







![Angiosome
• Toàn cơ thể: 40
• Vùng cổ - bàn chân: 6
11
Taylor GI, Palmer JH. The vascular territories [angiosomes] of the body:
experimental study and clinical applications. Br J Plast Surg. 1987;40:113](https://image.slidesharecdn.com/daodanhvinhcli-180811103509/85/Daodanhvinh-cli-11-320.jpg)

























































More Related Content
Similar to Daodanhvinh cli (20)
More from nguyenngat88 (20)


















Daodanhvinh cli
- 1. Can thiệp nội mạch điêu trị thiếu máu chi trầm trọng Bs. Đào Danh Vĩnh Depart of Radiology Bach Mai hospital 1
- 2. Nội dung • Giới thiệu • Phân vùng cấp máu (angiosome) • Nong bóng thường (POBA) • Bóng phủ thuốc (DEB) • Đặt khung giá đỡ (stent) 2
- 3. Giới thiệu • Thiếu máu chi trầm trọng (CLI) là giai đoạn cuối của bệnh động mạch ngoại vi (PAD) • Đặc trưng: • Lâm sàng: đau khi nghỉ/loét/hoại thư • Tổn thương ĐM: vùng BTK, nhiều tầng • Tổn thương phối hợp: ĐM vành, ĐM não • Tiên lượng sau 5 năm: • Tử vong 50 % • Cắt cụt chi mở rộng: 30% • Toàn vẹn chi: 20% 3 Eur J Vasc Endovasc Surg Vol 33, Supplement 1, 2007
- 4. 4
- 5. Giới thiệu Cắt cụt chi không phải là lựa chọn ưu tiên ! 5 Norgren L et al. Eur J Vasc Endovasc Surg Vol 33, Supplement 1, 2007
- 6. Giới thiệu Khuyến cáo từ TACE 2 6 Norgren L et al. Eur J Vasc Endovasc Surg Vol 33, Supplement 1, 2007
- 7. Giới thiệu Mục tiêu cơ bản trong điều trị CLI: • Giảm đau do thiếu máu • Liền vết loét do thiếu máu • Ngăn ngừa mất đoạn chi • Cải thiện chất lượng sống • Kéo dài thời gian sống 7 Norgren L et al. Eur J Vasc Endovasc Surg Vol 33, Supplement 1, 2007
- 8. Giới thiệu • Can thiệp nội mạch: • Chỉ định /chống chỉ định • Phục hồi dòng chảy đến tổn thương: trực tiếp / gián tiếp • ĐM đích cần can thiệp: vị trí/ số lượng • Thành công: kỹ thuật, lâm sàng • Điều trị bổ trợ sau can thiệp 8
- 9. Nội dung • Giới thiệu • Phân vùng cấp máu (angiosome) • Nong bóng thường (POBA) • Bóng phủ thuốc (DEB) • Sử dụng khung giá đỡ (stent) 9
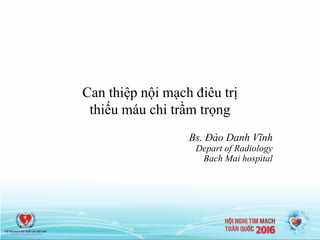
- 10. Angiosome • Phân vùng cấp máu (Angiosome): vùng mô được cấp máu bởi một nguồn ĐM nhất định • Taylor (1987): giới thiệu lần đầu • Attinger (1997): bơm dung dịch mầu xác định vùng cấp máu • Sự tương quan giữa tổn thương động mạch với tổn thương mô tương ứng 10 Attinger C. Vascular anatomy of the foot and ankle. Oper Tech Plast Reconstr Surg 1997;4:183
- 11. Angiosome • Toàn cơ thể: 40 • Vùng cổ - bàn chân: 6 11 Taylor GI, Palmer JH. The vascular territories [angiosomes] of the body: experimental study and clinical applications. Br J Plast Surg. 1987;40:113
- 12. Angiosome • Tái thông mạch: Angiosome vs. Non Angiosome 12 Alexandrescu et al. J Endovasc Ther 2011;18:376
- 13. • Tái thông mạch: Angiosome vs. Non Angiosome Angiosome 13 Tác giả Năm N Endpoint Trực tiếp Gián tiếp Attinger et al 2006 56 Tổn thương không liền 9% 38% Iidia et all 2010 203 Bảo tồn chi 86% 69% Valera et all 2010 76 Liền vết loét 92% 73% Iidia et all 2012 369 Bảo tồn chi (Rutherford III) 49% 29% Các kết quả nghiên cứu cho thấy tỷ lệ thành công về lâm sàng (bảo tồn chi) tốt hơn rõ rệt ở nhóm phục hồi tuần hoàn trực tiếp đến tổn thương
- 14. Nội dung • Giới thiệu • Phân vùng cấp máu (angiosome) • Nong bóng thường (POBA) • Bóng phủ thuốc (DEB) • Sử dụng khung giá đỡ (stent) 14
- 15. POBA • Kỹ thuật cơ bản và phổ biến nhất hiện nay • Mục tiêu chính (primary goal): bảo tồn chi • Chiến lược: – Xử lý inflow trước – Tiếp cận xuôi dòng – Phục hồi dòng chảy trực tiếp – Phục hồi được ít nhất một ĐM cấp máu đến cung gan chân 15
