



![Kanser Tedavileri ile Kemik Kayb─▒ 1. Kanis JA. The European Foundation for Osteoporosis and Bone Disease. Osteoporos Int. 1997;7:390-406. 2. Eastell R, et al. J Bone Miner Res. 1990;5:1237-1241. 3. Maillefert JF, et al. J Urol. 1999;161:1219-1222. 4. Gnant M, et al. Lancet Oncol. 2008;9:840-849. 5. Shapiro CL, et al. J Clin Oncol. 2001;19:3306-3311. 1. Y─▒lda Kemik Kayb─▒ (%) Do─¤al Geli┼¤en Kemik Kayb─▒ Kanser Tedavisi ─░li┼¤kili Kemik Kayb─▒ 0 2 4 6 8 10 Normal Erkek [1] Postmenop ozak Kad─▒n [1] Menopozal kad─▒n [1] Al T tedavisinde Postmenop ozal Kad─▒n [2] ADT [3] Al Te davisi + GnRH agonist Premenop ozal Kad─▒n [4] Kemoterapiye sekonder Prematur Menop oz [5] 0.5 1.0 2.0 2.6 4.6 7.0 7.7](https://image.slidesharecdn.com/memecaosteoporoz2011-110326103119-phpapp02/85/Osteoporoz-Sercan-Aksoy-5-320.jpg)






![Steroidal ve Non - steroidal AI Tmx g├Čre K─▒r─▒k riskini art─▒r─▒yor Tamoxifen Letrozole Anastrozole Pla s ebo K─▒r─▒klar (%) 11.0 7.7 5.7 4.0 5.3 4.6 7.0 5.0 P < .0001 P < .001 0 2 4 6 8 10 12 14 P = .003 P = .25 Exemestane ATAC [1] (68 Ay ) IES [2] (58 Ay ) BIG 1-98 [3] (26 Ay ) MA.17 [4] (30 Ay ) 1. Howell A, et al. Lancet. 2005;365:60-62. 2. Coleman RE, et al. Lancet Oncol. 2007;8:119-127. 3. Th├╝rlimann B, et al. N Engl J Med. 2005;353:2747-2757. 4. Goss PE, et al. J Natl Cancer Inst. 2005;97:1262-1271.](https://image.slidesharecdn.com/memecaosteoporoz2011-110326103119-phpapp02/85/Osteoporoz-Sercan-Aksoy-12-320.jpg)








![E/Z/ZO-FAST ├ćal─▒┼¤malar─▒nda K─▒r─▒klar (3 ├ćal─▒┼¤ma ) 36 ay─▒n ├╝zerinde tedavi alan ve up-fron ZA kullanan hastalarda k─▒r─▒k geli┼¤imi gecikmi┼¤ ZA kullananlara g├Čre daha d├╝┼¤├╝k 1. Brufsky AM, et al. Clin Breast Cancer. 2009;9:77-85. 2. Eidtmann H, et al. Ann Oncol. 2010;[Epub ahead of print]. 3. Llombart A, et al. ECCO 2007. Abstract 2044. K─▒r─▒k , % ├ćal─▒┼¤ma Ay Up-front ZOL Gecikmi┼¤ ZOL Z-FAST [1] 36 5.7 6.3 ZO-FAST [2] 36 5.0 6.0 E-ZO-FAST [3] 12 0.8 1.9](https://image.slidesharecdn.com/memecaosteoporoz2011-110326103119-phpapp02/85/Osteoporoz-Sercan-Aksoy-21-320.jpg)

![ZO-FAST 48 Ay : Up-front Z A Belirgin olarak DFS olaylar─▒ riskini %41 azalt─▒r Gecikmi┼¤ Z A (n = 532) Up-front Z A (n = 532) 50 45 40 35 30 25 20 15 10 5 Patients (n) 3 5 20 30 10 2 Rek├╝rrens (36 Ay ) [2] * 1. Coleman R, et al. SABCS 2009. Abstract 4082. 2. Eidtmann H, et al. Ann Oncol. 