

































































































































































































































































































More Related Content
What's hot (20)
Viewers also liked (20)


















Similar to Feraboli 2 (20)




















Feraboli 2
- 1. Divisione di Ortopedia e Traumatologia Azienda Ospedaliera di Cremona
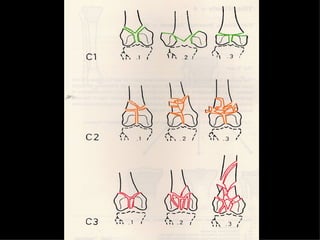
- 2. A B C Distal femoral fractures type C Choosing the right strategy and the right implant
- 4. La placca a compressione percutanea (PC.C.P.) di Gotfried ÃĻ un mezzo di sintesi studiato per assicurare un âimpattamento controllatoâ delle fratture pertrocanteriche grazie alle due viti telescopiche prossimali che garantiscono una ottima stabilità rotazionale
- 5. Ėý
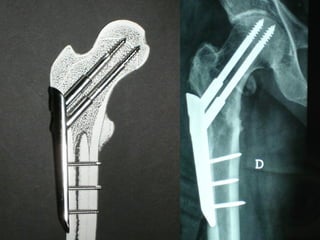
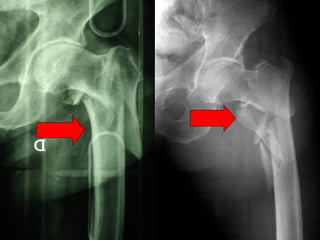
- 6. Tradizionalmente si ritiene importante per la stabilità delle fratture pertrocanteriche lâintegrità della parte mediale della metafisi prossimale del femore
- 7. Ėý
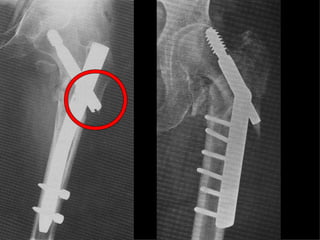
- 8. In realtà la zona piÃđ importante per la ricostruzione di questo tipo di fratture ÃĻ il muro laterale contro il quale si impatta il frammento metaepifisario mediale
- 9. Ėý
- 10. Ėý
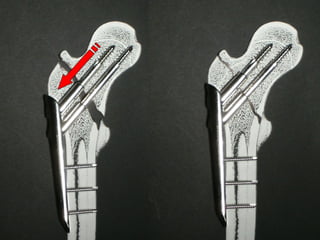
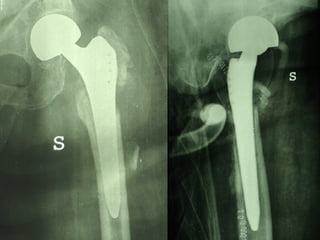
- 11. Se il muro laterale ÃĻ rotto o viene lesionato durante la sintesi , come spesso accade in fase di applicazione della vite cefalica dei chiodi endomidollari o della vite-placca, andremo incontro al collasso della frattura e ad un conseguente lungo periodo di impotenza funzionale
- 12. Ėý
- 13. Ėý
- 14. Con la placca di Gotfried non si ÃĻ mai riscontrato un danno iatrogeno del muro laterale e nessun collasso della frattura.CiÃē ÃĻ dovuto al fatto che i fori per lâapplicazione delle due viti prossimali sono di piccolo diametro (9 mm) rispetto ai 16-32 mm necessari per introdurre la vite cefalica di un chiodo endomidollare o di una vite-placca a compressione.
