










![±R╬▓ųó║“╚║
1. Ž┬ų½ż╬═┤ż▀ż“░ķż”č³═┤
2. Ž┬ų½ż╬▀\äė┬ķ»w
3. ┼┼─“šŽ║”Īó▒Ń╩¦Į¹Īóų▒─cšŽ║”
Ż©S3-S5Ż®
4. ĖąęÖšŽ║”
±R╬▓ųó║“╚║ż╬į\ČŽżŪ─“ķ]żŽ
ĖąČ╚90%
? 2021 M.Okuyama Akita University Graduate School of Medicine](https://image.slidesharecdn.com/erresidencytraining2020-26-210206065427/85/ER-residency-training-2020-26-11-320.jpg)

































More Related Content
What's hot (20)
Similar to ER residency training 2020 26 (8)






More from Manabu Okuyama (17)

















ER residency training 2020 26
- 1. Š╚╝▒īØÅĻ 2020-26 ĪĖč³═┤Ī╣ Ū’╠’┤¾č¦┤¾č¦į║ęĮ覎ĄčąŠ┐┐ŲŠ╚╝▒╝»ųąų╬»¤ęĮč¦ųvū∙ ░┬╔Į č¦ ? 2021 M.Okuyama Akita University Graduate School of Medicine
- 2. Red flags sign ? 2021 M.Okuyama Akita University Graduate School of Medicine JAMA. 1992;268(6):760-765. doi:10.1001/jama.1992.03490060092030 Pseudoclaudication é╬ķgŪĘąį§╦ąą Sciatica ū°╣Ū╔±ĮU═┤ What can the history and physical examination tell us about low back pain?
- 3. ? 2021 M.Okuyama Akita University Graduate School of Medicine Most clinical practice guidelines for back pain recommend the use of red flags to help identify those patients with a higher likelihood of spinal fracture or malignancy who then become candidates for more extensive diagnostic investigations. ČÓż»ż╬č³═┤ż╬┼R┤▓į\»¤ź¼źżź╔źķźżź¾żŪżŽĪó╝╣ūĄ╣Ūš█żõÉÖąį─[»āż╬┐╔─▄ąįż¼Ė▀żż╗╝š▀ż“╠žČ©ż╣żļż┐żß ż╦źņź├ź╔źšźķź├ź░ż“╩╣ė├ż╣żļż│ż╚ż“═ŲŖXżĘżŲż¬żĻĪóż│żņżķż╬╗╝š▀żŽżĶżĻÄ┌╣Āż╩į\ČŽŚ╩¢╦ż╬║“čaż╚ż╩żļĪŻ ┤_┬╩ż╬Ė▀żżRed flags (post-test probability, 95% confidence interval) ╣Ūš█ 1. Ė▀²h Ż©─ąąį©R65ÜrĪó┼«ąį©R75ÜrŻ® (9%, 3% to 25%) 2. ķLŲ┌ż╬ź╣źŲźĒźżź╔╩╣ė├ (33%, 10% to 67%) 3. ųžųó═Ōé¹ (11%, 8% to 16%) 4. ┤“ōõżõ┤ņäōż╬┤µį┌ (62%, 49% to 74%) 5. č}╩²ż╬╬ŻĻōę“ūė (90%, 34% to 99%) ÉÖąį╝▓╗╝ 1. ░®ż╬╝╚═∙ (33%, 22% to 46%).