2010;[Epub ahead of print]. Lo kal Uzak L enf nodu 0 1.0 0.8 0.6 0.4 0.2 0 0 6 36 42 48 54 60 66 Study Mo Survival Distribution Function Z A 4 mg up-front Z A 4 mg gecikmi┼¤ 12 18 24 30 Up-front Gecikmi┼¤ Patients, n 532 533 Events/censored 32/500 53/480 Median follow-up 48.0 48.1 HR (95% CI) 0.59 (0.38-0.92) Up-front vs delayed log rank P value .0175 DFS at Median Follow-up 48 Mos [1] *Multiple sites of metastases may be reported for the same patient. Sites of distant metastases include bone, brain, liver, lung, skin, lymph node, and other.](https://image.slidesharecdn.com/memecaosteoporoz2011-110326103119-phpapp02/85/Osteoporoz-Sercan-Aksoy-23-320.jpg)






![Does adjuvant bisphosphonate in early breast cancer modify the natural course of the disease? A meta-analysis of randomized controlled trials. Bifosfonat vs Tedavi YOK (Ocak 2009 ) 13 ├¦al─▒┼¤ma (n= 6886 ) bi fosfonat (n = 3414) vs Tedavi YOK (n = 3472). Mortalite [OR], 0.70; 95% CI, 0.48-1.04; P = .079), Kemik metastaz─▒ (OR, 0.92; 95% CI, 0.76-1.11; P = .413), Toplam n├╝ks (OR, 0.84; 95% CI, 0.60-1.18; P = .321), Uzak metastaz (OR, 0.89; 95% CI, 0.67-1.19; P = .453), V iseral rek├╝rrens (OR, 1.05; 95% CI, 0.68-1.60; P = .820), L o k al relaps (OR, 1.056; 95% CI, 0.750-1.487; P = .756). J Natl Compr Canc Netw. 2010 Mar;8(3):279-86.](https://image.slidesharecdn.com/memecaosteoporoz2011-110326103119-phpapp02/85/Osteoporoz-Sercan-Aksoy-30-320.jpg)




































More Related Content
What's hot (20)
Viewers also liked (9)







Similar to Osteoporoz - Sercan Aksoy (20)




















More from ankaramhd (20)




















Osteoporoz - Sercan Aksoy
- 1. Erken Evre Meme Kanseri Tedavisinde Yan Etkiler: OSTEOPOROZ Dr. Sercan Aksoy Ankara Numune E─¤itim ve Ara┼¤t─▒rma Hastanesi T─▒bbi Onkoloji Klini─¤i 26 MART 2011, MEME KANSER─░ VE HORMONLAR KURSUANKARA
- 2. Kemik Kayb─▒ & Osteoporoz D├╝┼¤├╝k Kemik Kitlesi Sex Hormon Eksikli─¤i ├¢strojen eksikli─¤i Androjen eksikli─¤i Ya┼¤ Beslenme bozuklu─¤u
- 3. Kemik Mineral Dansitometrisi ├¢l├¦├╝mlerine G├Čre Osteopeni ve Osteoporoz i├¦in Tan─▒ S─▒n─▒flamas─▒ Data from The World Health Organization Assessment of osteoporosis at the primary health care level. Summary report of a WHO Scientific Group. 2007; WHO, Geneva Kemik Kitlesi (T skoru) Normal Ōēź -1 D├╝┼¤├╝k Kemik Kitlesi (osteopeni) 1 ile -2.5 aras─▒ Osteoporoz Ōēż -2.5 Yerle┼¤mi┼¤ Osteoporoz Ōēż -2.5 + osteoporotik k─▒r─▒k
- 4. Tedavi ili┼¤kili Kemik Kayb─▒ Nedenleri Kemik kayb─▒ GnRH agonist leri Bilateral oo ferektomi Bilateral or ┼¤iektomi Kemoterapiye ba─¤l─▒ o v er yetmezli─¤i Artm─▒┼¤ kemik turnover ─▒ Pfeilschifter J, et al. J Clin Oncol. 2000;18:1570-1593. Theriault RL. Oncology (Williston Park). 2004;18(5 suppl 3):11-15. Dempster DW. Osteoporos Int. 2003;14 suppl 5:S54-S56. Azalm─▒┼¤ kemik kalitesi Aromata z inhibit ├Črleri Glu kokortikoidler H i pogonadi zm