- 16. POBA Khó khăn, thách thức:  Tổn thương lan toả, nhiều tầng  Vùng hạ lưu tưới máu kém  Xơ vữa vôi hoá  Khó đi qua được tổn thương  Mạch nhỏ (2-3mm), dễ vỡ  Tái hẹp sau can thiệp (vessel re-coil)  Co thắt, tắc mạch 16
- 17. POBA 17
- 18. POBA Sau 7 ngày
- 19. • Khi tiếp cận trong lòng / xuôi dòng thất bại POBA 19
- 20. POBA • 634 bệnh nhân CLI (101 BTK only) • Tuổi trung bình: 65 • Rutherford: 5-6 • Chiều dài tổn thương trung bình: 21cm • Theo dõi 3 năm sau can thiệp 20 European Society for Vascular Surgery 2008
- 21. POBA 21 • Nhược điểm lớn nhất của POBA trong CLI: Tái hẹp & Tái phát • Cần giải pháp bổ trợ để cải thiện: – DEB (drug - eluting balloon) – BMS (bare metallic stent) – DES (drug-eluting stent) – Bio-absorbable stent, atherectomy device, cryoplasty, laser….
- 22. Nội dung • Giới thiệu • Phân vùng cấp máu (angiosome) • Nong bóng thường (POBA) • Bóng phủ thuốc (DEB) • Sử dụng khung giá đỡ (stent) 22
- 23. DEB 23 • Tầng trên gối (ATK): hiệu quả của DEB đã được khẳng định • Tầng dưới gối (BTK): – Lần đầu (2011): Schmidt A. – Sử dụng Paclitaxel – Nhiều sản phẩm trên thị trường: IN.PACT Amphirion, Lutonix, Passeo Lux… – Nhiều nghiên cứu lâm sàng Schmidt A et al. J Am Coll Cardiol. 2011 Sep 6;58(11):1105-9
- 24. DEB 24 1.F.Fanelli et al. JEVT 2012;19:571–580 2.A.Cioppa – EuroPCR 2012 3.F.Liistro – TCT 2012 2011 4. K.Suzuki – LINC Asia Pacific 2012 5. A.Schmidt et al. J Am Coll Cardiol 2011;58:1105– 9
- 26. DEB 26 J Am Coll Cardiol 2014;64:1568-76
- 27. Nội dung • Giới thiệu • Phân vùng cấp máu (angiosome) • Nong bóng thường (POBA) • Bóng phủ thuốc (DEB) • Sử dụng khung giá đỡ (stent) 27
- 28. • Stent thường (BMS) / stent phủ thuốc (DES) • DES: sirolimus / everolimus • Thường áp dụng với những tổn thương khu trú (<10cm), đoạn gần (1/3 trên - giữa cẳng chân) – CLI: tổn thương lan toả – BTK: đường kính mạch nhỏ 2-3mm • Nhiều nghiên cứu lâm sàng nhưng tiêu chuẩn lựa chọn chặt chẽ Đặt stent 28 From: Siablis D. JAmColl Cardiol Intv 2014;7:1048–56.
- 29. Đặt stent BMS vs. POBA 29 Sau 1 năm, không có sự khác biệt về lưu thông, bảo tồn chi, thời gian sống sau can thiệp giữa nhóm POBA và nhóm BMS
- 30. Đặt stent DES vs. POBA 30 Andrew J. Feiring 2011
- 31. Đặt stent DES vs. POBA 31 Andrew J. Feiring 2011
- 32. • Số nghiên cứu RCTs: 5 • Số bệnh nhân BTK: N = 611 (DES vs. POBA / BMS) • Thời gian theo dõi trung bình 12 tháng • Chiều dài tổn thương: 18-30mm Đặt stent 32 J Am Coll Cardiol Intv. 2013;6(12):1284-1293
- 33. • Số nghiên cứu RCTs: 5 • Số bệnh nhân CLI: 611(DES vs. POBA / BMS) • Thời gian theo dõi trung bình 12 tháng • Chiều dài tổn thương: 18-30mm Đặt stent 33 J Am Coll Cardiol Intv. 2013;6(12):1284-1293
- 34. • Số nghiên cứu RCTs: 5 • Số bệnh nhân CLI: 611(DES vs. POBA / BMS) • Thời gian theo dõi trung bình 12 tháng • Chiều dài tổn thương: 18-30mm Đặt stent 34 J Am Coll Cardiol Intv. 2013;6(12):1284-1293
- 35. • Số nghiên cứu RCTs: 5 • Số bệnh nhân CLI: 611(DES vs. POBA / BMS) • Thời gian theo dõi trung bình 12 tháng • Chiều dài tổn thương: 18-30mm Đặt stent 35 J Am Coll Cardiol Intv. 2013;6(12):1284-1293
- 36. 36
- 37. Kết luận • Bệnh nhân CLI đặc trưng bằng tổn thương động mạch đa tầng, trong đó đặc biệt là tầng dưới gối. • Cần có sự phối hợp nhiều chuyên khoa trong kiểm soát, điều trị • Mục tiêu điều trị cơ bản là hàn gắn vết loét và bảo tồn chi • Nong tạo hình ĐM qua da bằng bóng thường (POBA) là phương pháp điều trị tái thông cơ bản và phổ biến nhất hiện nay. • Các kỹ thuật mới, chi phí cao (DEB, DES…) được chỉ định trong những trường hợp cụ thể, chặt chẽ và cần thêm bằng chứng lâm sàng. 37
- 38. Trân trọng cảm ơn ! 38