- 15. Ėý
- 16. La placca PC.C.P. viene inoltre applicata per via percutanea attraverso due piccole incisioni ottenendo in tal modo un minimo trauma chirurgico ed una perdita di sangue estremamente ridotta in pazienti che per lâetà sono già in condizioni critiche
- 17. Ėý
- 18. Ėý
- 19. Ėý
- 20. Ėý
- 21. Ėý
- 22. Ėý
- 23. Ėý
- 24. Ėý
- 25. Ėý
- 26. Ėý
- 27. Ėý
- 28. Ėý
- 29. Ėý
- 30. Ėý
- 31. Dal Gennaio 2005 ad Agosto 2006 110 placche di Gotfried Età media : 78 anni (range 29-94) Tempo chirurgico: 30 minuti (range 12-45) IMMEDIATA CONCESSIONE DEL CARICO
- 32. F. 76a
- 33. Ėý
- 34. M. 73a
- 35. Ėý
- 36. F. 86a
- 37. Ėý
- 38. F. 91a
- 39. Ėý
- 40. M. 87a
- 41. Ėý
- 42. F. 75a
- 43. Ėý
- 44. F. 68a
- 45. Ėý
- 46. M. 29a
- 47. Ėý
- 48. M. 34a
- 49. Ėý
- 50. Ėý
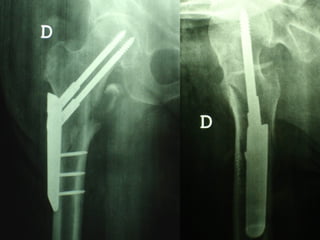
- 51. 3 INSUCCESSI
- 52. F. 72a
- 53. Ėý
- 54. Ėý
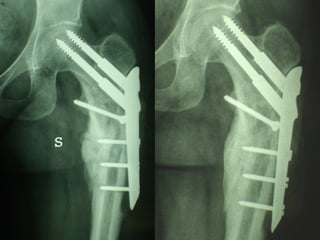
- 55. F. 77a
- 56. Ėý
- 57. Ėý
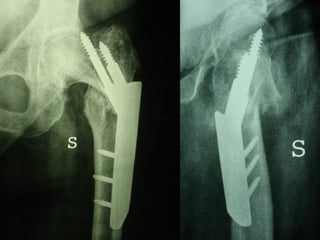
- 58. F. 84a
- 59. Ėý
- 60. Ėý
- 61. Ėý
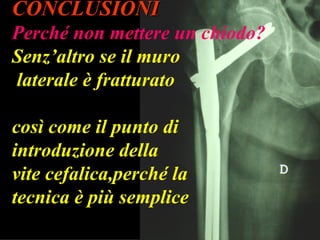
- 62. CONCLUSIONI PerchÃĐ non mettere un chiodo? Senzâaltro se il muro laterale ÃĻ fratturato cosÃŽ come il punto di introduzione della vite cefalica,perchÃĐ la tecnica ÃĻ piÃđ semplice
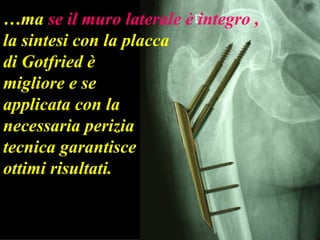
- 63. âĶ ma se il muro laterale ÃĻ integro , la sintesi con la placca di Gotfried ÃĻ migliore e se applicata con la necessaria perizia tecnica garantisce ottimi risultati.
- 64. Ėý
- 65. Ėý
- 66. Trauma center
- 67. Ėý
- 68. Ėý
- 69. Ėý
- 70. Ėý
- 71. POLITRAUMA â Sindrome che si instaura a seguito di lesioni multiple e si manifesta nella forma di massicce reazioni sistemiche , che possono portare al mal funzionamento e perfino alla compromissione totale di altri organi e sistemi vitali non direttamente coinvolti nel trauma.â
- 72. Le fratture , da intendersi come lesioni sia dellâosso che delle parti molli in grado di provocare dolore ed emorragia, sono una componente molto frequente nel politrauma , soggette a loro volta a diverse complicanze .
