

































More Related Content
What's hot (20)
Viewers also liked (6)




Similar to ĐąĐ”ĐŒĐ°łć3łćĐ±Đ»ĐŸĐșłć7 (20)




















More from kafedra_trauma (20)




















ĐąĐ”ĐŒĐ°łć3łćĐ±Đ»ĐŸĐșłć7
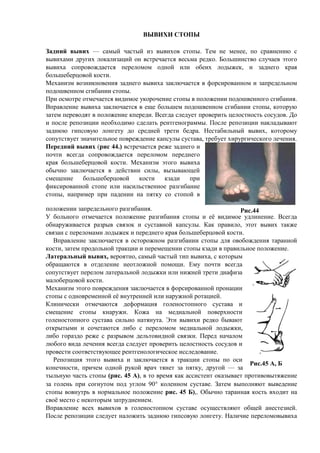
- 1. ĐĐ«ĐĐĐ„Đ ĐĄĐąĐĐĐ« ĐĐ°ĐŽĐœĐžĐč ĐČŃĐČĐžŃ â ŃĐ°ĐŒŃĐč ŃĐ°ŃŃŃĐč Оз ĐČŃĐČĐžŃ ĐŸĐČ ŃŃĐŸĐżŃ. ĐąĐ”ĐŒ ĐœĐ” ĐŒĐ”ĐœĐ”Đ”, ĐżĐŸ ŃŃĐ°ĐČĐœĐ”ĐœĐžŃ Ń ĐČŃĐČĐžŃ Đ°ĐŒĐž ĐŽŃŃĐłĐžŃ Đ»ĐŸĐșалОзаŃĐžĐč ĐŸĐœ ĐČŃŃŃĐ”ŃĐ°Đ”ŃŃŃ ĐČĐ”ŃŃĐŒĐ° ŃДЎĐșĐŸ. ĐĐŸĐ»ŃŃĐžĐœŃŃĐČĐŸ ŃĐ»ŃŃĐ°Đ”ĐČ ŃŃĐŸĐłĐŸ ĐČŃĐČĐžŃ Đ° ŃĐŸĐżŃĐŸĐČĐŸĐ¶ĐŽĐ°Đ”ŃŃŃ ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐŸĐŒ ĐŸĐŽĐœĐŸĐč ОлО ĐŸĐ±Đ”ĐžŃ Đ»ĐŸĐŽŃжДĐș, Đž Đ·Đ°ĐŽĐœĐ”ĐłĐŸ ĐșŃĐ°Ń Đ±ĐŸĐ»ŃŃДбДŃŃĐŸĐČĐŸĐč ĐșĐŸŃŃĐž. ĐĐ”Ń Đ°ĐœĐžĐ·ĐŒ ĐČĐŸĐ·ĐœĐžĐșĐœĐŸĐČĐ”ĐœĐžŃ Đ·Đ°ĐŽĐœĐ”ĐłĐŸ ĐČŃĐČĐžŃ Đ° Đ·Đ°ĐșĐ»ŃŃĐ°Đ”ŃŃŃ ĐČ ŃĐŸŃŃĐžŃĐŸĐČĐ°ĐœĐœĐŸĐŒ Đž Đ·Đ°ĐżŃДЎДлŃĐœĐŸĐŒ ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐŒ ŃĐłĐžĐ±Đ°ĐœĐžĐž ŃŃĐŸĐżŃ. ĐŃĐž ĐŸŃĐŒĐŸŃŃĐ” ĐŸŃĐŒĐ”ŃĐ°Đ”ŃŃŃ ĐČĐžĐŽĐžĐŒĐŸĐ” ŃĐșĐŸŃĐŸŃĐ”ĐœĐžĐ” ŃŃĐŸĐżŃ ĐČ ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐž ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐłĐŸ ŃĐłĐžĐ±Đ°ĐœĐžŃ. ĐĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐ” ĐČŃĐČĐžŃ Đ° Đ·Đ°ĐșĐ»ŃŃĐ°Đ”ŃŃŃ ĐČ Đ”ŃĐ” Đ±ĐŸĐ»ŃŃĐ”ĐŒ ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐŒ ŃĐłĐžĐ±Đ°ĐœĐžĐž ŃŃĐŸĐżŃ, ĐșĐŸŃĐŸŃŃŃ Đ·Đ°ŃĐ”ĐŒ пДŃĐ”ĐČĐŸĐŽŃŃ ĐČ ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐ” ĐșпДŃДЎО. ĐŃДгЎа ŃлДЎŃĐ”Ń ĐżŃĐŸĐČĐ”ŃĐžŃŃ ŃĐ”Đ»ĐŸŃŃĐœĐŸŃŃŃ ŃĐŸŃŃĐŽĐŸĐČ. ĐĐŸ Đž ĐżĐŸŃлД ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐœĐ”ĐŸĐ±Ń ĐŸĐŽĐžĐŒĐŸ ŃЎДлаŃŃ ŃĐ”ĐœŃĐłĐ”ĐœĐŸĐłŃĐ°ĐŒĐŒŃ. ĐĐŸŃлД ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐœĐ°ĐșлаЎŃĐČĐ°ŃŃ Đ·Đ°ĐŽĐœŃŃ ĐłĐžĐżŃĐŸĐČŃŃ Đ»ĐŸĐœĐłĐ”ŃŃ ĐŽĐŸ ŃŃĐ”ĐŽĐœĐ”Đč ŃŃĐ”ŃĐž бДЎŃĐ°. ĐĐ”ŃŃабОлŃĐœŃĐč ĐČŃĐČĐžŃ , ĐșĐŸŃĐŸŃĐŸĐŒŃ ŃĐŸĐżŃŃŃŃĐČŃĐ”Ń Đ·ĐœĐ°ŃĐžŃДлŃĐœĐŸĐ” ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžĐ” ĐșĐ°ĐżŃŃĐ»Ń ŃŃŃŃĐ°ĐČĐ°, ŃŃДбŃĐ”Ń Ń ĐžŃŃŃгОŃĐ”ŃĐșĐŸĐłĐŸ лДŃĐ”ĐœĐžŃ. ĐĐ”ŃĐ”ĐŽĐœĐžĐč ĐČŃĐČĐžŃ (ŃĐžŃ 44.) ĐČŃŃŃĐ”ŃĐ°Đ”ŃŃŃ ŃДжД Đ·Đ°ĐŽĐœĐ”ĐłĐŸ Đž ĐżĐŸŃŃĐž ĐČŃДгЎа ŃĐŸĐżŃĐŸĐČĐŸĐ¶ĐŽĐ°Đ”ŃŃŃ ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐŸĐŒ пДŃĐ”ĐŽĐœĐ”ĐłĐŸ ĐșŃĐ°Ń Đ±ĐŸĐ»ŃŃДбДŃŃĐŸĐČĐŸĐč ĐșĐŸŃŃĐž. ĐĐ”Ń Đ°ĐœĐžĐ·ĐŒ ŃŃĐŸĐłĐŸ ĐČŃĐČĐžŃ Đ° ĐŸĐ±ŃŃĐœĐŸ Đ·Đ°ĐșĐ»ŃŃĐ°Đ”ŃŃŃ ĐČ ĐŽĐ”ĐčŃŃĐČОО ŃОлŃ, ĐČŃĐ·ŃĐČĐ°ŃŃĐ”Đč ŃĐŒĐ”ŃĐ”ĐœĐžĐ” Đ±ĐŸĐ»ŃŃДбДŃŃĐŸĐČĐŸĐč ĐșĐŸŃŃĐž ĐșĐ·Đ°ĐŽĐž ĐżŃĐž ŃĐžĐșŃĐžŃĐŸĐČĐ°ĐœĐœĐŸĐč ŃŃĐŸĐżĐ” ОлО ĐœĐ°ŃОлŃŃŃĐČĐ”ĐœĐœĐŸĐ” ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžĐ” ŃŃĐŸĐżŃ, ĐœĐ°ĐżŃĐžĐŒĐ”Ń ĐżŃĐž ĐżĐ°ĐŽĐ”ĐœĐžĐž ĐœĐ° ĐżŃŃĐșŃ ŃĐŸ ŃŃĐŸĐżĐŸĐč ĐČ ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐž Đ·Đ°ĐżŃДЎДлŃĐœĐŸĐłĐŸ ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžŃ. ĐŁ Đ±ĐŸĐ»ŃĐœĐŸĐłĐŸ ĐŸŃĐŒĐ”ŃĐ°Đ”ŃŃŃ ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐ” ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžŃ ŃŃĐŸĐżŃ Đž Đ”Ń ĐČĐžĐŽĐžĐŒĐŸĐ” ŃĐŽĐ»ĐžĐœĐ”ĐœĐžĐ”. ĐŃДгЎа ĐŸĐ±ĐœĐ°ŃŃжОĐČĐ°Đ”ŃŃŃ ŃĐ°Đ·ŃŃĐČ ŃĐČŃĐ·ĐŸĐș Đž ŃŃŃŃĐ°ĐČĐœĐŸĐč ĐșĐ°ĐżŃŃĐ»Ń. ĐĐ°Đș ĐżŃĐ°ĐČĐžĐ»ĐŸ, ŃŃĐŸŃ ĐČŃĐČĐžŃ ŃĐ°ĐșжД ŃĐČŃĐ·Đ°Đœ Ń ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐ°ĐŒĐž Đ»ĐŸĐŽŃжДĐș Đž пДŃĐ”ĐŽĐœĐ”ĐłĐŸ ĐșŃĐ°Ń Đ±ĐŸĐ»ŃŃДбДŃŃĐŸĐČĐŸĐč ĐșĐŸŃŃĐž. ĐĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐ” Đ·Đ°ĐșĐ»ŃŃĐ°Đ”ŃŃŃ ĐČ ĐŸŃŃĐŸŃĐŸĐ¶ĐœĐŸĐŒ ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžĐž ŃŃĐŸĐżŃ ĐŽĐ»Ń ĐŸĐČĐŸĐ±ĐŸĐ¶ĐŽĐ”ĐœĐžŃ ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž, Đ·Đ°ŃĐ”ĐŒ ĐżŃĐŸĐŽĐŸĐ»ŃĐœĐŸĐč ŃŃĐ°ĐșŃОО Đž пДŃĐ”ĐŒĐ”ŃĐ”ĐœĐžĐž ŃŃĐŸĐżŃ ĐșĐ·Đ°ĐŽĐž ĐČ ĐżŃĐ°ĐČОлŃĐœĐŸĐ” ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐ”. ĐĐ°ŃĐ”ŃĐ°Đ»ŃĐœŃĐč ĐČŃĐČĐžŃ , ĐČĐ”ŃĐŸŃŃĐœĐŸ, ŃĐ°ĐŒŃĐč ŃĐ°ŃŃŃĐč ŃОп ĐČŃĐČĐžŃ Đ°, Ń ĐșĐŸŃĐŸŃŃĐŒ ĐŸĐ±ŃĐ°ŃĐ°ŃŃŃŃ ĐČ ĐŸŃĐŽĐ”Đ»Đ”ĐœĐžĐ” ĐœĐ”ĐŸŃĐ»ĐŸĐ¶ĐœĐŸĐč ĐżĐŸĐŒĐŸŃĐž. ĐĐŒŃ ĐżĐŸŃŃĐž ĐČŃДгЎа ŃĐŸĐżŃŃŃŃĐČŃĐ”Ń ĐżĐ”ŃĐ”Đ»ĐŸĐŒ лаŃĐ”ŃĐ°Đ»ŃĐœĐŸĐč Đ»ĐŸĐŽŃжĐșĐž ОлО ĐœĐžĐ¶ĐœĐ”Đč ŃŃĐ”ŃĐž ЎОаŃОза ĐŒĐ°Đ»ĐŸĐ±Đ”ŃŃĐŸĐČĐŸĐč ĐșĐŸŃŃĐž. ĐĐ”Ń Đ°ĐœĐžĐ·ĐŒ ŃŃĐŸĐłĐŸ ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ Đ·Đ°ĐșĐ»ŃŃĐ°Đ”ŃŃŃ ĐČ ŃĐŸŃŃĐžŃĐŸĐČĐ°ĐœĐœĐŸĐč ĐżŃĐŸĐœĐ°ŃОО ŃŃĐŸĐżŃ Ń ĐŸĐŽĐœĐŸĐČŃĐ”ĐŒĐ”ĐœĐœĐŸĐč Đ”Ń ĐČĐœŃŃŃĐ”ĐœĐœĐ”Đč ОлО ĐœĐ°ŃŃĐ¶ĐœĐŸĐč ŃĐŸŃĐ°ŃОДĐč. ĐĐ»ĐžĐœĐžŃĐ”ŃĐșĐž ĐŸŃĐŒĐ”ŃĐ°ŃŃŃŃ ĐŽĐ”ŃĐŸŃĐŒĐ°ŃĐžŃ ĐłĐŸĐ»Đ”ĐœĐŸŃŃĐŸĐżĐœĐŸĐłĐŸ ŃŃŃŃĐ°ĐČĐ° Đž ŃĐŒĐ”ŃĐ”ĐœĐžĐ” ŃŃĐŸĐżŃ ĐșĐœĐ°ŃŃжО. ĐĐŸĐ¶Đ° ĐœĐ° ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸĐč ĐżĐŸĐČĐ”ŃŃ ĐœĐŸŃŃĐž ĐłĐŸĐ»Đ”ĐœĐŸŃŃĐŸĐżĐœĐŸĐłĐŸ ŃŃŃŃĐ°ĐČĐ° ŃОлŃĐœĐŸ ĐœĐ°ŃŃĐœŃŃĐ°. ĐŃĐž ĐČŃĐČĐžŃ Đž ŃДЎĐșĐŸ бŃĐČĐ°ŃŃ ĐŸŃĐșŃŃŃŃĐŒĐž Đž ŃĐŸŃĐ”ŃĐ°ŃŃŃŃ Đ»ĐžĐ±ĐŸ Ń ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐŸĐŒ ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸĐč Đ»ĐŸĐŽŃжĐșĐž, Đ»ĐžĐ±ĐŸ ĐłĐŸŃĐ°Đ·ĐŽĐŸ ŃДжД Ń ŃĐ°Đ·ŃŃĐČĐŸĐŒ ЎДлŃŃĐŸĐČĐžĐŽĐœĐŸĐč ŃĐČŃĐ·ĐșĐž. ĐĐ”ŃДЎ ĐœĐ°ŃĐ°Đ»ĐŸĐŒ Đ»ŃĐ±ĐŸĐłĐŸ ĐČОЎа лДŃĐ”ĐœĐžŃ ĐČŃДгЎа ŃлДЎŃĐ”Ń ĐżŃĐŸĐČĐ”ŃĐžŃŃ ŃĐ”Đ»ĐŸŃŃĐœĐŸŃŃŃ ŃĐŸŃŃĐŽĐŸĐČ Đž ĐżŃĐŸĐČĐ”ŃŃĐž ŃĐŸĐŸŃĐČĐ”ŃŃŃĐČŃŃŃДД ŃĐ”ĐœŃĐłĐ”ĐœĐŸĐ»ĐŸĐłĐžŃĐ”ŃĐșĐŸĐ” ĐžŃŃĐ»Đ”ĐŽĐŸĐČĐ°ĐœĐžĐ”. Đ Đ”ĐżĐŸĐ·ĐžŃĐžŃ ŃŃĐŸĐłĐŸ ĐČŃĐČĐžŃ Đ° Đž Đ·Đ°ĐșĐ»ŃŃĐ°Đ”ŃŃŃ ĐČ ŃŃĐ°ĐșŃОО ŃŃĐŸĐżŃ ĐżĐŸ ĐŸŃĐž ĐșĐŸĐœĐ”ŃĐœĐŸŃŃĐž, ĐżŃĐžŃĐ”ĐŒ ĐŸĐŽĐœĐŸĐč ŃŃĐșĐŸĐč ĐČŃĐ°Ń ŃŃĐœĐ”Ń Đ·Đ° ĐżŃŃĐșŃ, ĐŽŃŃĐłĐŸĐč â Đ·Đ° ŃŃĐ»ŃĐœŃŃ ŃĐ°ŃŃŃ ŃŃĐŸĐżŃ (ŃĐžŃ. 45 Đ), ĐČ ŃĐŸ ĐČŃĐ”ĐŒŃ ĐșĐ°Đș Đ°ŃŃĐžŃŃĐ”ĐœŃ ĐŸĐșĐ°Đ·ŃĐČĐ°Đ”Ń ĐżŃĐŸŃĐžĐČĐŸĐČŃŃŃĐ¶Đ”ĐœĐžĐ” Đ·Đ° ĐłĐŸĐ»Đ”ĐœŃ ĐżŃĐž ŃĐŸĐłĐœŃŃĐŸĐŒ ĐżĐŸĐŽ ŃĐłĐ»ĐŸĐŒ 90ï° ĐșