦a═ĶżßśöŠ▓ų╣Ģrš±æķ 2. ┼R┤▓Ą─ż╦├„żķż½ż╩ź╦źÕ®`źĒźčź┴®` 3. ĘŪ╦aäłąį╗├ęÖ 4. ŻĘŻĄÜręį╔Žż╬░kųó 5. ▀\äė╩¦š{?źč®`źŁź¾źĮź╦ź║źÓż╬╝ęūÕÜs 6. šJų¬ųóŻ©DSM-IVż╦╗∙ż┼ż»Ż® 7. ČÓ░kąįė▓╗»ųóż“╩Š╦¶ż╣żļ░ū┘|▓Īēõ ó█ į\ČŽż“ų¦│ųżĘż╩żżĒŚ─┐żŌżĄż▐żČż▐ż╩å¢Ņ}ż“║¼żÓ
- 8. 1. ╣┼ĄõĄ─ż╩═Ķ╦a═ĶżßśöŠ▓ų╣Ģrš±æķ 2. ┼R┤▓Ą─ż╦├„żķż½ż╩ź╦źÕ®`źĒźčź┴®` 3. ĘŪ╦aäłąį╗├ęÖĪ·żóżĻ 4. ŻĘŻĄÜręį╔Žż╬░kųóĪ·żóżĻ 5. ▀\äė╩¦š{?źč®`źŁź¾źĮź╦ź║źÓż╬╝ęūÕÜsĪ·żóżĻ 6. šJų¬ųóŻ©DSM-IVż╦╗∙ż┼ż»Ż® Ī·żóżĻ 7. ČÓ░kąįė▓╗»ųóż“╩Š╦¶ż╣żļ░ū┘|▓ĪēõĪ·żóżĻ ? └²═Ōż╚żżż”ż└ż▒żŪż╩ż»Ż¼ųžę¬ż╩ęŌ┴xż“│ųż─Ż©└²Ż║Ė▀²h░kųóŻ® ó█ į\ČŽż“ų¦│ųżĘż╩żżĒŚ─┐żŌżĄż▐żČż▐ż╩å¢Ņ}ż“║¼żÓ
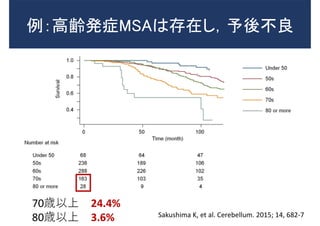
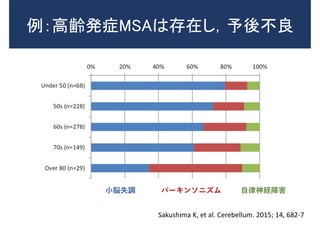
- 9. └²Ż║Ė▀²h░kųóMSAżŽ┤µį┌żĘŻ¼ėĶßß▓╗┴╝ Sakushima K, et al. Cerebellum. 2015; 14, 682-7 70Üręį╔Ž 24.4% 80Üręį╔Ž 3.6%
- 10. ąĪ├Ś╩¦š{ źč®`źŁź¾źĮź╦ź║źÓ ūį┬╔╔±ĮUšŽ║” Sakushima K, et al. Cerebellum. 2015; 14, 682-7 └²Ż║Ė▀²h░kųóMSAżŽ┤µį┌żĘŻ¼ėĶßß▓╗┴╝
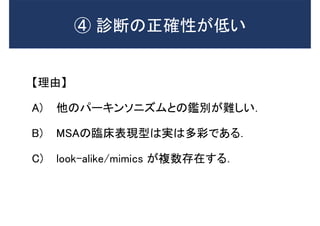
- 11. ĪŠ└Ēė╔Ī┐ A) ╦¹ż╬źč®`źŁź¾źĮź╦ź║źÓż╚ż╬Ķaäeż¼ļyżĘżżŻ« B) MSAż╬┼R┤▓▒Ē¼Fą═żŽīgżŽČÓ▓╩żŪżóżļŻ« C) look-alike/mimics ż¼č}╩²┤µį┌ż╣żļŻ« ? į\ČŽż╬š²┤_ąįż¼Ą═żż
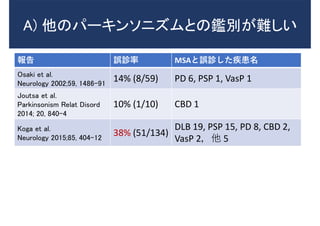
- 12. A) ╦¹ż╬źč®`źŁź¾źĮź╦ź║źÓż╚ż╬Ķaäeż¼ļyżĘżż ł¾Ėµ š`į\┬╩ MSAż╚š`į\żĘż┐╝▓╗╝├¹ Osaki et al. Neurology 2002;59, 1486-91 14% (8/59) PD 6, PSP 1, VasP 1 Joutsa et al. Parkinsonism Relat Disord 2014; 20, 840-4 10% (1/10) CBD 1 Koga et al. Neurology 2015;85, 404-12 38% (51/134) DLB 19, PSP 15, PD 8, CBD 2, VasP 2Ż¼╦¹ 5
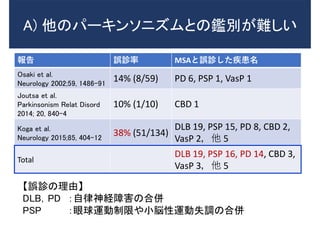
- 13. ł¾Ėµ š`į\┬╩ MSAż╚š`į\żĘż┐╝▓╗╝├¹ Osaki et al. Neurology 2002;59, 1486-91 14% (8/59) PD 6, PSP 1, VasP 1 Joutsa et al. Parkinsonism Relat Disord 2014; 20, 840-4 10% (1/10) CBD 1 Koga et al. Neurology 2015;85, 404-12 38% (51/134) DLB 19, PSP 15, PD 8, CBD 2, VasP 2Ż¼╦¹ 5 Total DLB 19, PSP 16, PD 14, CBD 3, VasP 3Ż¼╦¹ 5 ĪŠš`į\ż╬└Ēė╔Ī┐ DLBŻ¼PD Ż║ūį┬╔╔±ĮUšŽ║”ż╬║ŽüŃ PSP Ż║č█Ū“▀\äėųŲŽ▐żõąĪ├Śąį▀\äė╩¦š{ż╬║ŽüŃ A) ╦¹ż╬źč®`źŁź¾źĮź╦ź║źÓż╚ż╬Ķaäeż¼ļyżĘżż
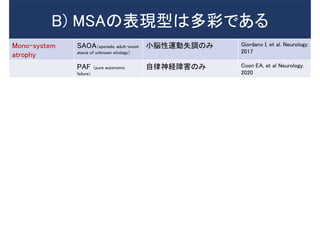
- 14. B) MSAż╬▒Ē¼Fą═żŽČÓ▓╩żŪżóżļ Mono-system atrophy SAOAŻ©sporadic adult©Conset ataxia of unknown etiologyŻ® ąĪ├Śąį▀\äė╩¦š{ż╬ż▀ Giordano I, et al. Neurology. 2017 PAF Ż©pure autonomic failureŻ® ūį┬╔╔±ĮUšŽ║”ż╬ż▀ Coon EA, et al Neurology. 2020
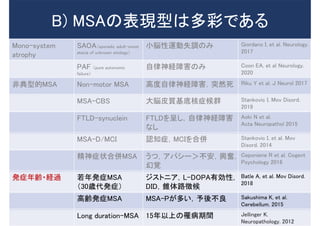
- 15. B) MSAż╬▒Ē¼Fą═żŽČÓ▓╩żŪżóżļ Mono-system atrophy SAOAŻ©sporadic adult©Conset ataxia of unknown etiologyŻ® ąĪ├Śąį▀\äė╩¦š{ż╬ż▀ Giordano I, et al. Neurology. 2017 PAF Ż©pure autonomic failureŻ® ūį┬╔╔±ĮUšŽ║”ż╬ż▀ Coon EA, et al Neurology. 2020 ĘŪĄõą═Ą─MSA Non-motor MSA Ė▀Č╚ūį┬╔╔±ĮUšŽ║”Ż¼═╗╚╗╦└ Riku Y et al. J Neurol 2017 MSA-CBS ┤¾├ŚŲż┘|╗∙Ąū║╦ųó║“╚║ Stankovic I, Mov Disord. 2019 FTLD-synuclein FTLDż“│╩żĘŻ¼ūį┬╔╔±ĮUšŽ║” ż╩żĘ Aoki N et al. Acta Neuropathol 2015 MSA-D/MCI šJų¬ųóŻ¼MCIż“║ŽüŃ Stankovic I, et al. Mov Disord. 2014 Š½╔±ųóū┤║ŽüŃMSA ż”ż─Ż¼źóźčźĘ®`ŻŠ▓╗░▓Ż¼┼dŖ^Ż¼ ╗├ęÖ Ceponiene R et al. Cogent Psychology 2016
- 16. B) MSAż╬▒Ē¼Fą═żŽČÓ▓╩żŪżóżļ Mono-system atrophy SAOAŻ©sporadic adult©Conset ataxia of unknown etiologyŻ® ąĪ├Śąį▀\äė╩¦š{ż╬ż▀ Giordano I, et al. Neurology. 2017 PAF Ż©pure autonomic failureŻ® ūį┬╔╔±ĮUšŽ║”ż╬ż▀ Coon EA, et al Neurology. 2020 ĘŪĄõą═Ą─MSA Non-motor MSA Ė▀Č╚ūį┬╔╔±ĮUšŽ║”Ż¼═╗╚╗╦└ Riku Y et al. J Neurol 2017 MSA-CBS ┤¾├ŚŲż┘|╗∙Ąū║╦ųó║“╚║ Stankovic I, Mov Disord. 2019 FTLD-synuclein FTLDż“│╩żĘŻ¼ūį┬╔╔±ĮUšŽ║” ż╩żĘ Aoki N et al. Acta Neuropathol 2015 MSA-D/MCI šJų¬ųóŻ¼MCIż“║ŽüŃ Stankovic I, et al. Mov Disord. 2014 Š½╔±ųóū┤║ŽüŃMSA ż”ż─Ż¼źóźčźĘ®`ŻŠ▓╗░▓Ż¼┼dŖ^Ż¼ ╗├ęÖ Ceponiene R et al. Cogent Psychology 2016 ░kųó─Ļ²h?ĮU▀^ ╚¶─Ļ░kųóMSA Ż©30Ür┤·░kųóŻ® źĖź╣ź╚ź╦źóŻ¼L-DOPAėąä┐ąįŻ¼ DIDŻ¼ÕF╠Õ┬ĘÅš║“ Batle A, et al. Mov Disord. 2018 Ė▀²h░kųóMSA MSA-Pż¼ČÓżżŻ¼ėĶßß▓╗┴╝ Sakushima K, et al. Cerebellum. 2015 Long duration-MSA 15─Ļęį╔Žż╬ŅŠ▓ĪŲ┌ķg Jellinger K. Neuropathology. 2012
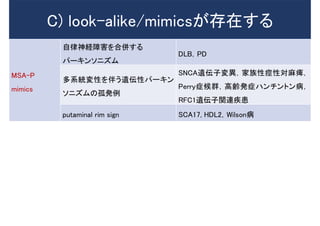
- 17. C) look-alike/mimicsż¼┤µį┌ż╣żļ MSA-P mimics ūį┬╔╔±ĮUšŽ║”ż“║ŽüŃż╣żļ źč®`źŁź¾źĮź╦ź║źÓ DLBŻ¼PD ČÓŽĄĮyēõąįż“░ķż”▀zü╗ąįźč®`źŁź¾ źĮź╦ź║źÓż╬╣┬░k└² SNCA▀zü╗ūėēõ«ÉŻ¼╝ęūÕąį»dąįīØ┬ķ»wŻ¼ Perryųó║“╚║Ż¼Ė▀²h░kų󟎟¾ź┴ź¾ź╚ź¾▓ĪŻ¼ RFC1▀zü╗ūėķv▀B╝▓╗╝ putaminal rim sign SCA17, HDL2Ż¼Wilson▓Ī
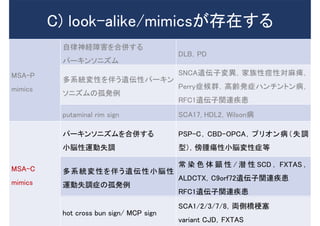
- 18. C) look-alike/mimicsż¼┤µį┌ż╣żļ MSA-P mimics ūį┬╔╔±ĮUšŽ║”ż“║ŽüŃż╣żļ źč®`źŁź¾źĮź╦ź║źÓ DLBŻ¼PD ČÓŽĄĮyēõąįż“░ķż”▀zü╗ąįźč®`źŁź¾ źĮź╦ź║źÓż╬╣┬░k└² SNCA▀zü╗ūėēõ«ÉŻ¼╝ęūÕąį»dąįīØ┬ķ»wŻ¼ Perryųó║“╚║Ż¼Ė▀²h░kų󟎟¾ź┴ź¾ź╚ź¾▓ĪŻ¼ RFC1▀zü╗ūėķv▀B╝▓╗╝ putaminal rim sign SCA17, HDL2Ż¼Wilson▓Ī MSA-C mimics źč®`źŁź¾źĮź╦ź║źÓż“║ŽüŃż╣żļ ąĪ├Śąį▀\äė╩¦š{ PSP-CŻ¼CBD-OPCAŻ¼źūźĻź¬ź¾▓ĪŻ©╩¦š{ ą═Ż®Ż¼░°─[»āąįąĪ├ŚēõąįųóĄ╚ ČÓŽĄĮyēõąįż“░ķż”▀zü╗ąįąĪ├Śąį ▀\äė╩¦š{ųóż╬╣┬░k└² │Ż ╚Š ╔½ ╠Õ Ņć ąį / Ū▒ ąį SCD Ż¼ FXTAS Ż¼ ALDCTXŻ¼C9orf72▀zü╗ūėķv▀B╝▓╗╝ RFC1▀zü╗ūėķv▀B╝▓╗╝ hot cross bun sign/ MCP sign SCA1/2/3/7/8Ż¼üIé╚ś“╣Ż╚¹ variant CJDŻ¼FXTAS
- 19. Imaging mimics of MSA
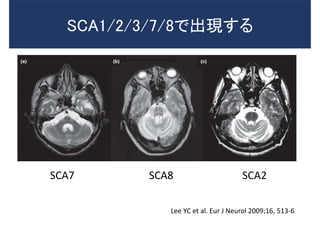
- 20. SCA7 SCA8 SCA2 Lee YC et al. Eur J Neurol 2009;16, 513-6 SCA1/2/3/7/8żŪ│÷¼Fż╣żļ
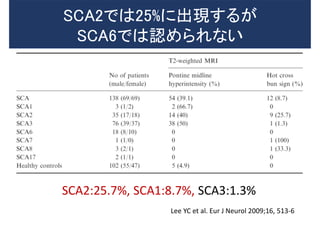
- 21. SCA2:25.7%, SCA1:8.7%, SCA3:1.3% Lee YC et al. Eur J Neurol 2009;16, 513-6 SCA2żŪżŽ25%ż╦│÷¼Fż╣żļż¼ SCA6żŪżŽšJżßżķżņż╩żż
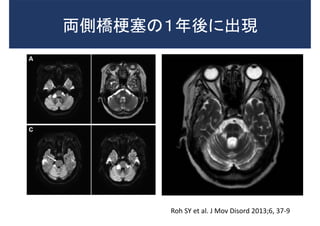
- 22. üIé╚ś“╣Ż╚¹ż╬Ż▒─Ļßßż╦│÷¼F Roh SY et al. J Mov Disord 2013;6, 37-9
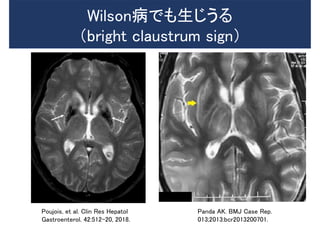
- 23. Poujois, et al. Clin Res Hepatol Gastroenterol. 42:512-20, 2018. Wilson▓ĪżŪżŌ╔·żĖż”żļ Ż©bright claustrum signŻ® Panda AK. BMJ Case Rep. 013;2013:bcr2013200701.
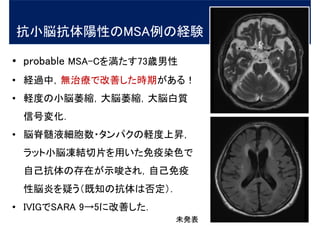
- 25. ? probable MSA-Cż“£║ż┐ż╣73Ür─ąąį ? ĮU▀^ųąŻ¼¤oų╬»¤żŪĖ─╔ŲżĘż┐ĢrŲ┌ż¼żóżļŻĪ ? ▌XČ╚ż╬ąĪ├Ś╬«┐sŻ¼┤¾├Ś╬«┐sŻ¼┤¾├Ś░ū┘| ą┼║┼ēõ╗»Ż« ? ├Ś╝╣¾lę║╝Ü░¹╩²?ź┐ź¾źčź»ż╬▌XČ╚╔ŽĢNŻ¼ źķź├ź╚ąĪ├Śā÷ĮYŪąŲ¼ż“ė├żżż┐├Ōę▀╚Š╔½żŪ ūį╝║┐╣╠Õż╬┤µį┌ż¼╩Š╦¶żĄżņŻ¼ūį╝║├Ōę▀ ąį├Śčūż“ę╔ż”Ż©╝╚ų¬ż╬┐╣╠ÕżŽĘ±Č©Ż®Ż« ? IVIGżŪSARA 9Ī·5ż╦Ė─╔ŲżĘż┐Ż« ┐╣ąĪ├Ś┐╣╠ÕĻ¢ąįż╬MSA└²ż╬ĮU“Y ╬┤░k▒Ē
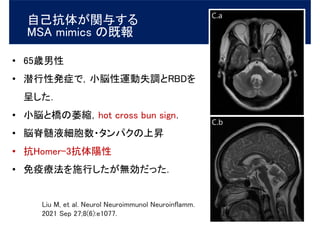
- 26. ? 65Ür─ąąį ? Ū▒ąąąį░kųóżŪŻ¼ąĪ├Śąį▀\äė╩¦š{ż╚RBDż“ │╩żĘż┐Ż« ? ąĪ├Śż╚ś“ż╬╬«┐sŻ¼hot cross bun signŻ« ? ├Ś╝╣¾lę║╝Ü░¹╩²?ź┐ź¾źčź»ż╬╔ŽĢN ? ┐╣Homer-3┐╣╠ÕĻ¢ąį ? ├Ōę▀»¤Ę©ż“╩®ąążĘż┐ż¼¤oä┐ż└ż├ż┐Ż« ūį╝║┐╣╠Õż¼ķvėļż╣żļ MSA mimics ż╬╝╚ł¾ Liu M, et al. Neurol Neuroimmunol Neuroinflamm. 2021 Sep 27;8(6):e1077.
- 27. ąĪ└©Ż▒ ? GilmanĘųŅÉż╬ųž┤¾ż╩å¢Ņ}ĄŃżŽŻ¼į\ČŽż╬š²┤_ąįż¼Ą═żżĄŃ ż╚Ż¼įńŲ┌ż╦į\ČŽż╣żļĖąČ╚ż╦ż½ż▒żŲżżżļĄŃżŪżóżļŻ« ? ą┬į\ČŽ╗∙£╩żŪżŽŻ¼┼R┤▓įć“Yżžż╬ĄŪÕhż╬Ž“╔Žż╦ż─ż╩ż¼żļ ▓Ī│§Ų┌ż╬į\ČŽŠ½Č╚ż╬Ž“╔Žż¼ųžę¬ż╩šnŅ}ż╚ż╩żļŻ« ? ż│ż╬ż┐żßż╦żŽą┬╣µš’ČŽź▐®`ź½®`ż╬╚Ę┴óż¼Ū¾żßżķżņżļŻ«
- 28. GilmanĘųŅÉ ż╬å¢Ņ}ĄŃ MDS MSA į\ČŽ╗∙£╩ äō╦a蹊┐ż╬ ¼Fū┤ į\ČŽ╗∙£╩ż╬śŗįņ Ė─ėåż╬ź▌źżź¾ź╚ ų¦│ųĄ─źąźżź¬ź▐®`ź½®` Wenning GK, et al. Mov Disord. 2022;37(6):1131-1148
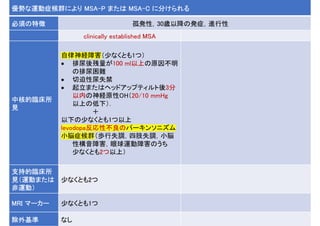
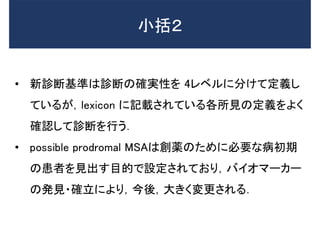
- 29. ą┬į\ČŽ╗∙£╩ż╬╠žÅš ? į\ČŽż╬┤_īgąįż“ 4 ż─ż╬źņź┘źļż╦Ęųż▒żŲČ©┴xżĘżŲżżżļŻ« 1. neuropathologically established MSA 2. clinically established MSA 3. clinically probable MSA 4. possible prodromal MSA ? 3ż─ż╬┼R┤▓į\ČŽź½źŲź┤źĻ®`żŽĮ±ß߯¼Ś╩į^įć“Yż“ąąż”ż╚├„ėøżĄżņżŲżżżļŻ« ? į\ČŽż╦▒žę¬ż╩╦∙ęŖż╬Č©┴xż¼Ż¼lexiconŻ©šZÅĪ─┐ÕhŻ®ż╦ėø▌dżĄżņżŲżżżļŻ« ┼R┤▓į\ČŽź½źŲź┤źĻ®`
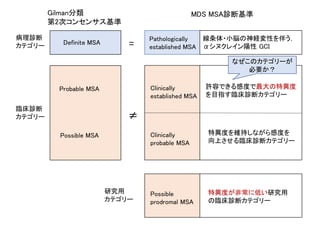
- 30. GilmanĘųŅÉ Ą┌2┤╬ź│ź¾ź╗ź¾źĄź╣╗∙£╩ MDS MSAį\ČŽ╗∙£╩ Definite MSA Probable MSA Possible MSA Pathologically established MSA Clinically established MSA Clinically probable MSA Possible prodromal MSA = Ī┘ ▓Ī└Ēį\ČŽ ź½źŲź┤źĻ®` ┼R┤▓į\ČŽ ź½źŲź┤źĻ®` 蹊┐ė├ ź½źŲź┤źĻ®` įS╚▌żŪżŁżļĖąČ╚żŪūŅ┤¾ż╬╠ž«ÉČ╚ ż“─┐ųĖż╣┼R┤▓į\ČŽź½źŲź┤źĻ®` ╠ž«ÉČ╚ż“ŠS│ųżĘż╩ż¼żķĖąČ╚ż“ Ž“╔ŽżĄż╗żļ┼R┤▓į\ČŽź½źŲź┤źĻ®` ╠ž«ÉČ╚ż¼ĘŪ│Żż╦Ą═żżčąŠ┐ė├ ż╬┼R┤▓į\ČŽź½źŲź┤źĻ®` ŠĆ╠§╠Õ?ąĪ├Śż╬╔±ĮUēõąįż“░ķż”Ż¼ ”┴źĘź╠ź»źņźżź¾Ļ¢ąį GCI ż╩ż╝ż│ż╬ź½źŲź┤źĻ®`ż¼ ▒žę¬ż½Ż┐
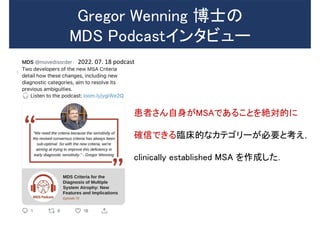
- 31. Gregor Wenning ▓®╩┐ż╬ MDS Podcastźżź¾ź┐źėźÕ®` ╗╝š▀żĄż¾ūį╔Ēż¼MSAżŪżóżļż│ż╚ż“Į~īØĄ─ż╦ ┤_ą┼żŪżŁżļ┼R┤▓Ą─ż╩ź½źŲź┤źĻ®`ż¼▒žę¬ż╚┐╝ż©Ż¼ clinically established MSA ż“ū„│╔żĘż┐Ż« 2022. 07. 18 podcast
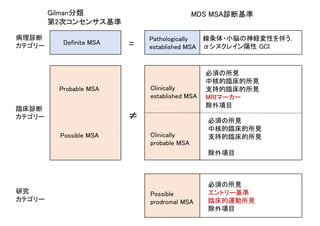
- 32. Definite MSA Probable MSA Possible MSA Pathologically established MSA Clinically established MSA Clinically probable MSA Possible prodromal MSA = Ī┘ ▓Ī└Ēį\ČŽ ź½źŲź┤źĻ®` ┼R┤▓į\ČŽ ź½źŲź┤źĻ®` 蹊┐ ź½źŲź┤źĻ®` ▒žĒÜż╬╦∙ęŖ ųą║╦Ą─┼R┤▓Ą─╦∙ęŖ ų¦│ųĄ─┼R┤▓Ą─╦∙ęŖ MRIź▐®`ź½®` │²═ŌĒŚ─┐ ▒žĒÜż╬╦∙ęŖ ųą║╦Ą─┼R┤▓Ą─╦∙ęŖ ų¦│ųĄ─┼R┤▓Ą─╦∙ęŖ │²═ŌĒŚ─┐ ▒žĒÜż╬╦∙ęŖ ź©ź¾ź╚źĻ®`╗∙£╩ ┼R┤▓Ą─▀\äė╦∙ęŖ │²═ŌĒŚ─┐ ŠĆ╠§╠Õ?ąĪ├Śż╬╔±ĮUēõąįż“░ķż”Ż¼ ”┴źĘź╠ź»źņźżź¾Ļ¢ąį GCI GilmanĘųŅÉ Ą┌2┤╬ź│ź¾ź╗ź¾źĄź╣╗∙£╩ MDS MSAį\ČŽ╗∙£╩
- 33. clinically established MSA clinically probable MSA
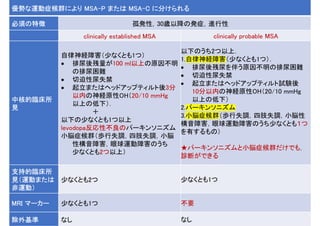
- 34. ā×ä▌ż╩▀\äėųó║“╚║ż╦żĶżĻ MSA-P ż▐ż┐żŽ MSA-C ż╦Ęųż▒żķżņżļ ▒žĒÜż╬╠žÅš ╣┬░kąįŻ¼30ÜręįĮĄż╬░kųóŻ¼▀Mąąąį clinically established MSA ųą║╦Ą─┼R┤▓╦∙ ęŖ ūį┬╔╔±ĮUšŽ║”Ż©╔┘ż╩ż»ż╚żŌ1ż─Ż® ? ┼┼─“ßß▓ą┴┐ż¼100 mlęį╔Žż╬įŁę“▓╗├„ ż╬┼┼─“└¦ļy ? ŪąŲ╚ąį─“╩¦Į¹ ? Ų┴óż▐ż┐żŽźžź├ź╔źóź├źūźŲźŻźļź╚ßß3Ęų ęį─┌ż╬╔±ĮUįŁąįOHŻ©20/10 mmHg ęį╔Žż╬Ą═Ž┬Ż®Ż« Ż½ ęįŽ┬ż╬╔┘ż╩ż»ż╚żŌ1ż─ęį╔Ž levodopaĘ┤ÅĻąį▓╗┴╝ż╬źč®`źŁź¾źĮź╦ź║źÓ ąĪ├Śųó║“╚║Ż©Üiąą╩¦š{Ż¼╦─ų½╩¦š{Ż¼ąĪ├Ś ąįśŗ궚Ž║”Ż¼č█Ū“▀\äėšŽ║”ż╬ż”ż┴ ╔┘ż╩ż»ż╚żŌ2ż─ęį╔ŽŻ® ų¦│ųĄ─┼R┤▓╦∙ ęŖŻ©▀\äėż▐ż┐żŽ ĘŪ▀\äėŻ® ╔┘ż╩ż»ż╚żŌ2ż─ MRI ź▐®`ź½®` ╔┘ż╩ż»ż╚żŌ1ż─ │²═Ō╗∙£╩ ż╩żĘ
- 35. ā×ä▌ż╩▀\äėųó║“╚║ż╦żĶżĻ MSA-P ż▐ż┐żŽ MSA-C ż╦Ęųż▒żķżņżļ ▒žĒÜż╬╠žÅš ╣┬░kąįŻ¼30ÜręįĮĄż╬░kųóŻ¼▀Mąąąį clinically established MSA clinically probable MSA ųą║╦Ą─┼R┤▓╦∙ ęŖ ūį┬╔╔±ĮUšŽ║”Ż©╔┘ż╩ż»ż╚żŌ1ż─Ż® ? ┼┼─“ßß▓ą┴┐ż¼100 mlęį╔Žż╬įŁę“▓╗├„ ż╬┼┼─“└¦ļy ? ŪąŲ╚ąį─“╩¦Į¹ ? Ų┴óż▐ż┐żŽźžź├ź╔źóź├źūźŲźŻźļź╚ßß3Ęų ęį─┌ż╬╔±ĮUįŁąįOHŻ©20/10 mmHg ęį╔Žż╬Ą═Ž┬Ż®Ż« Ż½ ęįŽ┬ż╬╔┘ż╩ż»ż╚żŌ1ż─ęį╔Ž levodopaĘ┤ÅĻąį▓╗┴╝ż╬źč®`źŁź¾źĮź╦ź║źÓ ąĪ├Śųó║“╚║Ż©Üiąą╩¦š{Ż¼╦─ų½╩¦š{Ż¼ąĪ├Ś ąįśŗ궚Ž║”Ż¼č█Ū“▀\äėšŽ║”ż╬ż”ż┴ ╔┘ż╩ż»ż╚żŌ2ż─ęį╔ŽŻ® ęįŽ┬ż╬ż”ż┴2ż─ęį╔ŽŻ« 1.ūį┬╔╔±ĮUšŽ║”Ż©╔┘ż╩ż»ż╚żŌ1ż─Ż®Ż« ? ┼┼─“ßß▓ą─“ż“░ķż”įŁę“▓╗├„ż╬┼┼─“└¦ļy ? ŪąŲ╚ąį─“╩¦Į¹ ? Ų┴óż▐ż┐żŽźžź├ź╔źóź├źūźŲźŻźļź╚įć“Yßß 10Ęųęį─┌ż╬╔±ĮUįŁąįOHŻ©20/10 mmHg ęį╔Žż╬Ą═Ž┬Ż® 2.źč®`źŁź¾źĮź╦ź║źÓ 3.ąĪ├Śųó║“╚║Ż©Üiąą╩¦š{Ż¼╦─ų½╩¦š{Ż¼ąĪ├Śąį śŗ궚Ž║”Ż¼č█Ū“▀\äėšŽ║”ż╬ż”ż┴╔┘ż╩ż»ż╚żŌŻ▒ż─ ż“ėąż╣żļżŌż╬Ż® Ī’źč®`źŁź¾źĮź╦ź║źÓż╚ąĪ├Śųó║“╚║ż└ż▒żŪżŌŻ¼ į\ČŽż¼żŪżŁżļ ų¦│ųĄ─┼R┤▓╦∙ ęŖŻ©▀\äėż▐ż┐żŽ ĘŪ▀\äėŻ® ╔┘ż╩ż»ż╚żŌ2ż─ ╔┘ż╩ż»ż╚żŌ1ż─ MRI ź▐®`ź½®` ╔┘ż╩ż»ż╚żŌ1ż─ ▓╗ę¬ │²═Ō╗∙£╩ ż╩żĘ ż╩żĘ
- 36. ą─č¬╣▄ūį┬╔╔±ĮUšŽ║” Ż©╔±ĮUįŁąįŲ┴óąįĄ═謳RŻ║nOHŻ® ? 謳RĄ═Ž┬ż¼30/15 mmHgęį╔Žż½żķ20/10 mmHgęį╔Žż╦Ė─ėåżĄżņŻ¼ żĄżķż╦”żą─┼─╩²Ż©HRŻ®Ż»”żSBP▒╚Ż╝0.5 bpmŻ»mmHgż¼ūĘ╝ėżĄżņż┐ Ż©nOHżŽč¬łRĄ═Ž┬ż╦żŌż½ż½ż’żķż║Ż¼├}┼─╔ŽĢNż¼Ę”żĘżżŻ®Ż« 30/15 mmHgż╬Ą═Ž┬ż╦żĶżĻį\ČŽż╬╠ž«ÉąįżŽŽ“╔Žż╗ż║Ż¼ĖąČ╚żŽÉÖ╗»żĘż┐ Ż©20/10 mmHgęį╔ŽŻ╗╠ž«ÉČ╚76%Ż¼ĖąČ╚46%Ż¼30/15 mmHgęį╔ŽŻ╗╠ž«ÉČ╚80%Ż¼ĖąČ╚28%Ż®Ż« Fanciulli A, et al. Mov Disord 2019;341926©C8. ? clinically probable MSAżŪżŽŻ¼┴ó╬╗ßß10Ęųęį─┌ż╦Ųż│żļ▀Wčėą═żŌ ūĘ╝ėżĄżņż┐Ż« 3 Ęųż½żķ10Ęųż╦čėķLż╣żļż╚ĖąČ╚ż¼ 18%╔ŽĢNż╣żļŻ« Pavy-Le Traon A, et al. JNNP 2016;87:554-61.
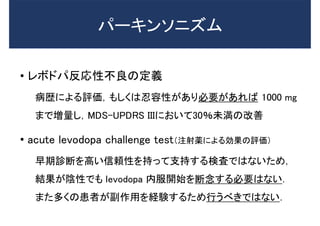
- 37. ? źņź▄ź╔źčĘ┤ÅĻąį▓╗┴╝ż╬Č©┴x ▓ĪÜsż╦żĶżļįuü²Ż¼żŌżĘż»żŽ╚╠╚▌ąįż¼żóżĻ▒žę¬ż¼żóżņżą 1000 mg ż▐żŪēł┴┐żĘŻ¼MDS-UPDRS IIIż╦ż¬żżżŲ30Żź╬┤£║ż╬Ė─╔Ų ? acute levodopa challenge testŻ©ūó╔õ╦aż╦żĶżļä┐╣¹ż╬įuü²Ż® įńŲ┌į\ČŽż“Ė▀żżą┼Ņmąįż“│ųż├żŲų¦│ųż╣żļŚ╩¢╦żŪżŽż╩żżż┐żßŻ¼ ĮY╣¹ż¼ĻÄąįżŪżŌ levodopa ─┌Ę■ķ_╩╝ż“ČŽ─Ņż╣żļ▒žę¬żŽż╩żżŻ« ż▐ż┐ČÓż»ż╬╗╝š▀ż¼Ė▒ū„ė├ż“ĮU“Yż╣żļż┐żßąąż”ż┘żŁżŪżŽż╩żżŻ« źč®`źŁź¾źĮź╦ź║źÓ
- 38. ? Ż┤ĒŚ─┐ż“┤_šJż╣żļŻ« Üiąą╩¦š{Ż¼╦─ų½╩¦š{Ż¼ąĪ├Śąįśŗ궚Ž║” ąĪ├Śąįč█Ū“▀\äėšŽ║”Ż©│ųŠAąįūóęĢĘĮŽ“ąįč█š±żŌżĘż»żŽ Ņ^╬╗Ž┬Ž“żŁč█š±Ż¼źĄź├ź½®`ź╔ąį▀\äė£yČ©▀^┤¾Ż® ? 2ż─ęį╔Žżóżņżą clinically established MSAż╚į\ČŽżĄżņŻ¼ 1ż─ż¼żóżņżą clinically probable MSA ż╚į\ČŽżĄżņżļŻ« ąĪ├Śųó║“╚║
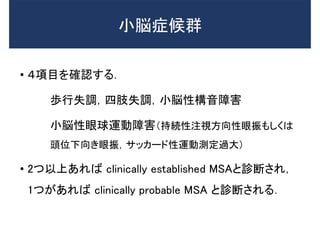
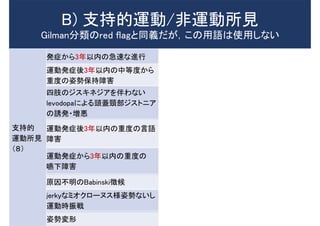
- 40. ų¦│ųĄ─ ▀\äė╦∙ęŖ Ż©ŻĖŻ® ░kųóż½żķ3─Ļęį─┌ż╬╝▒╦┘ż╩▀Mąą ų¦│ųĄ─ ĘŪ▀\äė╦∙ęŖ Ż©ŻĄŻ® ║ĒŅ^┤Ł°Q ▀\äė░kųóßß3─Ļęį─┌ż╬ųąĄ╚Č╚ż½żķ ųžČ╚ż╬ū╦ä▌▒Ż│ųšŽ║” ╬³Ü▌ąįż┐żßŽó ╦─ų½ż╬źĖź╣źŁź═źĖźóż“░ķż’ż╩żż levodopaż╦żĶżļŅ^╔wŅi▓┐źĖź╣ź╚ź╦źó ż╬šT░k?ēłÉÖ └õż┐ż»ēõ╔½żĘż┐╩ųūŃ ▀\äė░kųóßß3─Ļęį─┌ż╬ųžČ╚ż╬čįšZ šŽ║” ▓¬ŲšŽ║” ▀\äė░kųóż½żķ3─Ļęį─┌ż╬ųžČ╚ż╬ ć▓Ž┬šŽ║” ▓ĪĄ─ż╩ą”żż?Ų³żŁ įŁę“▓╗├„ż╬BabinskiÅš║“ jerkyż╩ź▀ź¬ź»źĒ®`ź╠ź╣śöū╦ä▌ż╩żżżĘ ▀\äėĢrš±æķ ū╦ä▌ēõą╬ B) ų¦│ųĄ─▀\äė/ĘŪ▀\äė╦∙ęŖ GilmanĘųŅÉż╬red flagż╚═¼┴xż└ż¼Ż¼ż│ż╬ė├šZżŽ╩╣ė├żĘż╩żż
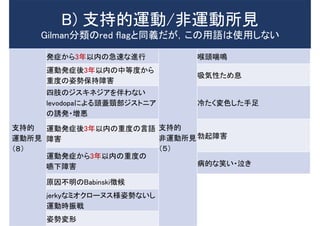
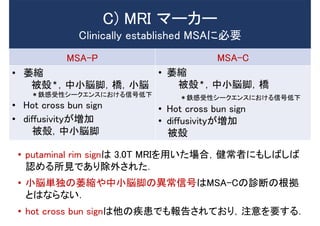
- 41. MSA-P MSA-C ? ╬«┐s ▒╗ÜŻŻ¬Ż¼ųąąĪ├ŚĮ┼Ż¼ś“Ż¼ąĪ├Ś Ż¬Ō¤Ėą╩▄ąįźĘ®`ź»ź©ź¾ź╣ż╦ż¬ż▒żļą┼║┼Ą═Ž┬ ? Hot cross bun sign ? diffusivityż¼ēł╝ė ▒╗ÜŻŻ¼ųąąĪ├ŚĮ┼ ? ╬«┐s ▒╗ÜŻŻ¬Ż¼ųąąĪ├ŚĮ┼Ż¼ś“ Ż¬Ō¤Ėą╩▄ąįźĘ®`ź»ź©ź¾ź╣ż╦ż¬ż▒żļą┼║┼Ą═Ž┬ ? Hot cross bun sign ? diffusivityż¼ēł╝ė ▒╗ÜŻ C) MRI ź▐®`ź½®` Clinically established MSAż╦▒žę¬ ? putaminal rim signżŽ 3.0T MRIż“ė├żżż┐ł÷║ŽŻ¼ĮĪ│Żš▀ż╦żŌżĘżążĘżą šJżßżļ╦∙ęŖżŪżóżĻ│²═ŌżĄżņż┐Ż« ? ąĪ├ŚģgČ└ż╬╬«┐sżõųąąĪ├ŚĮ┼ż╬«É│Żą┼║┼żŽMSA-Cż╬į\ČŽż╬Ė∙Æć ż╚żŽż╩żķż╩żżŻ« ? hot cross bun signżŽ╦¹ż╬╝▓╗╝żŪżŌł¾ĖµżĄżņżŲż¬żĻŻ¼ūóęŌż“ꬿ╣żļŻ«
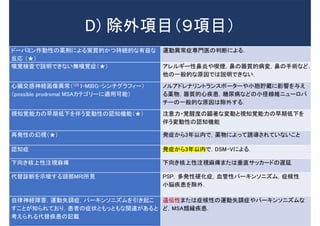
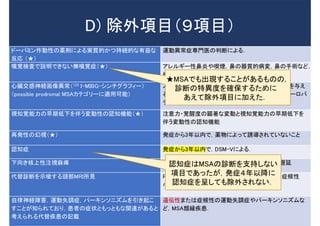
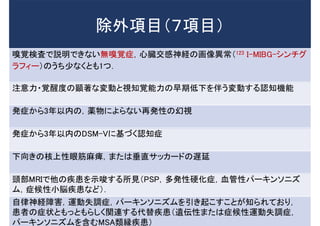
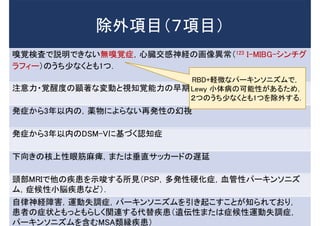
- 42. D) │²═ŌĒŚ─┐Ż©Ż╣ĒŚ─┐Ż® ź╔®`źčź▀ź¾ū„äėąįż╬╦aäłż╦żĶżļīg┘|Ą─ż½ż─│ųŠAĄ─ż╩ėąęµż╩ Ę┤ÅĻ Ż©Ī’Ż® ▀\äė«É│Żųóī¤ķTęĮż╬┼ąČŽż╦żĶżļŻ« ąßęÖŚ╩¢╦żŪšh├„żŪżŁż╩żż¤oąßęÖųóŻ©Ī’Ż® źóźņźļź«®`ąį▒Ūčūżõå╦¤¤Ż¼▒Ūż╬Ų„┘|Ą─▓ĪēõŻ¼▒Ūż╬╩ųągż╩ż╔Ż¼ ╦¹ż╬ę╗░ŃĄ─ż╩įŁę“żŪżŽšh├„żŪżŁż╩żżŻ« ą──ĀĮ╗Ėą╔±ĮU╗ŁŽ±«É│ŻŻ©123 I-MIBG-źĘź¾ź┴ź░źķźšźŻ®`Ż® Ż©possible prodromal MSAź½źŲź┤źĻ®`ż╦▀mė├┐╔─▄Ż® ź╬źļźóź╔źņź╩źĻź¾ź╚źķź¾ź╣ź▌®`ź┐®`żõąĪ░¹┘A╩iż╦ė░Ēæż“ėļż© żļ╦a╬’Ż¼Ų„┘|Ą─ą─╝▓╗╝Ż¼╠Ū─“▓Īż╩ż╔ż╬ąĪŠČŠĆŠSź╦źÕ®`źĒźč ź┴®`ż╬ę╗░ŃĄ─ż╩įŁę“żŽ│²═Ōż╣żļŻ« ęĢų¬ęÖ─▄┴”ż╬įńŲ┌Ą═Ž┬ż“░ķż”ēõäėąįż╬šJų¬ÖC─▄Ż©Ī’Ż® ūóęŌ┴”?ęÖąčČ╚ż╬Ņćų°ż╩ēõäėż╚ęĢų¬ęÖ─▄┴”ż╬įńŲ┌Ą═Ž┬ż“ ░ķż”ēõäėąįż╬šJų¬ÖC─▄ į┘░kąįż╬╗├ęĢŻ©Ī’Ż® ░kųóż½żķ3─Ļęį─┌żŪŻ¼╦a╬’ż╦żĶż├żŲšTī¦żĄżņżŲżżż╩żżż│ż╚ šJų¬ųó ░kųóż½żķ3─Ļęį─┌żŪŻ¼DSM-Vż╦żĶżļŻ« Ž┬Ž“żŁ║╦╔ŽąįūóęĢ┬ķ»w Ž┬Ž“żŁ║╦╔ŽąįūóęĢ┬ķ»wż▐ż┐żŽ┤╣ų▒źĄź├ź½®`ź╔ż╬▀Wčė ┤·╠µį\ČŽż“╩Š╦¶ż╣żļŅ^▓┐MRI╦∙ęŖ PSPŻ¼ČÓ░kąįė▓╗»ųóŻ¼č¬╣▄ąįźč®`źŁź¾źĮź╦ź║źÓŻ¼ųó║“ąį ąĪ├Ś╝▓╗╝ż“│²═ŌŻ« ūį┬╔╔±ĮUšŽ║”Ż¼▀\äė╩¦š{ųóŻ¼źč®`źŁź¾źĮź╦ź║źÓż“ę²żŁŲż│ ż╣ż│ż╚ż¼ų¬żķżņżŲż¬żĻŻ¼╗╝š▀ż╬ųóū┤ż╚żŌż├ż╚żŌż╩ķv▀Bż¼żóżļż╚ ┐╝ż©żķżņżļ┤·╠µ╝▓╗╝ż╬ėø▌d ▀zü╗ąįż▐ż┐żŽųó║“ąįż╬▀\äė╩¦š{ųóżõźč®`źŁź¾źĮź╦ź║źÓż╩ ż╔Ż¼MSAŅÉ┐F╝▓╗╝Ż«
