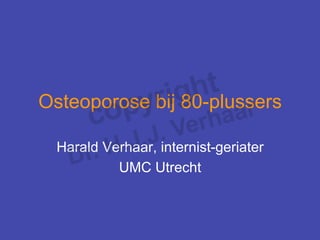























![Strontiumranelaat en heupfractuurrisico bij patiënten
(> 74 jaar en T-score < -3; n=1977, 40% TROPOS)
Patients (%) N = 1977
12
10
placebo
8 RR: - 36%
6
*
4
Strontium
ranelaat
2
0 Months
0 6 12 18 24 30 36 42
ITT, over 3 jaar: RR = 0.64 95% CI [0.412;0.997] * P= 0.046
Kaplan-Meier, Cox Model Rizzoli R. et al, Osteoporosis Int 2004; 15 (Suppl. 1):OC39](https://image.slidesharecdn.com/iwo-2011-11-18-haraldverhaar-111201031912-phpapp02/85/Osteoporose-bij-80-plussers-25-320.jpg)




































More Related Content
What's hot (15)
More from Stichting Interdisciplinaire Werkgroep Osteoporose (20)













Osteoporose bij 80-plussers
- 1. Osteoporose bij 80-plussers Harald Verhaar, internist-geriater UMC Utrecht
- 2. Vraag ŌĆóŌĆ» Is het ├╝berhaupt nog wel zinvol om een anti-osteoporose medicament voor te schrijven aan een 80-plusser (die frequent valt)? ŌĆóŌĆ» Weegt het vallen niet zwaarder dan het versterken van het bot met medicatie?
- 3. Can fall risk be incorporated into fracture risk assessment algorithms: a study of responsiveness to clodronate? Kayan E., McCloskey K. et al. Osteoporos Int. 2009 - The debate about the efficacy of skeletal therapies on fracture risk in women at increased risk of falling continues - We determined whether fall risk impeded the efficacy of clodronate to reduce osteoporotic fracture incidence - Methods: a post-hoc analysis of a 3-year placebo-controlled study of clodronate involving 5.212 women aged > 75. At entry, self-reported multiple falls in the previous month were documented - Results: clodronate reduced osteoporotic fracture incidence by 24% (HR) 0.76, 95% CI 0.63ŌĆō0.93). The efficacy was similar in women with recent multiple falls compared to those without (HR 0.61 vs. 0.77): next slide - Conclusion: fall risk does not significantly impact on the anti-fracture efficacy of clodronate. If confirmed with other agents, fall risk may be incorporated into risk assessment tools designed to target skeletal therapies
- 4. Impact clodronate on incidence of fractures in women with(out) a recent history of multiple falls or impaired mobility. Horzontal line is overall efficacy for clodonate on fractures
- 5. ŌĆóŌĆ» Wat is het risico op een nieuwe fractuur op SEH binnen 2 jaar na een eerste klinische fractuur voor een 80-jarige? ŌĆóŌĆ» Hoe vaak zijn daarbij ook multipele valrisicofactoren aanwezig?