- 73. Ėý
- 74. Ėý
- 75. Ėý
- 76. Ėý
- 77. First priority : Sopravvivenza del paziente insieme al mantenimento di normali funzioni cognitive RIANIMAZIONE per assicurare una adeguata perfusione ed ossigenazione degli organi vitali
- 78. Rianimazione
- 79. Trattamento rianimatorio RISPOSTA NEGATIVA INTERVENTO CHIRURGICO SALVAVITA
- 80. 1- DECOMPRESSIONE delle cavitÃ
- 82. Pneumotorace
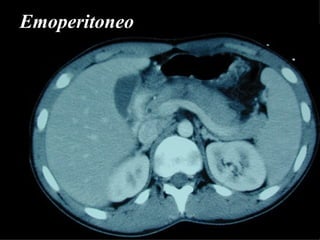
- 84. 2- CONTROLLO della EMORRAGIA
- 85. Emoperitoneo
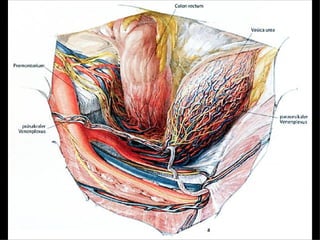
- 86. Gravi traumi della pelvi
- 88. DAMAGE CONTROL Controllo dellâemorragia e delle lesioni contaminate mediante abbondanti lavaggi, packing pelvici , suture provvisorie delle ferite e delle cavità addominali e successivo intervento chirurgico dopo 6 â 12 ore.
- 89. Ėý
- 90. Ėý
- 91. Ėý
- 92. Ėý
- 93. Ėý
- 94. Ėý
- 95. Ėý
- 96. Trattamento rianimatorio RISPOSTA POSITIVA Trattamento chirurgico primario differito
- 97. APPARATO LOCOMOTORE Hanno priorità assoluta : Fratture esposte Fratture con lesioni vascolari e nervose Fasciotomie Fratture multiple delle ossa lunghe Fratture della colonna vertebrale
- 98. Ėý
- 99. Ėý
- 100. Ėý
- 101. Ėý
- 102. Fratture multiple delle ossa lunghe
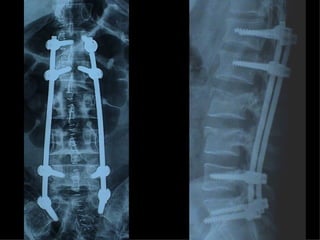
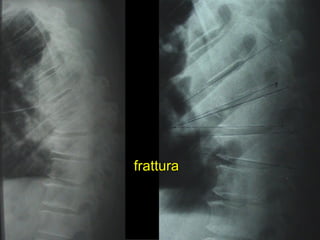
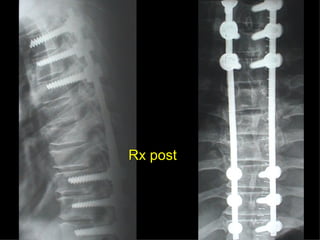
- 103. Fratture della colonna vetebrale
- 104. Ėý
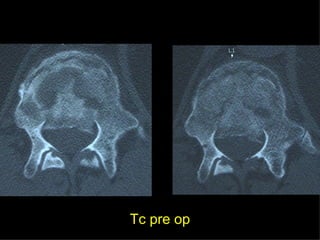
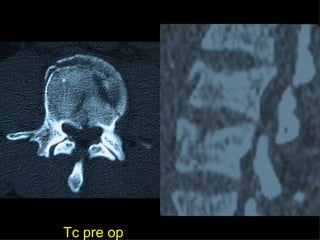
- 105. Tc pre op
- 106. Tc pre op
- 107. Ėý
- 108. Ėý
- 109. Ėý
- 110. Ėý
- 111. Ėý
- 112. Ėý
- 113. Ėý
- 114. Ėý
- 115. Ėý
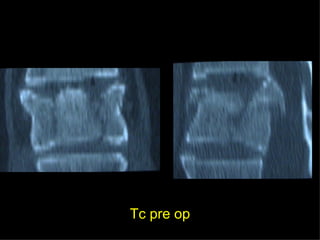
- 116. Tc pre op
- 117. Ėý
- 118. frattura
- 119. TC RMN
- 120. Rx post
- 121. Ėý
- 122. Ėý
- 123. Timing chirurgico 1° GIORNO :- intervento salvavita - âDamage controlâ - trattamento chirurgico primario differito 2°-3° GIORNO : soltanto un âsecond lookâ
- 124. 5°-10° GIORNO : âwindow of opportunityâ per un intervento definitivo 10°- 20° GIORNO : NESSUN TRATTAMENTO CHIRURGICO Dal 21° GIORNO : intervento chirurgico secondario - ricostruttivo
- 125. Precoce stabilizzazione delle fratture DRASTICO CALO DEL TASSO DI MORTALITAâ
- 126. Le fratture hanno un impatto fondamentale sulla severità delle reazioni sistemiche post traumatiche
- 127. Emorragia
- 128. Contaminazione della frattura esposta
- 129. Stress e dolore
- 130. Interferenza con le cure intensive
- 131. STABILIZZAZIONE DELLE FRATTURE
- 132. Ėý
- 135. Ėý
- 136. Ėý
- 137. Ėý
- 138. Ėý
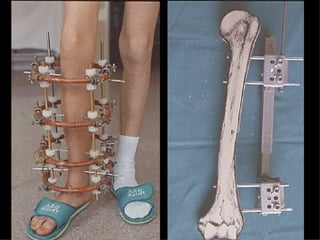
- 139. Fissazione esterna
- 140. Ėý
- 141. Ėý
- 142. Evitare rigidi protocolli relativi al timing ed alle scelte del mezzo di sintesi, accordando la preferenza alla personalizzazione del trattamento in base al tipo di trauma , alle condizioni del paziente ed allâ esperienza del chirurgo.