- 4. ? 2021 M.Okuyama Akita University Graduate School of Medicine č³═┤į\»¤ź¼źżź╔źķźżź¾2019 Ė─ėåĄ┌2░µ ęįŽ┬ż╬3ż─ż╦ź╚źĻźó®`źĖż╣żļż│ż╚ż¼äßżßżķżņżļ 1. Red flagsż“ėążĘųž║Vż╩╝╣ūĄ╝▓╗╝ż╬┐╔─▄ąįż╬żóżļč³═┤ 2. ╔±ĮUųóū┤ż╬ż╩żżč³═┤ 3. ╔±ĮUųóū┤ż“░ķż”č³═┤
- 5. ? 2021 M.Okuyama Akita University Graduate School of Medicine Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Recommendation 1 3ż─ż╬Ä┌żżź½źŲź┤źĻ®`ż╬1ż─ż╦ĘųŅÉż╣żļż┐żßż╦ĪóĮ╣ĄŃż“Įgż├ż┐▓ĪÜsż╚╔Ē╠ÕŚ╩ ¢╦ż“īg╩®ż╣żļ▒žę¬ż¼żóżĻż▐ż╣ 1. ĘŪ╠ž«ÉĄ─č³═┤ 2. ╔±ĮUĖ∙ųóųóū┤żõ╝╣ų∙╣▄Ž┴šŁųóū┤ż╬┐╔─▄ąįż╬żóżļč³═┤ 3. żĮż╬╦¹ż╬╠ž«ÉĄ─įŁę“ż╦ķv▀Bż╣żļč³═┤ └² ó┘ ─[»ā ó┌ Ėą╚Š ó█ łRŲ╚╣Ūš█ ó▄ ÅŖų▒ąį╝╣ūĄčū Ann Intern Med. 2007; 147(7):478-491. doi:10.7326/0003-4819-147-7-200710020-00006
- 6. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society ż“Ė─ēõ Ann Intern Med. 2007; 147(7):478-491. doi:10.7326/0003-4819-147-7-200710020-00006 įŁę“ ųóū┤?╔Ē╠Õ╦∙ęŖ ╗ŁŽ±Ś╩¢╦ ░® ą┬żĘżżč³═┤ż╬░kųóż╚░®ż╬┤µį┌ MRI įŁę“▓╗├„ż╬╠Õųž£p╔┘ XŠĆą┤šµ 1ż½į┬ęį╔Žųóū┤ż¼Ė─╔ŲżĘż╩żż 50Üręį╔Ž č}╩²ż╬╬ŻĻōę“ūėż╬┤µį┌ XŠĆ/MRI ╝╣ūĄĖą╚Šųó ░k¤ß MRI ╦aż╬Š▓├}═Čėļ ūŅĮ³ż╬Ėą╚Šųó ±R╬▓ųó║“╚║ ┼┼─“šŽ║” MRI č}╩²ż╬źņź┘źļż╦ż’ż┐żļĮŅ┴”Ą═Ž┬ ų▒─cšŽ║” ═╬▓┐Ī½╗ßĻÄ▓┐ż╬ĖąęÖšŽ║” ūĄ╠ÕłRŲ╚╣Ūš█ ╣Ū┤ų¾Āųóż╬┤µį┌ XŠĆą┤šµ ź╣źŲźĒźżź╔ż╬╩╣ė├ Ė▀²h ÅŖų▒ąį╝╣ūĄčū │»ż╬ż│ż’żążĻ XŠĆą┤šµ ▀\äėż╦żĶżļĖ─╔Ų ═╬▓┐═┤ ├„ż▒ĘĮż╦▒│▓┐═┤żŪ─┐ż¼ęÖżßżļ ╚¶─Ļš▀ ųžųó?▀Mąąąį╔±ĮUšŽ║” ▀Mąąż╣żļ▀\äėšŽ║” MRI č³═┤ż╬Ķaäeį\ČŽ įŁę“ ųóū┤?╔Ē╠Õ╦∙ęŖ ╗ŁŽ±Ś╩¢╦ ūĄķg░Õźžźļź╦źó L4, L5, S1ż╬╔±ĮUĖ∙ųóū┤ż“░ķż”č³═┤ None SLRĻ¢ąį 1ż½į┬ęį╔ŽŠAż»ųóū┤ MRI ╝╣ų∙╣▄Ž┴šŁųó Ž┬ų½żžż╬Ę┼╔ó═┤ None Ė▀²h ķgą¬ąį§╦ąą 1ż½į┬ęį╔ŽŠAż»ųóū┤ MRI ? 2021 M.Okuyama Akita University Graduate School of Medicine