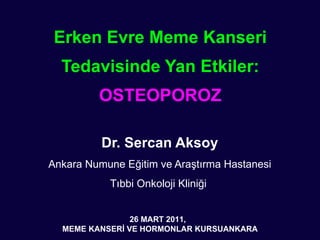
- 5. Kanser Tedavileri ile Kemik Kayb─▒ 1. Kanis JA. The European Foundation for Osteoporosis and Bone Disease. Osteoporos Int. 1997;7:390-406. 2. Eastell R, et al. J Bone Miner Res. 1990;5:1237-1241. 3. Maillefert JF, et al. J Urol. 1999;161:1219-1222. 4. Gnant M, et al. Lancet Oncol. 2008;9:840-849. 5. Shapiro CL, et al. J Clin Oncol. 2001;19:3306-3311. 1. Y─▒lda Kemik Kayb─▒ (%) Do─¤al Geli┼¤en Kemik Kayb─▒ Kanser Tedavisi ─░li┼¤kili Kemik Kayb─▒ 0 2 4 6 8 10 Normal Erkek [1] Postmenop ozak Kad─▒n [1] Menopozal kad─▒n [1] Al T tedavisinde Postmenop ozal Kad─▒n [2] ADT [3] Al Te davisi + GnRH agonist Premenop ozal Kad─▒n [4] Kemoterapiye sekonder Prematur Menop oz [5] 0.5 1.0 2.0 2.6 4.6 7.0 7.7
- 6. ╠²
- 7. Aromataz ─░nhibit├Črleri Klasifikasyonu Ku┼¤ak Tip I (Steroidal) Tip II (Non-Steroidal) Birinci YOK Aminoglutethimide ─░kinci Formestane Fadrozole Rogletimide ├£├¦├╝nc├╝ Exemestane ( Aromasin ) Anastrozole Letrozole Vorozole
- 8. ╠²
- 9. Letrozole Suppresses Plasma Estradiol and Estrone Sulphate More Completely Than Anastrozole in Postmenopausal Women With Breast Cancer J Clin Oncol 2008
- 10. Letrozole reduces plasma E2 and E1S levels to a significantly greater extent than anastrozole in postmenopausal women taking AIs as part of their adjuvant therapy for hormone receptorŌĆōpositive breast cancer.
- 11. Serum E stradiol ve K─▒r─▒k Riski Serum estradiol concentrations at base line and age-adjusted risk of subsequent hip or vertebral fracture in postmenopausal women over the age of 64 years. Compared to the reference group of the women with undetectable serum estradiol concentrations (below 5 pg/mL), those with higher baseline serum estradiol concentrations had a significantly lower relative risk of fracture of 0.3 to 0.5. To convert serum estradiol values to pmol/L, multiply by 3.67 Cummings, et al . N Engl J Med 1998; 339:733.
- 12. Steroidal ve Non - steroidal AI Tmx g├Čre K─▒r─▒k riskini art─▒r─▒yor Tamoxifen Letrozole Anastrozole Pla s ebo K─▒r─▒klar (%) 11.0 7.7 5.7 4.0 5.3 4.6 7.0 5.0 P < .0001 P < .001 0 2 4 6 8 10 12 14 P = .003 P = .25 Exemestane ATAC [1] (68 Ay ) IES [2] (58 Ay ) BIG 1-98 [3] (26 Ay ) MA.17 [4] (30 Ay ) 1. Howell A, et al. Lancet. 2005;365:60-62. 2. Coleman RE, et al. Lancet Oncol. 2007;8:119-127. 3. Th├╝rlimann B, et al. N Engl J Med. 2005;353:2747-2757. 4. Goss PE, et al. J Natl Cancer Inst. 2005;97:1262-1271.