- 143. Ėý
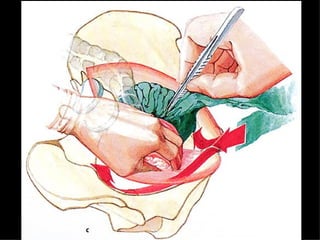
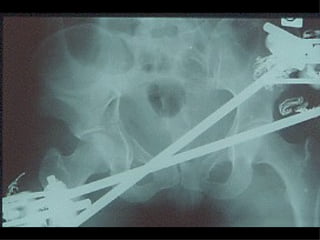
- 144. La lesione dellâapparato muscolo scheletrico che richiede in ogni caso un trattamento chirurgico con priorità assoluta ÃĻ la rottura dellâanello pelvico , che comporta una emorragia severa nel retro peritoneo e nella cavità peritoneale.
- 145. Immediata riduzione e fissazione del bacino
- 146. Se la risposta emodinamica a questo trattamento ÃĻ buona il paziente verrà monitorato e potrà essere programmato un successivo intervento di osteosintesi definitiva
- 147. Ėý
- 148. Ėý
- 149. Ėý
- 150. Ėý
- 151. Ėý
- 152. Ėý
- 153. Ėý
- 154. Ėý
- 155. Ėý
- 156. Angiografia e/o packing pelvico Se il paziente rimane instabile
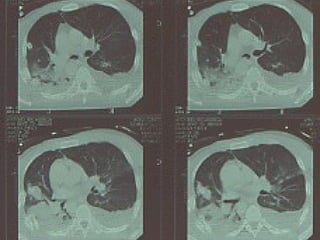
- 157. Unâaltra situazione di emergenza ortopedica ÃĻ rappresentata dalle fratture delle ossa lunghe in pazienti con gravi traumi cranici e toracici
- 158. Ėý
- 159. A.Luzzati Reward:up to $ 50 million
- 160. Ėý
- 161. Il trattamento delle fratture distali di femore con la placca NCB a stabilità angolare poliassiale A.Luzzati , F.Feraboli ( Divisione di Ortopedia â Azienda Ospitaliera di Cremona Responsabile : Dott. Alessandro Luzzati )
- 162. Ėý
- 163. Ėý
- 164. Ėý
- 165. Ėý
- 166. Ėý
- 167. MIPPO
- 168. Ėý
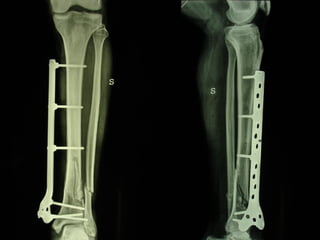
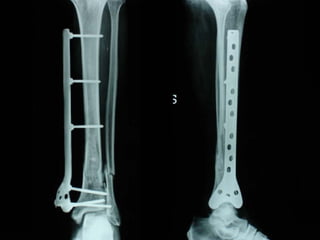
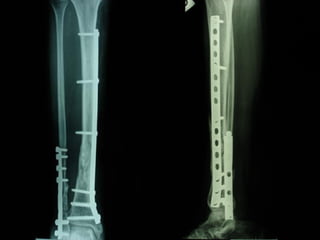
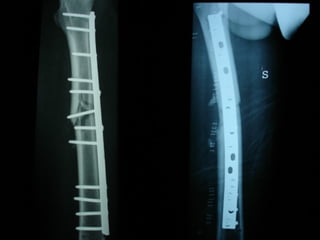
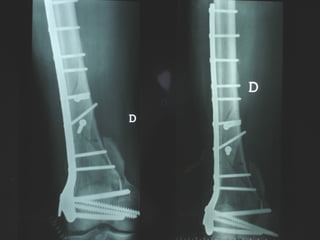
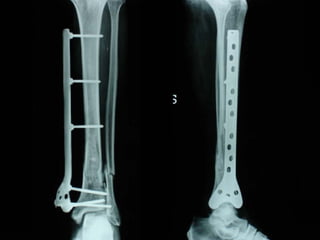
- 169. Dal Gennaio 2000 al Febbraio 2006 abbiamo trattato 167 fratture chiuse con placca percutanea in 164 pazienti : 27 lesioni diafisarie di gamba, 12 piloni tibiali , 11 fratture prossimali di tibia, 36 fratture sovracondiloidee di femore, 17 fratture diafisarie di femore, 43 fratture metaepifisarie prossimali di omero, 21 diafisarie dâomero. 156 guarigioni 8 fallimenti