- 7. ? 2021 M.Okuyama Akita University Graduate School of Medicine źūźķźżź▐źĻź▒źóŅIė“żŪż╬č³═┤ųó ÖCąĄĄ─╝╣ūĄ╝▓╗╝Ż©97%Ż® ĘŪÖCąĄĄ─╝╣ūĄ╝▓╗╝Ż©1ŻźŻ® ─┌─Ā╝▓╗╝Ż©2ŻźŻ® č³ż╬ŠoÅł 70% ą┬╔·╬’ 0.7% ╣Ū▒P─┌─ĀŲ„ ēõąį╝▓╗╝ 10% ČÓ░kąį╣Ū¾l─[ Ū░┴óŽ┘čū źŪźŻź╣ź»Ż©╝╣ūĄųóŻ® ▄×ęŲąį░® ūėīm─┌─żųó ūĄķgķv╣ØŻ©ēõą╬ąįķv╣ØųóŻ® źĻź¾źč─[ż╚░ūč¬▓Ī ┬²ąį╣Ū▒P─┌čūųóąį╝▓╗╝ ūĄķg░Õźžźļź╦źó 4% ╝╣¾l─[»ā ─I╝▓╗╝ ╝╣ų∙╣▄Ž┴šŁųó 3% ßßĖ╣─ż─[»ā ─IĮY╩»ųó ╝╣ūĄż╣ż┘żĻųó 2% Ėą╚Š 0.1% ─Iė█─Ičū ╣Ū┤ųżĘżńż”ųó ╣Ūš█ 4% ╣Ū¾lčū ─Ių▄ćņ─ō»ā ═Ōé¹ąį╣Ūš█ <1% öĪč¬ųóąįūĄķg░Õčū ┤¾äė├}┴÷ Ž╚╠ņąį╝▓╗╝ <1% ░°╝¼ąį─ō»ā ╬Ė─c╝▓╗╝ ųžČ╚ż╬ßß═õ ė▓─ż═Ō─ō»ā ─ŗčū ųžČ╚ż╬╝╣ų∙é╚═õųó čūųóąįķv╣Øčū 0.3% Ą©ć░čū ÅŖų▒ąį╝╣ūĄčū Ž¹╗»╣▄┤®┐ū Ū¼░_ąį╝╣ūĄčū źžźļź╦źó Ę┤ÅĻąįķv╣Øčū čūųóąį─c╝▓╗╝ źĘźńźżź©źļź▐ź¾▓ĪŻ©╣Ū▄ø╣ŪųóŻ® ╣Ūź┌®`źĖź¦ź├ź╚▓Ī N Engl J Med. 2001 Feb 1;344(5):363-70. doi: 10.1056/NEJM200102013440508.
- 8. č³═┤ż╬ĘųŅÉ 1. ╔±ĮUųóū┤ż╬ż╩żżč³═┤ 2. ╔±ĮUųóū┤ż“░ķż”č³═┤ 3. ųž║Vż╩╝╣ūĄ╝▓╗╝ż╬┐╔─▄ąįż╬żóżļč³═┤ ó┘ ░® ó┌ Ėą╚Š ó█ ╣Ūš█ 4. ─┌─Ā╝▓╗╝?╚½╔Ē╝▓╗╝ż╦░ķż”č³═┤ ? 2021 M.Okuyama Akita University Graduate School of Medicine Red Flags sign
- 9. ▓ĪÜs┬Ś╚Ī 1. ─Ļ²hĪó░®ż╬╝╚═∙ÜsĪóįŁę“▓╗├„ż╬╠Õųž£p╔┘Īó╠█═┤ż╬│ųŠAĢrķgĪóęįŪ░ż╬ų╬»¤ż╦īØż╣żļĘ┤ÅĻąį 2. Š▓├}─┌╦a╬’ż╬╩╣ė├żõ─“┬ĘĖą╚Šż¼żóżļż╚╝╣ūĄĖą╚Šųóż╬ę╔żżż¼Ė▀ż▐żļ 3. ÅŖų▒ąį╝╣ūĄčūżŽ╚¶żż─ąąįż╦ČÓżż 4. ą▌ŽóżĘżŲżŌĖ─╔ŲżĘż╩żż═┤ż▀żŽ╠ž«ÉĄ─żŪżŽż╩żżż¼Īó╚½╔Ēąį╝▓╗╝ż╦īØżĘżŲ├¶Ėąż╩╦∙ęŖ 5. ū°╣Ū╔±ĮU═┤ż╬ųóū┤ ķgą¬ąį§╦ąąż╬ėą¤oŻ¬ 6. ±R╬▓ųó║“╚║ż╬ųóū┤ 7. ą─└Ē╔ń╗ߥ─å¢Ņ}ż╬įuü² ż”ż─▓Īź╣ź»źĻ®`ź╦ź¾ź░ ? 