- 6. Risico op nieuwe fractuur op SEH binnen 2 jaar na eerste fractuur Bij 15% geen valrisicofactoren aanwezig, 1 valrisicofactor bij 27%, 2 of meer valrisicofactoren bij 58% Van Helden S, Geusens P. Osteoporosis Int. 2006; 17: 348-354
- 7. Lee#ijd, ╠²BMD ╠²en ╠²risico ╠²op ╠²een ╠²heupfractuur ╠² Rela9ef ╠²risico: ╠²x2 ╠²per ╠²10 ╠²jaar ╠²toename ╠² Leeftijd (jaren) 10 jaars fractuurrisico (%) 20 80 70 10 60 50 0 -3 -2 -1 0 1 T-score Kanis et al, Bone, 2002
- 8. Casus ╠² ŌĆóŌĆ» Een 66-jarige vrouw komt op uw spreekuur met lage rugpijnklachten (acuut begonnen). Bij nader onderzoek wordt een fractuur van L1 (op X-LWK) gevonden. Er is geen valincident aan voorafgegaan ŌĆóŌĆ» Bij navraag wel 3x gevallen in afgelopen 12 maanden en een polsfractuur op 54-jarige leeftijd ŌĆóŌĆ» Er wordt ook een DEXA aangevraagd: FN T-score: -3.3
- 9. Fracture ╠²Calcula9on ╠²Tool ╠²(FRAX) ╠² ╠²hGp://www.shef.ac.uk/FRAX/
- 10. Fracture ╠²Risk ╠²Calculator ╠²van ╠²Garvan ╠² hGp://www.garvan.org.au/bone-┬ŁŌĆÉfracture-┬ŁŌĆÉrisk/ ╠² Dubbo ╠²Osteoporosis ╠²Epidemiology ╠²Study: ╠²n=2500 ╠²men ╠²and ╠²women ╠²> ╠²60 ╠²started ╠²in ╠²1989 ╠²
- 12. Tot op welke leeftijd zijn de verschillende ŌĆśanti-osteoporoseŌĆÖ medicamenten onderzocht m.b.t. fractuurreductie?
- 13. Literatuuroverzicht heupfractuurreductie Studies: prospectief, gerandomiseerd, dubbelblind, fractuur eindpunt (na = niet aangetoond) BOTAFBRAAK REMMERS Leeftijd Aantal patiënten RR over 1-3j Alendronaat FIT 1 55-81 2027 51% FIT2 54-81 4432 56% (4j) Raloxifen MORE 31-80 7705 na Ibandronaat BONE 55-80 2946 na Risedronaat HIP 70-79 5445 40% 80-85 3886 NS Zoledronaat HORIZON 65-89 3886 41% Denosumab (Freedom) 60-90 7868 40% ANABOLICA Fracture Prevention Trial (PTH1-34) 55-80 1637 na TOP trial (PTH 1-84) 45-94 2532 na DUBBELE WERKING Strontiumranelaat TROPOS 74-100 1977 36%* *posthoc
- 14. Hip Intervention Program Primair eindpunt: heupfractuurincidentie McClung, Geusens Piet et al, NEJM 2001 l’ü¼ŌĆ» 9497 postmenopauzale vrouwen; placebo of risedronaat (2.5 mg/ dag, 5 mg/dag) voor 3 jaar; bij inclusie 2 groepen: lage BMD (groep 1) of valrisicofactoren (groep 2) l’ü¼ŌĆ» 1000 mg Ca en tot 500 IE vit. D/ dag indien 25(OH)D3 < 40 nmol/l Groep 1 Groep 2 Lage Botmassa Klinische Risicofactoren 70-79 jaar oud > 80 jaar oud Femurhals T-Score < - 4 geen BMD vereiste of en > 1 Risicofactoren Femurhals T-Score < - 3 of plus >1 Risicofactoren Femurhals T-Score < - 4
- 15. Heupfractuurreductie in hele studiepopulatie (Groep 1 en 2) Controle Risedronaat 5 mg 5 4 30% patiënten (% ) p=0,02 3 2 1 0 0 6 12 18 24 30 36 Maanden 232 patiënten met een heupfractuur
- 16. Risedronaat en heupfractuurincidentie (-40%) bij osteoporotische vrouwen (groep 1) McClung et al, NEJM 2001
- 17. Risedronaat en heupfractuurincidentie bij vrouwen (80+) met alleen valrisicofactoren 6 Patients with Hip Fracture (%) 5 -8% Control NS 4 3 2 Risedronate 1 0 0 12 24 36 Month 131 ╠²pa9├½nten ╠²met ╠²heupfractuur ╠² McClung ╠²M, ╠²Geusens ╠²P. ╠²et ╠²al, ╠²NEJM, ╠²2001, ╠²333 ╠²