- 170. Dal Giugno 2002 al Dicembre 2004 abbiamo trattato 5 fratture esposte: 3 di tibia e 2 di ulna 5 guarigioni
- 171. Ėý
- 172. Ėý
- 173. Ėý
- 174. Ėý
- 175. Ėý
- 176. Ėý
- 177. Ėý
- 178. Ėý
- 179. Ėý
- 180. Ėý
- 181. Ėý
- 182. Ėý
- 183. Ėý
- 184. Ėý
- 185. Ėý
- 186. Ėý
- 187. Ėý
- 188. Ėý
- 189. Ėý
- 190. Ėý
- 191. Ėý
- 192. Ėý
- 193. Ėý
- 194. Ėý
- 195. Ėý
- 196. Ėý
- 197. Ėý
- 198. Ėý
- 199. Ėý
- 200. Ėý
- 201. Ėý
- 202. Ėý
- 203. Ėý
- 204. Ėý
- 205. Ėý
- 206. Ėý
- 207. Ėý
- 208. Ėý
- 209. Ėý
- 210. Ėý
- 211. Ėý
- 212. Ėý
- 213. Ėý
- 214. Ėý
- 215. Ėý
- 216. Ėý
- 217. Ėý
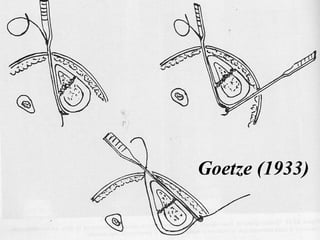
- 218. I buoni risultati ottenuti dipendono da 5 punti fondamentali: una accurata riduzione percutanea della frattura precise vie di accesso lâutilizzo della placca che consenta il piÃđ lungo braccio di leva possibile il pretensionamento della placca una sintesi con un ridotto numero di viti
- 219. Accurata riduzione percutanea della frattura
- 220. Ėý
- 221. Goetze (1933)
- 222. Ėý
- 223. Ėý
- 224. Ėý
- 225. Ėý
- 226. Ėý
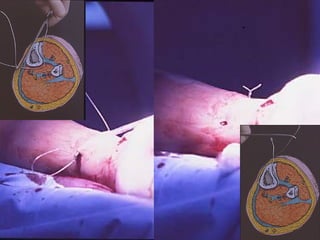
- 227. Precise vie di accesso
- 228. Ėý
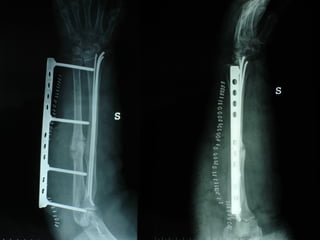
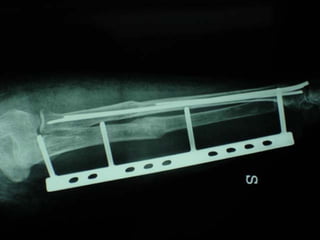
- 229. Placche lunghe e pretensionate
- 230. Placche lunghe e pretensionate Sintesi con un ridotto numero di viti
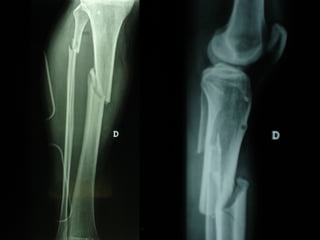
- 231. 2 Insuccessi
- 232. Ėý
- 233. Ėý
- 234. Ėý
- 235. Ėý
- 236. Ėý
- 237. Ėý
- 238. Ėý
- 239. Ėý
- 240. Ėý
- 241. Fratture esposte
- 242. Ėý
- 243. Ėý
- 244. Ėý
- 245. Ėý
- 246. Ėý
- 247. Ėý
- 248. Ėý
- 249. Ėý
- 250. Ėý
- 251. Ėý