2021 M.Okuyama Akita University Graduate School of Medicine JAMA. 1992;268(6):760-765. doi:10.1001/jama.1992.03490060092030 Ż¬╝╣ų∙╣▄Ž┴šŁųóż╬ųóū┤Ż║═┤ż▀ż¼ĪóÜiż»Īó┴óż─Īóż▐ż┐żŽ╠žČ©ż╬ū╦ä▌ż“ŠS│ųż╣żļż│ż╚żŪÉÖ╗»żĘĪóū∙ż├ż┐żĻ║ß ż╦ż╩ż├ż┐żĻż╣żļż│ż╚żŪ▌X£pż╣żļĪŻą▌Žóż¼ż╩ż»żŲżŌĪóż½ż¼ż¾ż└ĪóŪ·ż¼ż├ż┐ū╦ä▌ż“ż╚żļż│ż╚ż╦żĶż├żŲżżż»żķ ż½Ė─╔Ųż╣żļŻ©Up to dateŻ®
- 10. ? 2021 M.Okuyama Akita University Graduate School of Medicine ±R╬▓ųó║“╚║ ģgę╗ż╬╔±ĮUĖ∙ż╦ė╔└┤żĘż╩żż╔±ĮUųóū┤ ūŅĮ³ż╬░®ż╬╝╚═∙żõį┘░k ╠žż╦╚ķ░®ĪóŪ░┴óŽ┘░®ĪóĘ╬░®Īó─I░®ĪóČÓ░kąį╣Ū ¾l─[Īó╝ūū┤Ž┘ż¼ż¾ ░®ż╬┐╔─▄ąį ? ČÓ╩²ż╬źĻź╣ź»źšźĪź»ź┐®` ? ░®ż╬╝╚═∙ ? ┼R┤▓Ą─ż╦ÅŖż»ę╔ż” ╝╣ūĄĖą╚Šųóż╬ųóū┤Ī󟥟żź¾ ? ░k¤ß ? ├Ōę▀ęųųŲĪó═Ė╬÷ ? ūŅĮ³ż╬Ėą╚ŠųóĪó╝╣ūĄż╬äIų├Īó╩ųąg łRŲ╚╣Ūš█ż╬źĻź╣ź» ? Ė▀²h ? ź╣źŲźĒźżź╔ķLŲ┌╩╣ė├ ? ═Ōé¹ ? ╣Ū┤ų¾Āųóż╬źĻź╣ź»ż“│ųż─╚╦ż╬▌XČ╚ż╬═Ōé¹ ░®ż╬źĻź╣ź»ż¼ż╩żż ╝╣ūĄż╬Ėą╚Šż╬źĻź╣ź»ż¼ż╩żż ▀Mąąż╣żļ╔±ĮUųóū┤ż¼ż╩ MRI ╗╝š▀ż╦║Žż’ż╗ż┐╗ŁŽ±Ś╩¢╦ MRI XŠĆą┤šµ XŠĆą┤šµŻ½Æ±č¬ ŻžŠĆ╦∙ęŖżŪÉÖąįż╬┐╔─▄ąįżóżĻ ŻžŠĆ«É│Żż╩żĘ Æ±č¬żŪčūųóĘ┤ÅĻżóżĻ ░®ż╬įuü² ę╔żżż╬źņź┘źļ ųąĪ½Ė▀ ę╔żżż╬źņź┘źļ Ą═ MRI Æ±č¬ Æ±č¬żŪčūųóĘ┤ÅĻżóżĻ Æ±č¬żŪčūųóĘ┤ÅĻż╩żĘ MRI ╗ŁŽ±Ś╩¢╦▓╗ę¬ ▒Ż┤µĄ─ų╬»¤ ī¤ķTęĮź│ź¾źĄźļźŲ®`źĘźńź¾ No No No No No Yes Yes Yes Yes Yes N Engl J Med. 2001 Feb 1;344(5):363-70. doi: 10.1056/NEJM200102013440508. Ė─ēõ
- 11. ±R╬▓ųó║“╚║ 1. Ž┬ų½ż╬═┤ż▀ż“░ķż”č³═┤ 2. Ž┬ų½ż╬▀\äė┬ķ»w 3. ┼┼─“šŽ║”Īó▒Ń╩¦Į¹Īóų▒─cšŽ║” Ż©S3-S5Ż® 4. ĖąęÖšŽ║” ±R╬▓ųó║“╚║ż╬į\ČŽżŪ─“ķ]żŽ ĖąČ╚90% ? 2021 M.Okuyama Akita University Graduate School of Medicine
- 12. ╔Ē╠Õ╦∙ęŖ MMT ųó║“ąįč³ūĄūĄķg░Õźžźļź╦źó90Żźęį╔ŽżŽĪóL4/L5ż¬żĶżėL5/S1 ? SLR ? Žźż╬Ū³Ū·▀Mš╣Ż©┤¾═╚Č■Ņ^ĮŅĪó┤¾═╚╦─Ņ^ĮŅ L4╔±ĮUĖ∙Ż® ? ūŃż╬▒│Ū³Ż©Ū░├ä╣ŪĮŅ L5╔±ĮUĖ∙Ż® ? ūŃż╬ĄūŪ³Ż©Ž┬═╚╚²Ņ^ĮŅ S1╔±ĮUĖ∙Ż® ? 2021 M.Okuyama Akita University Graduate School of Medicine