- 13. AI ili┼¤kili Kemik Kayb─▒n─▒n ├¢nlenmesi ve ├¢nlenmesi ve Tedavisi Non- farmakolojik ╠² Ya┼¤am stili de─¤i┼¤ikli─¤i Fiziksel aktivite ’éŁ Sigara ’é» Kalsiyum ve vitamin D suplemantasyonu
- 14. AI ili┼¤kili Kemik Kayb─▒n─▒n ├¢nlenmesi ve ├¢nlenmesi ve Tedavisi Farmakolojik ╠² -Bifosfonatlar -Denosumab
- 15. SABRE: Risedronate ile AI ili┼¤kili Kemik Kayb─▒n─▒n ├¢nlenmesi * P values from paired t-test for open-label, noncomparative groups. ŌĆĀ P values from ANCOVA in favor of anastrozole plus risedronate. Anastrozole D├╝┼¤├╝k Risk (n = 26) Orta Risk (n = 114) Anastrozole+ Pla s ebo Anastrozole + Risedronate Anastrozole + Risedronate Y├╝ksek Risk (n = 33) % De─¤i┼¤iklik KMD Bazal de─¤erlendirmeden 24 Ay P = .0109* P = .5988* P = .0006* P = .0104* P < .0001 ŌĆĀ P < .0001 ŌĆĀ -2.0 -1.0 0 1.0 2.0 3.0 4.0 5.0 -3.0 Lumbar vertebra Total Kal├¦a Van Poznak C, et al. J Clin Oncol. 2010;28:967-975.
- 16. ABCSG-12 ├ćal─▒┼¤ma Dizayn─▒ Hasta kabul├╝: 1999-2006 1803 premenop ozal meme kanseri Hormon resept├Čr├╝ pozitif Evre I ve II, < 10 po zitif lenf nodu Neoadjuvant kemoterapi haricinde kemoterapi YOK Tedavi s├╝resi 3 y─▒l Randomize Cerrahi (+ RT) Tamoxifen 20 mg/ g├╝n Goserelin 3.6 mg q28d Anastrozole 1 mg/ g├╝n + Zoledronic Acid 4 mg q6m Anastrozole 1 mg/ g├╝n Tamoxifen 20 mg/ g├╝n + Zoledronic Acid 4 mg q6m Gnant M, et al. N Engl J Med . 2009;360:679-691.
- 17. Adjuvan Endo krin Tedavi ┬▒ Zoledroni k Asit: KMDŌĆÖde de─¤i┼¤iklik Gnant M, et al. Lancet Oncol. 2008;9:840-849. 10 5 0 -5 -10 -15 Percent Change in Lumbar Spine BMD (g/cm 2 ) From Baseline Ay Ay Ay Ay Zoledroni k A sit YOK Tamoxifen Anastrozole 36 60 -9.0 P < .0001 -4.5 NS -13.6 P < .0001 -7.8 P = .003 36 60 36 60 36 60 Zoledroni k A s i t Tamoxifen Anastrozole +1.0 NS +5.2 P = .04 -0.1 NS +3.1 NS
- 18. Brufsky, A. M. Oncologist 2008;13:187-195 Figure 2. Patients with normal bone mineral density, osteopenia, or osteoporosis in the lumbar spine treated with goserelin and anastrozole without (A) or with (B) zoledronic acid, which resulted in significantly better T-scores than with hormone therapy alone ( p < .0001 )
- 19. Z-FAST/ZO-FAST/E-ZO-FAST Letrozole ├¢nemli Noktalar: Primer : BMD Sekonder : Kemik mark─▒rlar─▒ , k─▒r─▒k , zaman rek├╝rrens Letrozole + Zoledroni k A sit 4 mg q6mo 2193 Evre I-IIIA meme kanserli hasta Postmenopozal veya kanser tedavisine ba─¤l─▒ amenore HR pozitif T-skoru Ōēź -2 SD Gecikmi┼¤ Zoledroni k A sit A┼¤a─¤─▒dakilerden biri geli┼¤irse : KMD T-score < -2 SD Klinik k─▒r─▒k 36. Ayda as s emptomatiik kr─▒k T edavi S├╝resi 5 y ─▒l R