- 18. Heupfractuurreductie in groep boven de 80 jaar (groep 2) (voornamelijk geincludeerd o.b.v. valrisicofactoren; slechts 16% o.b.v. lage BMD) Control RIS 12 25% CI=(-31,57%) 10 p=0.14 8% % incidence 8 CI=(-35,36%) 8% 6 p=ns CI=(-80,35%) p=0.75 4 43/1313 78/2573 21/316 31/625 22/997 47/1948 2 0 Group 2 Low BMD Risk Factors
- 19. Klinische risicofactoren: voornamelijk valgerelateerd bij inclusie (Groep 2) Het hebben van minimaal 1 risicofactor was genoeg voor inclusie in de studie! Klinische risicofactoren: 84% moeilijkheden met staan l’ü¼ŌĆ» 34% onzekere l’ü¼ŌĆ» gang 31% trauma l’ü¼ŌĆ» na val in de afgelopen 12 maanden 22% heupfractuur l’ü¼ŌĆ» moeder 13% eerder l’ü¼ŌĆ» doorgemaakte heupfractuur 11% l’ü¼ŌĆ»roken 27% Femurhals BMD < - 4: 16%
- 20. Limitations HIP-study ŌĆóŌĆ» The individual risk factors were not recorded in sufficient detail ŌĆóŌĆ» Loss to follow-up was quite substantial (complete data only available in 58% of the participants) ŌĆóŌĆ» Those lost to follow-up had a higher prevalence of risk factors for fracture incl. being older, lighter and smoking more
- 21. Fracture reduction by risedronate in elderly > 80 years Boonen ╠²S ╠²et ╠²al, ╠²JAGS, ╠²2004 ╠² ŌĆóŌĆ» Risk for vertebral fractures: ŌĆōŌĆ» After 1 yr: -81%* *p<0.01 ╠² ŌĆōŌĆ» After 3 yr: -44%* ŌĆóŌĆ» Risk for non-vertebral fractures: - < 80 years: -21%* *p<0.01 ╠² - > 80 years: -14% Pooled analysis of data from 3RCTŌĆÖs: Hip Intervention Program (HIP), Vertebral Efficacy with Risedronate Therapy-Multinational (VERT-MN), and VERT-North America (NA): Placebo (n=688) or risedronate 5 mg/d (n=704) for up to 3 years
- 22. Geen reductie non-vertebrale fracturen met risedronaat - It is possible that the reduced effect of treatment on non-vertebral fractures in pat > 80 may reflect the increasing influence of nonskeletal risk factors for these types of fractures, such as falling, with increasing age - In the current study, the frequency of comorbidities, including conditions likely to increase patients' risk of falling, was significantly higher in pat > 80 - Although falls in this age group were not assessed, it is likely that pat > 80 were at greater risk of falling because of their higher prevalence of comorbidities - It is also possible that this increase in fall risk may have offset the benefit of antiresorptive intervention on skeletal strength - Inadequate statistical power is likely to have contributed to the failure to demonstrate a significant effect. Under the assumption that the treatment effect in women > 80 would be similar to that in women younger than 80 (a 21% reduction in nonvertebral fracture risk), this trial had only 30% power to show an effect in these oldest patients
- 23. Alendronaat en heupfractuur tussen 55 en 81 jaar Black et al, Lancet 1996
- 24. Fractuurpreventie met alendronaat volgens leeftijd Heup: ╠²RR: ╠²00.47 Hip RR: .47 ╠² Clinical spine RR:RR: ╠²0.55 ╠² Klinische ╠²wervel: ╠² 0.55 Pols: ╠²RR: ╠²0.69 ╠² Wrist RR: 0.69 Alle: ╠²RR: ╠²00.60 All RR: .60 ╠² Hochberg ╠²M, ╠²Geusens ╠²P, ╠²et ╠²al, ╠²JBMR, ╠²2005, ╠²971 ╠²
- 25. Strontiumranelaat en heupfractuurrisico bij patiënten (> 74 jaar en T-score < -3; n=1977, 40% TROPOS) Patients (%) N = 1977 12 10 placebo 8 RR: - 36% 6 * 4 Strontium ranelaat 2 0 Months 0 6 12 18 24 30 36 42 ITT, over 3 jaar: RR = 0.64 95% CI [0.412;0.997] * P= 0.046 Kaplan-Meier, Cox Model Rizzoli R. et al, Osteoporosis Int 2004; 15 (Suppl. 1):OC39
- 26. Niet-┬ŁŌĆÉwervel ╠²fractuureduc0e ╠²bij ╠²pa0├½nten ╠² ╠² tussen ╠²80 ╠²en ╠²100 ╠²jaar ╠²oud ╠² (n=1488, ╠²SOTI ╠²en ╠²TROPOS ╠²gepooled) Ten gunste van strontiumranelaat Ōåō RR Na 1 jaar NNT=36 - 41% Alle niet-wervel fracturen P=0.027 Na 3 jaar NNT=18 - 31% Alle niet-wervel fracturen P=0.011 Na 5 jaar NNT=25 - 26% Alle niet-wervel fracturen P=0.019 0 0.5 1 1.5 t.o.v. placebo Seeman E et al. Osteoporos Int. 2006;18:1-13 (OC39).
- 27. Denosumab: ╠²baseline ╠²Characteris0cs ╠²of ╠²the ╠²Subjects ╠² Cummings SR et al. N Engl J Med 2009;361:756-765
- 28. Reduction of hip fracture risk is age-dependent The FREEDOM Trial ŌĆō post-hoc analyses by age In the FREEDOM study the risk of vertebral fracture was reduced in the overall study population by 68% (p<0.001) and the risk of hip fracture reduced by 40% (p =0.04) General Incidence Vertebral fracture Hip fracture Placebo Denosumab Vertebral Fractures Hip Fractures 400 General population Incidence per 10,000 women per year 300 200 100 0 Adapted from Rizzoli R. et al. Osteoporosis Intl Supl 2010 ŌĆō abstract P841; Adapted from Sambrook P & Cooper C. Lancet 2006;367:2010-2018 Boonen S et al J Clin Endocrinol Metab. 2011 Jun;96(6):1727-36
- 29. Incidentie tweede heupfractuur? De cumulatieve incidentie van een tweede heupfractuur is: ŌĆōŌĆ»5% in het eerste jaar na de eerste heupfractuur ŌĆōŌĆ»8% in het tweede jaar na de eerste heupfractuur Lonnroos et al. Osteoporos Int 2007
- 30. Afname mortaliteit met zoledronaat na heupfractuur (Lyles et al., N Engl J Med 2007;357)
- 31. Conclusies over effectiviteit bij ouderen ŌĆóŌĆ» Risedronaat geen duidelijk effect op heupfracturen en non- vertebrale fracturen boven de 80 jaar aangetoond ŌĆóŌĆ» Alendronaat heeft een effect op fractuurreductie (non)-vert./ heup) aangetoond tot 85 jaar ŌĆóŌĆ» Zoledronaat heeft een effect op fractuurreductie (non)vert./ heup) aangetoond tot 94 jaar ŌĆóŌĆ» Denosumab heeft alleen een effect op heupfractuurreductie boven de 75 jaar (niet bij <75 jaar). Tot 90 jaar effectief mbt (non)vertebrale # ŌĆóŌĆ» Strontiumranelaat heeft bij 74-plussers met een BMD < -3 heupfractuurreductie aangetoond, en van (non)-vertebrale # tot 100 jaar ŌĆóŌĆ» Fractuurreductie-effecten anti-osteoporose middelen lijken niet negatief te worden be├»nvloed door frequente valincidenten en kunnen dus ook bij die groep worden ingezet