- 13. Manual Muscle TestingŻ©MMTŻ® 5 Normal ▀\äė╣Āćņ╚½╠Õż╦Č╔ż├żŲäėż½ż╣ż│ż╚ż¼żŪżŁĪóūŅ┤¾ż╬═Į╩ųĄų┐╣ż╦┐╣żĘżŲūŅĮK▀\äėė“ ż“▒Ż│ųżŪżŁżļ 4 Good ▀\äė╣Āćņ╚½╠Õż╦Č╔ż├żŲäėż½ż╣ż│ż╚ż¼żŪżŁĪóųąĄ╚Č╚?ÅŖČ╚ż╬═Į╩ųĄų┐╣ż╦┐╣żĘżŲūŅ ĮK▀\äėė“ż“▒Ż│ųżŪżŁżļ Ż│ Fair ▀\äė╣Āćņ╚½╠Õż╦Č╔ż├żŲäėż½ż╣ż│ż╚ż¼żŪżŁżļż¼Īó═Į╩ųĄų┐╣ż╦żŽ┐╣ż╣żļż│ż╚ż¼żŪżŁ ż╩żż 2 Poor ųž┴”ż╬ė░Ēæż“│²żżż┐ų½╬╗żŪż╩żķĪó▀\äė╣Āćņ╚½╠ÕĪóż▐ż┐żŽę╗▓┐ż╦Č╔ż├żŲäėż½ż╣ż│ ż╚ż¼żŪżŁżļ 1 Trace ĮŅģ¦┐sż¼─┐ż╦ęŖż©żļĪóż▐ż┐żŽ┤źų¬żŪżŁżļż¼Īóķv╣Ø▀\äėżŽż¬ż│żķż╩żż 0 Zero ĮŅģ¦┐s?ķv╣Ø▀\äėżŽ╚½ż»ż¬ż│żķż╩żż ? 2021 M.Okuyama Akita University Graduate School of Medicine
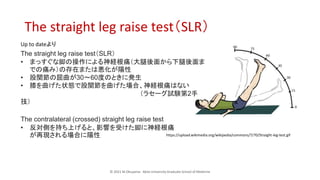
- 14. ? 2021 M.Okuyama Akita University Graduate School of Medicine The straight leg raise testŻ©SLRŻ® https://upload.wikimedia.org/wikipedia/commons/7/70/Straight-leg-test.gif The straight leg raise testŻ©SLRŻ® ? ż▐ż├ż╣ż░ż╩Į┼ż╬▓┘ū„ż╦żĶżļ╔±ĮUĖ∙═┤Ż©┤¾═╚ßß├µż½żķŽ┬═╚ßß├µż▐ żŪż╬═┤ż▀Ż®ż╬┤µį┌ż▐ż┐żŽÉÖ╗»ż¼Ļ¢ąį ? ╣╔ķv╣Øż╬Ū³Ū·ż¼30?60Č╚ż╬ż╚żŁż╦░k╔· ? Žźż“Ū·ż▓ż┐ū┤æBżŪ╣╔ķv╣Øż“Ū·ż▓ż┐ł÷║ŽĪó╔±ĮUĖ∙═┤żŽż╩żż Ż©źķź╗®`ź░įć“YĄ┌2╩ų ╝╝Ż® The contralateral (crossed) straight leg raise test ? Ę┤īØé╚ż“│ųż┴╔Žż▓żļż╚Īóė░Ēæż“╩▄ż▒ż┐Į┼ż╦╔±ĮUĖ∙═┤ ż¼į┘¼FżĄżņżļł÷║Žż╦Ļ¢ąį Up to dateżĶżĻ
- 15. č³═┤į\»¤ ī¤ķTęĮź│ź¾źĄźļź╚ż╬╗∙£╩ 1. ▓ĪÜs┬Ś╚Ī ó┘ OPQRST ó┌ źņź├ź╔źšźķź░źĄźżź¾ ó█ ±R╬▓ųó║“╚║ 2. ╔Ē╠Õ╦∙ęŖ ó┘ SLR ó┌ Žźż╬Ū³Ū·Īó╔ņš╣?ūŃż╬▒│Ū³ĪóŪ³Ū· ó█ ĖąęÖšŽ║”ż╬ėą¤o 3. Ś╩¢╦ ó┘ Æ±č¬ CRPż╩ż╔Ėą╚Šż╬įuü²Īó╚½╔Ēąį╝▓╗╝ż╬įuü² ó┌ ŻžŠĆą┤šµ ó█ ╔±ĮU╦∙ęŖż¼żóż├ż┐żķMRI ó▄ ─┌─Ā╝▓╗╝?╣Ūš█żŽCT ? 2021 M.Okuyama Akita University Graduate School of Medicine