- 20. Z-FAST: Up-front Z A Lomber vertebra ve kal├¦a BMD (KMD) art─▒r─▒r (N = 602) 1.96% * P values correspond to intergroup comparisons. ŌĆĀ Intragroup comparisons from baseline to all time points for all treatment groups were significant ( P Ōēż .0003 for all). L omber Vertebra Mean (SEM) Percent Change in BMD Up-front Z A 4 mg/6 ay Delayed ZOL 4 mg/6 ay Brufsky A, et al. SABCS 2009. Abstract 4083. P < .0001, all time points* ŌĆĀ 8 6 4 2 0 -2 -4 -6 Mos 12 24 36 48 61 3.14% 3.85% 4.64% 6.19% -2.33% -2.89% -2.99% -3.05% -2.42% Ōłå 4.29% Ōłå 6.03% Ōłå 6.84% Ōłå 7.69% Ōłå 8.61% 1.26% Total Kal├¦a P < .001, all time points* ŌĆĀ 4 3 2 1 0 -1 -4 -6 Mos 12 24 36 48 61 1.41% 1.68% 1.70% 2.57% -1.88% -3.15% -3.46% -4.02% -4.12% Ōłå 3.14% Ōłå 4.56% Ōłå 5.14% Ōłå 5.72% Ōłå 6.69% -2 -3 -5
- 21. E/Z/ZO-FAST ├ćal─▒┼¤malar─▒nda K─▒r─▒klar (3 ├ćal─▒┼¤ma ) 36 ay─▒n ├╝zerinde tedavi alan ve up-fron ZA kullanan hastalarda k─▒r─▒k geli┼¤imi gecikmi┼¤ ZA kullananlara g├Čre daha d├╝┼¤├╝k 1. Brufsky AM, et al. Clin Breast Cancer. 2009;9:77-85. 2. Eidtmann H, et al. Ann Oncol. 2010;[Epub ahead of print]. 3. Llombart A, et al. ECCO 2007. Abstract 2044. K─▒r─▒k , % ├ćal─▒┼¤ma Ay Up-front ZOL Gecikmi┼¤ ZOL Z-FAST [1] 36 5.7 6.3 ZO-FAST [2] 36 5.0 6.0 E-ZO-FAST [3] 12 0.8 1.9
- 22. ABCSG-12: Z A belirgin olarak DFS art─▒r─▒r ( %36 ) 100 90 80 70 60 50 40 30 20 10 0 0 12 24 36 48 60 72 84 Randomizasyon sonras─▒ s├╝re (Ay) DFS (%) HR (95% CI) Olay , n vs No ZOL P Value Z A 54 0.64 (0.46-0.91) .01 Z A YOK 83 Z A YOK Z A Gnant M, et al. N Engl J Med. 2009;360:679-691. Copyright ┬® 2009 Massachusetts Medical Society. All rights reserved. Ortanca takip s├╝resi : 48 Ay Olaylar (n) 10 10 9 6 29* 41* 20 10 83 54 * ZA Yok grupta 23 , ZA grupta 16 kemik metastaz─▒n─▒ da i├¦eriri 100 90 80 70 60 50 40 30 20 10 0 ─░kincil kanser Kontrolateral MK Uzak Lo korejyonel
- 23. ZO-FAST 48 Ay : Up-front Z A Belirgin olarak DFS olaylar─▒ riskini %41 azalt─▒r Gecikmi┼¤ Z A (n = 532) Up-front Z A (n = 532) 50 45 40 35 30 25 20 15 10 5 Patients (n) 3 5 20 30 10 2 Rek├╝rrens (36 Ay ) [2] * 1. Coleman R, et al. SABCS 2009. Abstract 4082. 2. Eidtmann H, et al. Ann Oncol. 2010;[Epub ahead of print]. Lo kal Uzak L enf nodu 0 1.0 0.8 0.6 0.4 0.2 0 0 6 36 42 48 54 60 66 Study Mo Survival Distribution Function Z A 4 mg up-front Z A 4 mg gecikmi┼¤ 12 18 24 30 Up-front Gecikmi┼¤ Patients, n 532 533 Events/censored 32/500 53/480 Median follow-up 48.0 48.1 HR (95% CI) 0.59 (0.38-0.92) Up-front vs delayed log rank P value .0175 DFS at Median Follow-up 48 Mos [1] *Multiple sites of metastases may be reported for the same patient. Sites of distant metastases include bone, brain, liver, lung, skin, lymph node, and other.