- 252. Ėý
- 253. Ėý
- 254. Ėý
- 255. Ėý
- 256. Ėý
- 257. Ėý
- 258. Ėý
- 259. Ėý
- 260. Ėý
- 261. Ėý
- 262. Ėý
- 263. Ėý
- 264. Ėý
- 265. Ėý
- 266. Ėý
- 267. Ėý
- 268. Ėý
- 269. Ėý
- 270. Ėý
- 271. Ėý
- 272. Ėý
- 273. Dal Gennaio 2000 al Dicembre 2005 27 placche LISS di femore
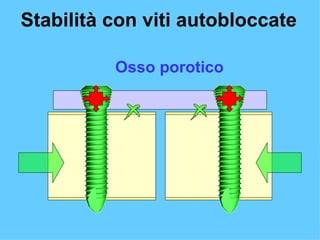
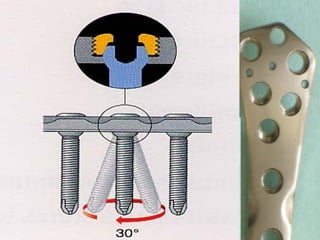
- 274. Stabilità tramite attrito placca ïģ osso
- 275. Osso porotico Stabilità con viti autobloccate
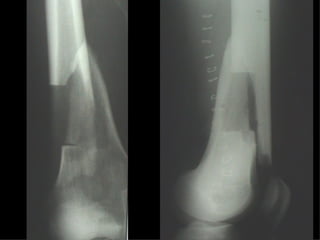
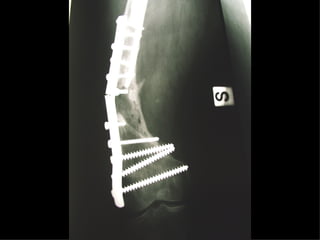
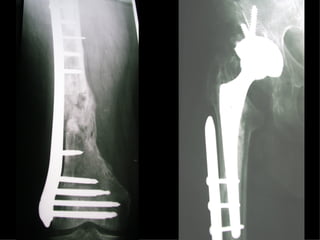
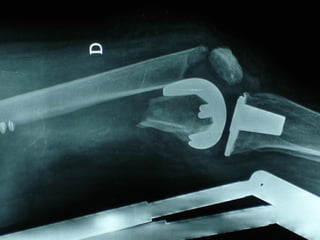
- 276. INDICAZIONI COMUNI Fratture sovracondiloidee Fratture intercondiliodee Fratture diafisarie distali PARTICOLARI Fratture con grave osteoporosi Fratture periprotesiche
- 277. VANTAGGI CHIRURGIA MININVASIVA Mini Open Inserimento della placca sottocutaneo per scivolamento Viti percutanee Preservazione dei tessuti molli Ridotto danno vascolare Rapida ripresa funzionale
- 278. Ėý
- 279. Ėý
- 280. Ėý
- 281. Ėý
- 282. Ėý
- 283. Ėý
- 284. Ėý
- 285. Ėý
- 286. Ėý
- 287. Ėý
- 288. Ėý
- 289. Ėý
- 290. Ėý
- 291. Ėý
- 292. Ėý
- 293. Ėý
- 294. F, 68 y
- 295. Ėý
- 296. Ėý
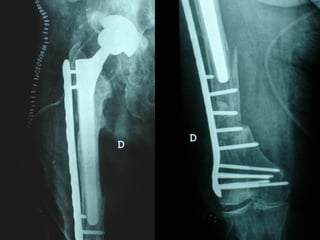
- 297. LISS NCB
- 298. Ėý
- 299. Ėý
- 300. Ėý
- 301. Ėý
- 302. NCB
- 303. Ėý
- 304. Ėý
- 305. Ėý
- 306. Ėý
- 307. Ėý
- 308. Ėý
- 309. Ėý
- 310. Ėý
- 311. Ėý
- 312. Ėý
- 313. Ėý
- 314. Ėý
- 315. Ėý
- 316. Ėý
- 317. Ėý
- 318. Ėý
- 319. Ėý
- 320. Ėý
- 321. Ėý
- 322. Ėý
- 323. Ėý
- 324. Ėý
- 325. Ėý
- 326. Ėý
- 327. Ėý
- 328. Ėý
- 329. Ėý
- 330. Ėý
- 331. Ėý
- 332. Ėý
- 333. Ėý
- 334. Ėý
- 335. Conclusioni Riduzione anatomica Minimo trauma chirurgico Corretto equilibrio fra elasticità e stabilità Precoce mobilizzazione