- 43. D) │²═ŌĒŚ─┐Ż©Ż╣ĒŚ─┐Ż® ź╔®`źčź▀ź¾ū„äėąįż╬╦aäłż╦żĶżļīg┘|Ą─ż½ż─│ųŠAĄ─ż╩ėąęµż╩ Ę┤ÅĻ Ż©Ī’Ż® ▀\äė«É│Żųóī¤ķTęĮż╬┼ąČŽż╦żĶżļŻ« ąßęÖŚ╩¢╦żŪšh├„żŪżŁż╩żż¤oąßęÖųóŻ©Ī’Ż® źóźņźļź«®`ąį▒Ūčūżõå╦¤¤Ż¼▒Ūż╬Ų„┘|Ą─▓ĪēõŻ¼▒Ūż╬╩ųągż╩ż╔Ż¼ ╦¹ż╬ę╗░ŃĄ─ż╩įŁę“żŪżŽšh├„żŪżŁż╩żżŻ« ą──ĀĮ╗Ėą╔±ĮU╗ŁŽ±«É│ŻŻ©123 I-MIBG-źĘź¾ź┴ź░źķźšźŻ®`Ż® Ż©possible prodromal MSAź½źŲź┤źĻ®`ż╦▀mė├┐╔─▄Ż® ź╬źļźóź╔źņź╩źĻź¾ź╚źķź¾ź╣ź▌®`ź┐®`żõąĪ░¹┘A╩iż╦ė░Ēæż“ėļż© żļ╦a╬’Ż¼Ų„┘|Ą─ą─╝▓╗╝Ż¼╠Ū─“▓Īż╩ż╔ż╬ąĪŠČŠĆŠSź╦źÕ®`źĒźč ź┴®`ż╬ę╗░ŃĄ─ż╩įŁę“żŽ│²═Ōż╣żļŻ« ęĢų¬ęÖ─▄┴”ż╬įńŲ┌Ą═Ž┬ż“░ķż”ēõäėąįż╬šJų¬ÖC─▄Ż©Ī’Ż® ūóęŌ┴”?ęÖąčČ╚ż╬Ņćų°ż╩ēõäėż╚ęĢų¬ęÖ─▄┴”ż╬įńŲ┌Ą═Ž┬ż“ ░ķż”ēõäėąįż╬šJų¬ÖC─▄ į┘░kąįż╬╗├ęĢŻ©Ī’Ż® ░kųóż½żķ3─Ļęį─┌żŪŻ¼╦a╬’ż╦żĶż├żŲšTī¦żĄżņżŲżżż╩żżż│ż╚ šJų¬ųó ░kųóż½żķ3─Ļęį─┌żŪŻ¼DSM-Vż╦żĶżļŻ« Ž┬Ž“żŁ║╦╔ŽąįūóęĢ┬ķ»w Ž┬Ž“żŁ║╦╔ŽąįūóęĢ┬ķ»wż▐ż┐żŽ┤╣ų▒źĄź├ź½®`ź╔ż╬▀Wčė ┤·╠µį\ČŽż“╩Š╦¶ż╣żļŅ^▓┐MRI╦∙ęŖ PSPŻ¼ČÓ░kąįė▓╗»ųóŻ¼č¬╣▄ąįźč®`źŁź¾źĮź╦ź║źÓŻ¼ųó║“ąį ąĪ├Ś╝▓╗╝ż“│²═ŌŻ« ūį┬╔╔±ĮUšŽ║”Ż¼▀\äė╩¦š{ųóŻ¼źč®`źŁź¾źĮź╦ź║źÓż“ę²żŁŲż│ ż╣ż│ż╚ż¼ų¬żķżņżŲż¬żĻŻ¼╗╝š▀ż╬ųóū┤ż╚żŌż├ż╚żŌż╩ķv▀Bż¼żóżļż╚ ┐╝ż©żķżņżļ┤·╠µ╝▓╗╝ż╬ėø▌d ▀zü╗ąįż▐ż┐żŽųó║“ąįż╬▀\äė╩¦š{ųóżõźč®`źŁź¾źĮź╦ź║źÓż╩ ż╔Ż¼MSAŅÉ┐F╝▓╗╝Ż« Ī’MSAżŪżŌ│÷¼Fż╣żļż│ż╚ż¼żóżļżŌż╬ż╬Ż¼ į\ČŽż╬╠ž«ÉČ╚ż“┤_▒Żż╣żļż┐żßż╦ żóż©żŲ│²═ŌĒŚ─┐ż╦╝ėż©ż┐Ż« šJų¬ųóżŽMSAż╬į\ČŽż“ų¦│ųżĘż╩żż ĒŚ─┐żŪżóż├ż┐ż¼Ż¼░kųóŻ┤─ĻęįĮĄż╦ šJų¬ųóż“│╩żĘżŲżŌ│²═ŌżĄżņż╩żżŻ«
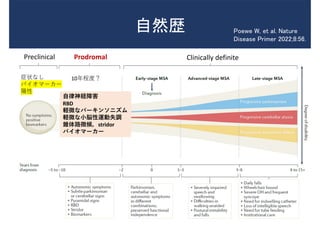
- 45. ūį╚╗Üs Preclinical Prodromal Clinically definite ųóū┤ż╩żĘ źąźżź¬ź▐®`ź½®` Ļ¢ąį 10─Ļ│╠Č╚Ż┐ Poewe W, et al. Nature Disease Primer 2022;8:56. ūį┬╔╔±ĮUšŽ║” RBD ▌X╬óż╩źč®`źŁź¾źĮź╦ź║źÓ ▌X╬óż╩ąĪ├Śąį▀\äė╩¦š{ ÕF╠Õ┬ĘÅš║“Ż¼stridor źąźżź¬ź▐®`ź½®`
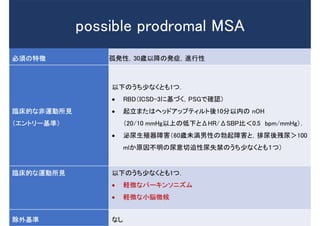
- 46. ▒žĒÜż╬╠žÅš ╣┬░kąįŻ¼30ÜręįĮĄż╬░kųóŻ¼▀Mąąąį ┼R┤▓Ą─ż╩ĘŪ▀\äė╦∙ęŖ Ż©ź©ź¾ź╚źĻ®`╗∙£╩Ż® ęįŽ┬ż╬ż”ż┴╔┘ż╩ż»ż╚żŌ1ż─Ż« ? RBDŻ©ICSD-3ż╦╗∙ż┼ż»Ż¼PSGżŪ┤_šJŻ® ? Ų┴óż▐ż┐żŽźžź├ź╔źóź├źūźŲźŻźļź╚ßß10Ęųęį─┌ż╬ nOH Ż©20/10 mmHgęį╔Žż╬Ą═Ž┬ż╚”żHR/”żSBP▒╚Ż╝0.5 bpm/mmHgŻ®Ż« ? ├┌─“╔·ų│Ų„šŽ║”Ż©60Ür╬┤£║─ąąįż╬▓¬ŲšŽ║”ż╚Ż¼┼┼─“ßß▓ą─“ŻŠ100 mlż½įŁę“▓╗├„ż╬─“ęŌŪąŲ╚ąį─“╩¦Į¹ż╬ż”ż┴╔┘ż╩ż»ż╚żŌŻ▒ż─Ż® ┼R┤▓Ą─ż╩▀\äė╦∙ęŖ ęįŽ┬ż╬ż”ż┴╔┘ż╩ż»ż╚żŌ1ż─Ż« ? ▌X╬óż╩źč®`źŁź¾źĮź╦ź║źÓ ? ▌X╬óż╩ąĪ├Ś╬ó║“ │²═Ō╗∙£╩ ż╩żĘ possible prodromal MSA
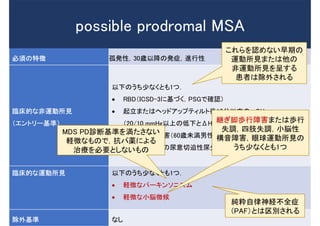
- 47. ▒žĒÜż╬╠žÅš ╣┬░kąįŻ¼30ÜręįĮĄż╬░kųóŻ¼▀Mąąąį ┼R┤▓Ą─ż╩ĘŪ▀\äė╦∙ęŖ Ż©ź©ź¾ź╚źĻ®`╗∙£╩Ż® ęįŽ┬ż╬ż”ż┴╔┘ż╩ż»ż╚żŌ1ż─Ż« ? RBDŻ©ICSD-3ż╦╗∙ż┼ż»Ż¼PSGżŪ┤_šJŻ® ? Ų┴óż▐ż┐żŽźžź├ź╔źóź├źūźŲźŻźļź╚ßß10Ęųęį─┌ż╬ nOH Ż©20/10 mmHgęį╔Žż╬Ą═Ž┬ż╚”żHR/”żSBP▒╚Ż╝0.5 bpm/mmHgŻ®Ż« ? ├┌─“╔·ų│Ų„šŽ║”Ż©60Ür╬┤£║─ąąįż╬▓¬ŲšŽ║”ż╚Ż¼┼┼─“ßß▓ą─“ŻŠ100 mlż½įŁę“▓╗├„ż╬─“ęŌŪąŲ╚ąį─“╩¦Į¹ż╬ż”ż┴╔┘ż╩ż»ż╚żŌŻ▒ż─Ż® ┼R┤▓Ą─ż╩▀\äė╦∙ęŖ ęįŽ┬ż╬ż”ż┴╔┘ż╩ż»ż╚żŌ1ż─Ż« ? ▌X╬óż╩źč®`źŁź¾źĮź╦ź║źÓ ? ▌X╬óż╩ąĪ├Ś╬ó║“ │²═Ō╗∙£╩ ż╩żĘ possible prodromal MSA ż│żņżķż“šJżßż╩żżįńŲ┌ż╬ ▀\äė╦∙ęŖż▐ż┐żŽ╦¹ż╬ ĘŪ▀\äė╦∙ęŖż“│╩ż╣żļ ╗╝š▀żŽ│²═ŌżĄżņżļ ╝ā╗éūį┬╔╔±ĮU▓╗╚½ųó Ż©PAFŻ®ż╚żŽŪ°äeżĄżņżļ MDS PDį\ČŽ╗∙£╩ż“£║ż┐żĄż╩żż ▌X╬óż╩żŌż╬żŪŻ¼┐╣źč╦aż╦żĶżļ ų╬»¤ż“▒žę¬ż╚żĘż╩żżżŌż╬ Š@ż«Į┼ÜiąąšŽ║”ż▐ż┐żŽÜiąą ╩¦š{Ż¼╦─ų½╩¦š{Ż¼ąĪ├Śąį śŗ궚Ž║”Ż¼č█Ū“▀\äė╦∙ęŖż╬ ż”ż┴╔┘ż╩ż»ż╚żŌ1ż─
- 50. į\ČŽ╗∙£╩ż╬Ž▐Įń ? ĖąČ╚?╠ž«ÉČ╚ż¼▓╗├„Ż« ? ╦¹ż╬źč®`źŁź¾źĮź╦ź║źÓżõ look-alike/mimicsż“ż╔żņż└ż▒ │²═ŌżŪżŁżļż½▓╗├„Ż« Ī· Į±ß߯¼Ś╩į^įć“Yż¼ąąż’żņżļŻ« ? mono-system atrophy ż╬į\ČŽż¼żŪżŁż╩żżŻ« ? ĘŪĄõą═Ą─MSAż╬į\ČŽż¼żŪżŁż╩żżŻ©MDS PSP criteriaż╦ ż¬ż▒żļ«Éą═ųó║“╚║ż¼įOż▒żķżņżŲżżż╩żżŻ®Ż«
- 51. į\ČŽ╗∙£╩ż╦Æ„▌dżĄżņż┐ ų¦│ųĄ─źąźżź¬ź▐®`ź½®`░Ė 1. possible prodromal MSAż╬Ņ^▓┐MRIź▐®`ź½®` 2. Ņ^▓┐FDG-PET 3. ą──Ā123I-MIBG źĘź¾ź┴ź░źķźšźŻ®` 4. PSGżŪ┤_šJżĄżņż┐RBD 5. č÷┼P╬╗10Ęųßßż╬č¬Ø{ź╬źļź©źįź═źšźĻź¾éÄĪ’ 6. ź”źĒź└źżź╩ź▀ź»ź╣Ś╩¢╦Ż©ģ¦┐s▓╗╚½ż“░ķż”┼┼─“▀^╗Ņäėż╩żżżĘ┼┼─“└©╝sĮŅģfš{▓╗╚½Ż® 7. ═ŌĖžķT└©╝sĮŅż╬═¼ą─āęßśĮŅļŖćĒ 8. ├Ś╝╣¾lę║ųąż╬”┴-źĘź╠ź»źņźżź¾ź¬źĻź┤ź▐®`Ż©PMCAż▐ż┐żŽRT-QUICĘ©Ż® Ī’ 9. ├Ś╝╣¾lę║?č¬Ø{ųąż╬ź╦źÕ®`źĒźšźŻźķźßź¾ź╚▌XµiŻ©│¼Ė▀ĖąČ╚ELISAŻ® Ī’
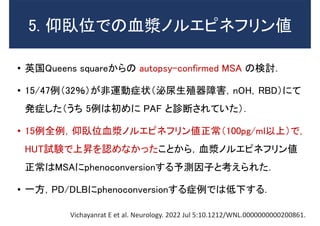
- 52. 5. č÷┼P╬╗żŪż╬č¬Ø{ź╬źļź©źįź═źšźĻź¾éÄ ? ėó╣·Queens squareż½żķż╬ autopsy-confirmed MSA ż╬Ś╩ėæŻ« ? 15/47└²Ż©32ŻźŻ®ż¼ĘŪ▀\äėųóū┤Ż©├┌─“╔·ų│Ų„šŽ║”Ż¼nOHŻ¼RBDŻ®ż╦żŲ ░kųóżĘż┐Ż©ż”ż┴ 5└²żŽ│§żßż╦ PAF ż╚į\ČŽżĄżņżŲżżż┐Ż®Ż« ? 15└²╚½└²Ż¼č÷┼P╬╗č¬Ø{ź╬źļź©źįź═źšźĻź¾éÄš²│ŻŻ©100pg/mlęį╔ŽŻ®żŪŻ¼ HUTįć“YżŪ╔ŽĢNż“šJżßż╩ż½ż├ż┐ż│ż╚ż½żķŻ¼č¬Ø{ź╬źļź©źįź═źšźĻź¾éÄ š²│ŻżŽMSAż╦phenoconversionż╣żļėĶ£yę“ūėż╚┐╝ż©żķżņż┐Ż« ? ę╗ĘĮŻ¼PD/DLBż╦phenoconversionż╣żļųó└²żŪżŽĄ═Ž┬ż╣żļŻ« Vichayanrat E et al. Neurology. 2022 Jul 5:10.1212/WNL.0000000000200861.
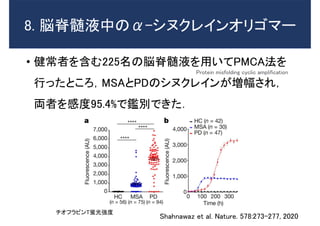
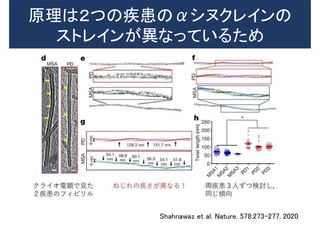
- 53. 8. ├Ś╝╣¾lę║ųąż╬”┴-źĘź╠ź»źņźżź¾ź¬źĻź┤ź▐®` ? ĮĪ│Żš▀ż“║¼żÓ225├¹ż╬├Ś╝╣¾lę║ż“ė├żżżŲPMCAĘ©ż“ ąąż├ż┐ż╚ż│żĒŻ¼MSAż╚PDż╬źĘź╠ź»źņźżź¾ż¼ēłĘ∙żĄżņŻ¼ üIš▀ż“ĖąČ╚95.4%żŪĶaäeżŪżŁż┐Ż« Shahnawaz et al. Nature. 578:273-277, 2020 ź┴ź¬źšźķźėź¾T═w╣ŌÅŖČ╚ Protein misfolding cyclic amplification
- 54. įŁ└ĒżŽŻ▓ż─ż╬╝▓╗╝ż╬”┴źĘź╠ź»źņźżź¾ż╬ ź╣ź╚źņźżź¾ż¼«Éż╩ż├żŲżżżļż┐żß Shahnawaz et al. Nature. 578:273-277, 2020
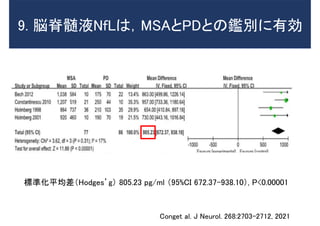
- 55. 9. ├Ś╝╣¾lę║NfLżŽŻ¼MSAż╚PDż╚ż╬Ķaäeż╦ėąä┐ ś╦£╩╗»ŲĮŠ∙▓ŅŻ©HodgesĪ»gŻ® 805.23 pg/ml Ż©95%CI 672.37-938.10Ż®, P<0.00001 Conget al. J Neurol. 268:2703-2712, 2021
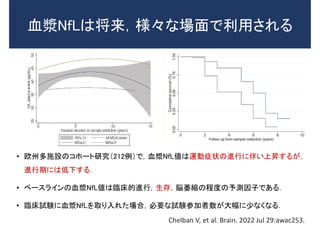
- 56. č¬Ø{NfLżŽĮ½└┤Ż¼śöĪ®ż╩ł÷├µżŪ└¹ė├żĄżņżļ ? ┼Ęų▌ČÓ╩®įOż╬ź│ź█®`ź╚蹊┐Ż©212└²Ż®żŪŻ¼č¬Ø{NfLéÄżŽ▀\äėųóū┤ż╬▀Mąąż╦░ķżż╔ŽĢNż╣żļż¼Ż¼ ▀MąąŲ┌ż╦żŽĄ═Ž┬ż╣żļŻ« ? ź┘®`ź╣źķźżź¾ż╬č¬Ø{NfLéÄżŽ┼R┤▓Ą─▀MąąŻ¼╔·┤µŻ¼├Ś╬«┐sż╬│╠Č╚ż╬ėĶ£yę“ūėżŪżóżļŻ« ? ┼R┤▓įć“Yż╦č¬Ø{NfLż“╚ĪżĻ╚ļżņż┐ł÷║ŽŻ¼▒žę¬ż╩įć“Y▓╬╝ėš▀╩²ż¼┤¾Ę∙ż╦╔┘ż╩ż»ż╩żļŻ« Chelban V, et al. Brain. 2022 Jul 29:awac253.
- 57. ? ą┬į\ČŽ╗∙£╩żŽį\ČŽż╬┤_īgąįż“ 4źņź┘źļż╦Ęųż▒żŲČ©┴xżĘ żŲżżżļż¼Ż¼lexicon ż╦ėø▌dżĄżņżŲżżżļĖ„╦∙ęŖż╬Č©┴xż“żĶż» ┤_šJżĘżŲį\ČŽż“ąąż”Ż« ? possible prodromal MSAżŽäō╦aż╬ż┐żßż╦▒žę¬ż╩▓Ī│§Ų┌ ż╬╗╝š▀ż“ęŖ│÷ż╣─┐Ą─żŪįOČ©żĄżņżŲż¬żĻŻ¼źąźżź¬ź▐®`ź½®` ż╬░kęŖ?┤_┴óż╦żĶżĻŻ¼Į±ß߯¼┤¾żŁż»ēõĖ³żĄżņżļŻ« ąĪ└©Ż▓
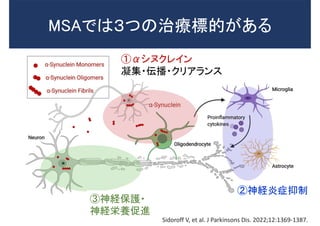
- 59. MSAżŪżŽŻ│ż─ż╬ų╬»¤ś╦Ą─ż¼żóżļ ó┘”┴źĘź╠ź»źņźżź¾ ─²╝»?ü╗▓ź?ź»źĻźóźķź¾ź╣ ó█╔±ĮU▒Żūo? ╔±ĮU¢čB┤┘▀M ó┌╔±ĮUčūųóęųųŲ Sidoroff V, et al. J Parkinsons Dis. 2022;12:1369-1387.
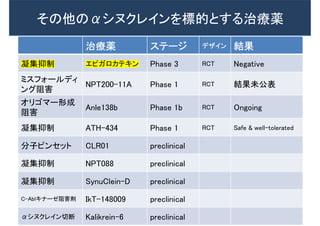
- 61. ó┘ ”┴źĘź╠ź»źņźżź¾ż“ś╦Ą─ż╚ż╣żļų╬»¤ ÖCą“ ų╬»¤╦a ź╣źŲ®`źĖ źŪźČźżź¾ ĮY╣¹ ź’ź»ź┴ź¾ PD01A/PD03A Ż©ź’ź»ź┴ź¾Ż® Phase 1 RCT Safe & well-tolerated ”┴źĘź╠ź»źņźżź¾┐╣╠Õ Lu AF82422 Phase 1 RCT Safe & well-tolerated źóź¾ź┴ź╗ź¾ź╣ BIIB 101 Phase 1 RCT Ongoing ĘųĮŌ┤┘▀M źĻźšźĪź¾źįźĘź¾ Phase 3 RCT įńŲ┌ųąų╣Ż©¤o굹įŻ® ĘųĮŌ┤┘▀M źĻź┴ź”źÓ Phase 2 RCT įńŲ┌ųąų╣Ż©Ė▒ū„ė├Ż® ? ”┴źĘź╠ź»źņźżź¾ż╦īØż╣żļ├Ōę▀»¤Ę©ż╦żŽŻ¼ź’ź»ź┴ź¾ż╦żĶżļ─▄äė├Ōę▀»¤Ę©ż╚Ż¼ ┐╣╠Õż“═Čėļż╣żļ╩▄äė├Ōę▀»¤Ę©ż¼┤µį┌ż╣żļŻ« ? ź’ź»ź┴ź¾żŪżŽBBBż“═©▀^ż╣żļ”┴źĘź╠ź»źņźżź¾┐╣╠Õż╬«b╔·ż¼┤_šJżĄżņż┐Ż«
- 62. ó┘ ”┴źĘź╠ź»źņźżź¾ż“ś╦Ą─ż╚ż╣żļų╬»¤ ÖCą“ ų╬»¤╦a ź╣źŲ®`źĖ źŪźČźżź¾ ĮY╣¹ ź’ź»ź┴ź¾ PD01A/PD03A Ż©ź’ź»ź┴ź¾Ż® Phase 1 RCT Safe & well-tolerated ”┴źĘź╠ź»źņźżź¾┐╣╠Õ Lu AF82422 Phase 1 RCT Safe & well-tolerated źóź¾ź┴ź╗ź¾ź╣ BIIB 101 Phase 1 RCT Ongoing ĘųĮŌ┤┘▀M źĻźšźĪź¾źįźĘź¾ Phase 3 RCT įńŲ┌ųąų╣Ż©¤o굹įŻ® ĘųĮŌ┤┘▀M źĻź┴ź”źÓ Phase 2 RCT įńŲ┌ųąų╣Ż©Ė▒ū„ė├Ż® ? ”┴źĘź╠ź»źņźżź¾ż╦īØż╣żļ├Ōę▀»¤Ę©ż╦żŽŻ¼ź’ź»ź┴ź¾ż╦żĶżļ─▄äė├Ōę▀»¤Ę©ż╚Ż¼ ┐╣╠Õż“═Čėļż╣żļ╩▄äė├Ōę▀»¤Ę©ż¼┤µį┌ż╣żļŻ« ? ź’ź»ź┴ź¾żŪżŽBBBż“═©▀^ż╣żļ”┴źĘź╠ź»źņźżź¾┐╣╠Õż╬«b╔·ż¼┤_šJżĄżņż┐Ż«
- 63. ? Ą┌Ż▓ŽÓ┼R┤▓įć“YŻ©źļź¾ź╔ź┘ź├ź»Ż® ? źķź¾ź└źÓ╗»Ż¼Č■ųž├żŚ╩Ż¼üKąą╚║ķgŻ¼ źūźķź╗ź▄īØššŻ¼ČÓ╩®įO╣▓═¼įć“Y ? ├ū╣·?╚š▒Šż½żķ60├¹ż╬╗╝š▀Ż©īg╦a40├¹Ż¼é╬╦a20├¹Ż® ? 40Üręį╔Ž75ÜręįŽ┬Ż¼░kųóż½żķ5─Ļ╬┤£║ ? ų╬»¤Ų┌ķgŻ║48Ī½72▀Lķg ? ╣·┴ó▓Īį║ÖCśŗ╬„ČÓ┘R▓Īį║Ż¼╠┘╠’ęĮ┐Ų┤¾č¦Ż¼ß¬ĖĘ┤¾č¦ AMULET study A Study of Lu AF82422 in Participants With Multiple System Atrophy
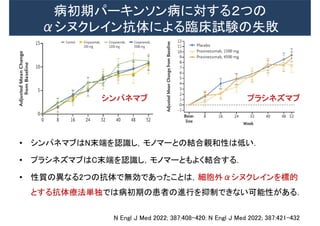
- 64. ▓Ī│§Ų┌źč®`źŁź¾źĮź¾▓Īż╦īØż╣żļŻ▓ż─ż╬ ”┴źĘź╠ź»źņźżź¾┐╣╠Õż╦żĶżļ┼R┤▓įć“Yż╬╩¦öĪ N Engl J Med 2022; 387:408-420: N Engl J Med 2022; 387:421-432 ? źĘź¾źčź═ź▐źųżŽN─®Č╦ż“šJūRżĘŻ¼źŌź╬ź▐®`ż╚ż╬ĮY║ŽėH║═ąįżŽĄ═żżŻ« ? źūźķźĘź═ź║ź▐źųżŽC─®Č╦ż“šJūRżĘŻ¼źŌź╬ź▐®`ż╚żŌżĶż»ĮY║Žż╣żļŻ« ? ąį┘|ż╬«Éż╩żļ2ż─ż╬┐╣╠ÕżŪ¤oä┐żŪżóż├ż┐ż│ż╚żŽŻ¼╝Ü░¹═Ō”┴źĘź╠ź»źņźżź¾ż“ś╦Ą─ ż╚ż╣żļ┐╣╠Õ»¤Ę©ģgČ└żŪżŽ▓Ī│§Ų┌ż╬╗╝š▀ż╬▀Mąąż“ęųųŲżŪżŁż╩żż┐╔─▄ąįż¼żóżļŻ« źĘź¾źčź═ź▐źų źūźķźĘź═ź║ź▐źų
- 65. ╩¦öĪż½żķ║╬ż“覿ųż½Ż┐ Front Mol Neurosci. 2019;12:299. Neuropathol Appl Neurobiol. 2021;47:268-282 ? ░kųóŪ░żŌżĘż»żŽŪ░±lųóū┤Ų┌ż╦ų╬»¤Įķ╚ļż“ ąąż”▒žę¬ż¼żóżļ. ©C Ė∙Æćż╚żĘżŲMSAė╔└┤╔±ĮUŪ░±l╝Ü░¹ż“ė├żżż┐ 蹊┐żŪŻ¼”┴źĘź╠ź»źņźżź¾ż¼╝Ü░¹║╦ż╦ęŲąąż╣żļż╬ żŽįńŲ┌ż╬źżź┘ź¾ź╚ż╚żżż”ł¾Ėµż¼żóżļŻ« ? żŌżĘż»żŽ╝Ü░¹─┌”┴źĘź╠ź»źņźżź¾ż╦Ė╔£hż╣żļ źżź¾ź╚źķź▄źŪźŻ®`Ż©╝Ü░¹─┌░k¼F┐╣╠ÕŻ®ż“ ķ_░kż╣żļ▒žę¬ż¼żóżļŻ«
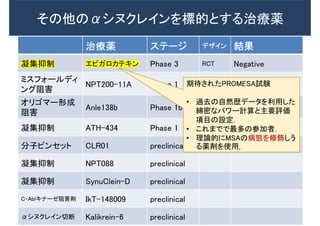
- 66. ų╬»¤╦a ź╣źŲ®`źĖ źŪźČźżź¾ ĮY╣¹ ─²╝»ęųųŲ ź©źįź¼źĒź½źŲźŁź¾ Phase 3 RCT Negative ź▀ź╣źšź®®`źļźŪźŻ ź¾ź░ūĶ║” NPT200-11A Phase 1 RCT ĮY╣¹╬┤╣½▒Ē ź¬źĻź┤ź▐®`ą╬│╔ ūĶ║” Anle138b Phase 1b RCT Ongoing ─²╝»ęųųŲ ATH-434 Phase 1 RCT Safe & well-tolerated Ęųūėźįź¾ź╗ź├ź╚ CLR01 preclinical ─²╝»ęųųŲ NPT088 preclinical ─²╝»ęųųŲ SynuClein-D preclinical C-AblźŁź╩®`ź╝ūĶ║”äł IkT-148009 preclinical ”┴źĘź╠ź»źņźżź¾ŪąČŽ Kalikrein-6 preclinical żĮż╬╦¹ż╬”┴źĘź╠ź»źņźżź¾ż“ś╦Ą─ż╚ż╣żļų╬»¤╦a
- 67. ų╬»¤╦a ź╣źŲ®`źĖ źŪźČźżź¾ ĮY╣¹ ─²╝»ęųųŲ ź©źįź¼źĒź½źŲźŁź¾ Phase 3 RCT Negative ź▀ź╣źšź®®`źļźŪźŻ ź¾ź░ūĶ║” NPT200-11A Phase 1 RCT ĮY╣¹╬┤╣½▒Ē ź¬źĻź┤ź▐®`ą╬│╔ ūĶ║” Anle138b Phase 1b RCT Ongoing ─²╝»ęųųŲ ATH-434 Phase 1 RCT Safe & well-tolerated Ęųūėźįź¾ź╗ź├ź╚ CLR01 preclinical ─²╝»ęųųŲ NPT088 preclinical ─²╝»ęųųŲ SynuClein-D preclinical C-AblźŁź╩®`ź╝ūĶ║”äł IkT-148009 preclinical ”┴źĘź╠ź»źņźżź¾ŪąČŽ Kalikrein-6 preclinical żĮż╬╦¹ż╬”┴źĘź╠ź»źņźżź¾ż“ś╦Ą─ż╚ż╣żļų╬»¤╦a Ų┌┤²żĄżņż┐PROMESAįć“Y ? ▀^╚źż╬ūį╚╗ÜsźŪ®`ź┐ż“└¹ė├żĘż┐ Šd├▄ż╩źčź’®`ėŗ╦Ńż╚ų„ę¬įuü² ĒŚ─┐ż╬įOČ©Ż« ? ż│żņż▐żŪżŪūŅČÓż╬▓╬╝ėš▀Ż« ? └ĒšōĄ─ż╦MSAż╬▓ĪæBż“ą▐’ŚżĘż” żļ╦aäłż“╩╣ė├Ż«
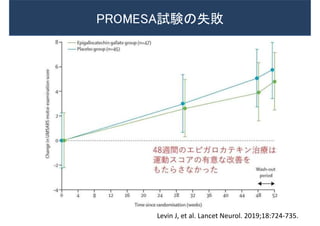
- 68. PROMESAįć“Yż╬╩¦öĪ Levin J, et al. Lancet Neurol. 2019;18:724-735.
- 69. PROMESAįć“Yż╬╩¦öĪż½żķ覿ųż┘żŁżŌż╬Ż©ų°š▀żķŻ® ? ĘŪ▀\äėųóū┤ż“║¼żÓūŅ▀mż╩ź©ź¾ź╔ź▌źżź¾ź╚ż╬øQČ© ? įńŲ┌į\ČŽż╚ų╬»¤ä┐╣¹┼ąČ©ż╬ż┐żßż╬źąźżź¬ź▐®`ź½®` ? ▀zü╗Ą─ę¬ę“żõżĶżĻįö╝Üż╩▓ĪæBż╬ĮŌ├„ ? ķg▀`ż├żŲżżżļ┐╔─▄ąįż╬żóżļ▓ĪæBüóšhż╦╗∙ż┼ż½ż╩żż Ū░┼R┤▓źŌźŪźļż╬śŗ║BŻ©└²ż©żąiPS╝Ü░¹źŌźŪźļż╬żĶż”ż╩ ╗╝š▀ė╔└┤ż╬źŌźŪźļŻ® Levin J, et al. Lancet Neurol. 2019;18:724-735.
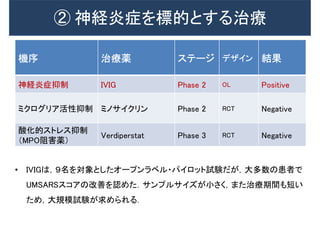
- 70. ó┌ ╔±ĮUčūųóż“ś╦Ą─ż╚ż╣żļų╬»¤ ÖCą“ ų╬»¤╦a ź╣źŲ®`źĖ źŪźČźżź¾ ĮY╣¹ ╔±ĮUčūųóęųųŲ IVIG Phase 2 OL Positive ź▀ź»źĒź░źĻźó╗ŅąįęųųŲ ź▀ź╬źĄźżź»źĻź¾ Phase 2 RCT Negative ╦ß╗»Ą─ź╣ź╚źņź╣ęųųŲ Ż©MPOūĶ║”╦aŻ® Verdiperstat Phase 3 RCT Negative ? IVIGżŽŻ¼Ż╣├¹ż“īØŽ¾ż╚żĘż┐ź¬®`źūź¾źķź┘źļ?źčźżźĒź├ź╚įć“Yż└ż¼Ż¼┤¾ČÓ╩²ż╬╗╝š▀żŪ UMSARSź╣ź│źóż╬Ė─╔Ųż“šJżßż┐Ż«źĄź¾źūźļźĄźżź║ż¼ąĪżĄż»Ż¼ż▐ż┐ų╬»¤Ų┌ķgżŌČ╠żż ż┐żßŻ¼┤¾ęÄ─Żįć“Yż¼Ū¾żßżķżņżļŻ«
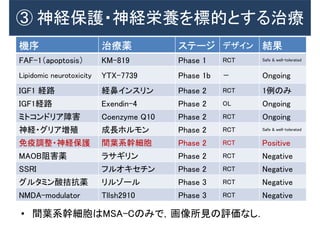
- 71. ó█ ╔±ĮU▒Żūo?╔±ĮU¢čBż“ś╦Ą─ż╚ż╣żļų╬»¤ ÖCą“ ų╬»¤╦a ź╣źŲ®`źĖ źŪźČźżź¾ ĮY╣¹ FAF-1Ż©apoptosisŻ® KM-819 Phase 1 RCT Safe & well-tolerated Lipidomic neurotoxicity YTX-7739 Phase 1b ŻŁ Ongoing IGF1 ĮU┬Ę ĮU▒Ūźżź¾ź╣źĻź¾ Phase 2 RCT 1└²ż╬ż▀ IGF1ĮU┬Ę Exendin-4 Phase 2 OL Ongoing ź▀ź╚ź│ź¾ź╔źĻźóšŽ║” Coenzyme Q10 Phase 2 RCT Ongoing ╔±ĮU?ź░źĻźóēłų│ │╔ķLź█źļźŌź¾ Phase 2 RCT Safe & well-tolerated ├Ōę▀š{š¹?╔±ĮU▒Żūo ķg╚~ŽĄÄų╝Ü░¹ Phase 2 RCT Positive MAOBūĶ║”╦a źķźĄź«źĻź¾ Phase 2 RCT Negative SSRI źšźļź¬źŁź╗ź┴ź¾ Phase 2 RCT Negative ź░źļź┐ź▀ź¾╦ß▐ū┐╣╦a źĻźļźŠ®`źļ Phase 3 RCT Negative NMDA-modulator Tllsh2910 Phase 3 RCT Negative ? ķg╚~ŽĄÄų╝Ü░¹żŽMSA-Cż╬ż▀żŪŻ¼╗ŁŽ±╦∙ęŖż╬įuü²ż╩żĘŻ«
- 72. ? ų╬»¤æķ┬įż╚żĘżŲŻ¼ó┘”┴źĘź╠ź»źņźżź¾Ż¼ó┌╔±ĮUčūųóż╬ęųųŲŻ¼ ó█╔±ĮU▒Żūo?╔±ĮU¢čBż╬┤┘▀Mż¼żóżļŻ« ? MSAż╦ż¬żżżŲŻ¼”┴źĘź╠ź»źņźżź¾┐╣╠Õż╬ä┐╣¹ż“įuü²ż╣żļ │§żßżŲż╬╣·ļHų╬“Yż¼▀MąąųążŪżóżļŻ« ? ┼R┤▓įć“Yż╬╩¦öĪż½żķ覿ėŻ¼æķ┬įż“┐╝ż©żļż│ż╚ż¼ųžę¬żŪ żóżļŻ« ąĪ└©Ż│
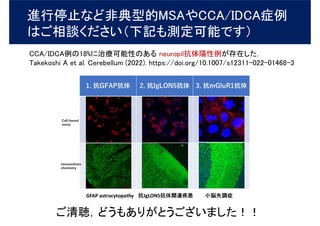
- 73. ▀Mąą═Żų╣ż╩ż╔ĘŪĄõą═Ą─MSAżõCCA/IDCAųó└² żŽż┤ŽÓšäż»ż└żĄżżŻ©Ž┬ėøżŌ£yČ©┐╔─▄żŪż╣Ż® CCA/IDCA└²ż╬18%ż╦ų╬»¤┐╔─▄ąįż╬żóżļ neuropil┐╣╠ÕĻ¢ąį└²ż¼┤µį┌żĘż┐Ż« Takekoshi A et al. Cerebellum (2022). https://doi.org/10.1007/s12311-022-01468-3 ż┤ŪÕ┬ŚŻ¼ż╔ż”żŌżóżĻż¼ż╚ż”ż┤żČżżż▐żĘż┐ŻĪŻĪ