- 24. Denosumab: RANK ŌĆÖ─▒ inhibe Eder RANKL ŌĆÖa kar┼¤─▒ y├╝ksek afinite ile ba─¤lanan monoklonal antikor. SC olarak uygulan─▒r Spe sifiktir: TNF- ╬▒ , TNF- ╬▓ , TRAIL veya CD40L ba─¤lanmaz Osteoklast olu┼¤umu ve aktivasyonunu inhibe eder
- 25. AI- Ba─¤l─▒ Kemik Kayb─▒n─▒n Denosumab ile ├¢nlenmesi Ellis GK, et al. J Clin Oncol. 2008;26:4875-4882. Percent Change in BMD From Baseline at Lumbar Spine 8 7 6 5 4 3 2 1 0 -1 -2 -3 1 3 6 12 24 Mos 5.5% Fark 12 . Ay 7.4% Fark 24 . Ay * P < .0001 vs placebo Pla s ebo (n = 122) Denosumab (n = 123) * * * * *
- 26. Lack of evidence for fracture prevention in early breast cancer bisphosphonate trials: A meta-analysis Gynecologic Oncology 117 (2010) 139ŌĆō145 n= 7461 Bifosfonat (n= 3691 ) vs Tedavi Yok (n= 3770 )
- 27. ╠²
- 28. ╠²
- 29. ╠²
- 30. Does adjuvant bisphosphonate in early breast cancer modify the natural course of the disease? A meta-analysis of randomized controlled trials. Bifosfonat vs Tedavi YOK (Ocak 2009 ) 13 ├¦al─▒┼¤ma (n= 6886 ) bi fosfonat (n = 3414) vs Tedavi YOK (n = 3472). Mortalite [OR], 0.70; 95% CI, 0.48-1.04; P = .079), Kemik metastaz─▒ (OR, 0.92; 95% CI, 0.76-1.11; P = .413), Toplam n├╝ks (OR, 0.84; 95% CI, 0.60-1.18; P = .321), Uzak metastaz (OR, 0.89; 95% CI, 0.67-1.19; P = .453), V iseral rek├╝rrens (OR, 1.05; 95% CI, 0.68-1.60; P = .820), L o k al relaps (OR, 1.056; 95% CI, 0.750-1.487; P = .756). J Natl Compr Canc Netw. 2010 Mar;8(3):279-86.
- 31. Does adjuvant bisphosphonate in early breast cancer modify the natural course of the disease? A meta-analysis of randomized controlled trials. ZA &Rek├╝rrens (OR, 0.67; 95% CI, 0.47-0.95; P = .025). ZA &Mortalite (OR, 0.64; 95% CI, 0.38-1.06) ZA&Kemik metastazlar─▒ (OR, 0.66; 95% CI, 0.37-1.15). Bifosfonatlar─▒n adjuvan kullan─▒m─▒ hastal─▒─¤─▒n do─¤al seyrinde farkl─▒l─▒k g├Čstermemektedir J Natl Compr Canc Netw. 2010 Mar;8(3):279-86.
