







































More Related Content
What's hot (20)
Viewers also liked (10)

![Bonaldi[1]](https://cdn.slidesharecdn.com/ss_thumbnails/bonaldi1-091219192130-phpapp02-thumbnail.jpg?width=560&fit=bounds)






Similar to Colpocele anteriore recidivante: riparazione fasciale vs protesica (20)




















More from GLUP2010 (20)




















Colpocele anteriore recidivante: riparazione fasciale vs protesica
- 1. Colpocele anteriore recidivante : riparazione fasciale vs protesica R. Baccichet
- 2. Il razionale della Mesh in chirurgia pelvica • Terapia di supporto? • Terapia di sostituzione ? • L’obiettivo è quello di aumentare la LONGEVITÀ della riparazione chirurgica
- 3. principi biochimici che guidano l’outcome chirurgico • Aggiungere del materiale protesico al tessuto connettivo danneggiato ne aumenta la resistenza tensile ma ne riduce la flessibilità per la reazione cicatriziale e la caratteristica anelasticità delle mesh • Nonostante il raccorciamento tipico della mesh ( 25% ) il materiale protesico incluso nel tessuto aumenta di gran lunga la resistenza ai carichi cronici compensando la degenerazione del collagene
- 9. FDA Safety Communication: UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ Prolapse Date Issued: July 13, 2011
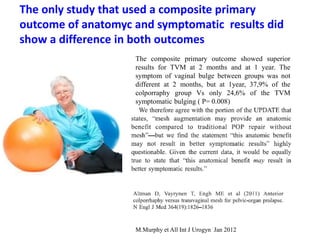
- 11. M.Murphy et All Int J Urogyn Jan 2012 The only study that used a composite primary outcome of anatomyc and symptomatic results did show a difference in both outcomes The composite primary outcome showed superior results for TVM at 2 months and at 1 year. The symptom of vaginal bulge between groups was not different at 2 months, but at 1year, 37,9% of the colporraphy group Vs only 24,6% of the TVM symptomatic bulging ( P= 0.008)
- 12. FDA Safety Communication: UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ Prolapse Date Issued: July 13, 2011 Erosion Sexual function Pain
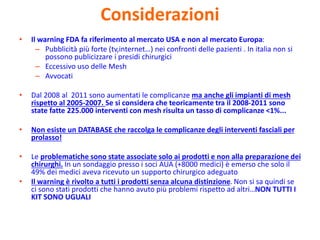
- 13. Considerazioni • Il warning FDA fa riferimento al mercato USA e non al mercato Europa: – Pubblicità più forte (tv,internet…) nei confronti delle pazienti . In italia non si possono publicizzare i presidi chirurgici – Eccessivo uso delle Mesh – Avvocati • Dal 2008 al 2011 sono aumentati le complicanze ma anche gli impianti di mesh rispetto al 2005-2007. Se si considera che teoricamente tra il 2008-2011 sono state fatte 225.000 interventi con mesh risulta un tasso di complicanze <1%... • Non esiste un DATABASE che raccolga le complicanze degli interventi fasciali per prolasso! • Le problematiche sono state associate solo ai prodotti e non alla preparazione dei chirurghi. In un sondaggio presso i soci AUA (+8000 medici) è emerso che solo il 49% dei medici aveva ricevuto un supporto chirurgico adeguato • Il warning è rivolto a tutti i prodotti senza alcuna distinzione. Non si sa quindi se ci sono stati prodotti che hanno avuto più problemi rispetto ad altri…NON TUTTI I KIT SONO UGUALI
- 14. Across the board, the risk of mesh erosion might be higher with TVM butin two large multicentric trials conducted by surgeons who perform the index surgery an a regular basis, the result of the abdominal and vaginalapproach are quite similar. In the TVM trial thet randomized 400 subjects, 3,2% had undergone a procedure to correct mesh erosion at 12 months
- 15. More than half of most exposures from TVM are ASYMPTOMATIC, 1/3 need only minor outpatient operative intervention
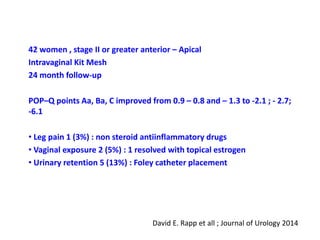
- 17. David E. Rapp et all ; Journal of Urology 2014 42 women , stage II or greater anterior – Apical Intravaginal Kit Mesh 24 month follow-up POP–Q points Aa, Ba, C improved from 0.9 – 0.8 and – 1.3 to -2.1 ; - 2.7; -6.1 • Leg pain 1 (3%) : non steroid antiinflammatory drugs • Vaginal exposure 2 (5%) : 1 resolved with topical estrogen • Urinary retention 5 (13%) : Foley catheter placement
- 18. Mert Turgol et all; Europea Journal Obst – Gyn 2013 20 patients anterior colporraphy 20 patients polypropylene mesh Follow-up 12 months Anatomical cure rate: - 73% colporraphy - 95% mesh De novo stress incontinence: 1 in anterior colporraphy Mesh erosion: 3 (15%)
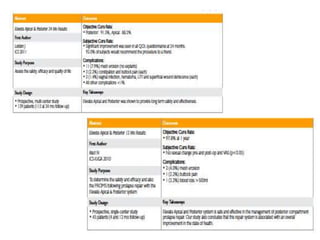
- 19. Josè Tamanini et all; Journal of urology 2015 Randomized controlled trial 100 women with II or grater anterior vaginal wall prolapse Anterior colporraphy vs mesh insertion • At 24 months follow-up significatly improved in the mesh group • Asymptomatic mesh exposure in 7 patient ( 16%) • Vaginal and urinary symptom and quality of life improved postoperatively in each group
- 20. Conclusioni • Penso: ...maggiore esperienza e consapevolezza • Penso: ...miglioramento di tecnica e materiali • Penso: ...valida arma terapeutica • Penso: ...autorizzati ad una visione più ottimistica