- 32. Vitamin D Eksikli─¤i & Meme Kanseri n= 407 Evre I-III Meme Kanseri Ortanca ya┼¤ 49.1 ┬▒ 11.7. % 50 premenop o sal V itamin D Seviyeleri Eksikli─¤i % 54 (< 10 ng/mL), Yetersizli─¤i % 3 4 (10 - 25 ng/mL), Yeterli % 12 (25-80 ng/mL Altundag ve Ark 2010 ASCO
- 33. Meme Kanseri Bayanlarda KMD takibi i├¦in ASCO Klavuzu ├¢nerileri ASCO: American Society of Clinical Oncology; AI: aromatase inhibitor. Reproduced with permission from: Pant, S, Shapiro, CL. Aromatase inhibitor-associated bone loss. Drugs 2008; 68:2591. Copyright ┬®2008 Adis Data Information BV. KMD i├¦in ─░ndikasyonlar: > 65 ya┼¤ bayan 60 - 64 ya┼¤─▒nda olan years with the one or more of the following: Ailede Osteoporoz ├Čyk├╝s├╝ D├╝┼¤├╝k v├╝cut a─¤─▒rl─▒─¤─▒( < 70 kg ) Travmatik olmayan k─▒r─▒k ├Čyk├╝s├╝ Di─¤er risk fakt├Črleri sedentar ya┼¤am, sigara AI kullanan postmenopozal hasta Premenop o sal hasta tedaviye ba─¤l─▒ erken menopoz
- 34. Tedaviye Ba─¤l─▒ Kemik Kayb─▒n─▒ ├¢nlemek ─░├¦in Pratik ├¢neriler T- sk or u Ōēź -2.0, R isk fa kt├Čr├╝ YOK Risk Durumunu ve KMD her 1-2 y─▒lda de─¤erlendir * K al s i y um ve vitamin D supplement asyonu Hadji P, et al. Ann Oncol. 2008;19:1407-1416 by permission of Oxford University Press. Risk Fakt├Črlerinden herhangi 2ŌĆÖsinin olmas─▒ : T-s k or u < -1.5 Ōēź 65 ya┼¤ Older than 65 yrs of age D├╝┼¤├╝k BMI (< 20) Ailede kal├¦a k─▒r─▒─¤─▒ ├Čyk├╝s├╝ 50 ya┼¤─▒ndan sonra k─▒r─▒k ├Čyk├╝s├╝ olmas─▒ > 6 ay uzun k orti k osteroid kullan─▒m─▒ Sigara ( halen veya ge├¦mi┼¤te ) *Ōēź 5% drop in BMD should trigger bone-targeted therapy. Use lowest T-score from 3 sites. T-s koru < -2.0 Kemi─¤e Y├Čnelik Tedavi + K al s i y um ve vitamin D supplement asyonu KMD Her 2 y─▒lda bir de─¤erlendir
- 35. Cevaplanmam─▒┼¤ Sorular : Meme Kanserinde Kemik Hedefli Tedaviler Hangi ila├¦ ve uygulama ┼¤emas─▒? Oral vs IV bifosfonat, denosumab Doz, s─▒kl─▒k, s├╝re Baz─▒ ajanlar ile direkt anti-t├╝m├Čr etki? Veya kemoterap├Čtiklerle sinerji? Hangi hastalar/t├╝m├Čr adjuvan tedaviden fayda g├Čr├╝r? Pre vs postmenopozal? A┼¤─▒r─▒ kemik y─▒k─▒m─▒ olan hastalar? KT vs endokrin vs hedefe y├Čnelik? ER+, PTHrP+, RANK+, di─¤er mark─▒rlar? Tan─▒ an─▒nda kemik ili─¤i tutulumu?
Editor's Notes
- #17: 8
- #35: BMD, bone mineral density; BMI, body mass index; CTIBL, cancer treatmentŌĆōinduced bone loss. ╠² Hadji and colleagues have tried to help clinicians understand bone loss in women receiving AI therapy or the fracture risk in patients who are getting older. Bone mineral density is one indicator of risk of bone loss and subsequent fracture, but Hadji and colleagues lists several other factors that contribute to the risk of bone loss and fracture in a patient receiving an AI. Their guidelines state that if the patient has any 2 of the following risk factors, then bisphosphonate therapy should be instituted: a T score of < 1.5, which the case study patient had; older than age 65 of years; low body mass index (< 20); a family history of hip fracture (and because this case-study patient had a maternal relative that had a hip fracture this was a risk factor); personal history of fragility fracture after 50 years of age, which the case-study patient did not have; oral steroid use of more than 6 months, which the patient did not have; and smoking, which the patient did not have. Because this patient had 2 risk factors, bone-targeted therapy, such as a bisphosphonate, should be considered for this patient.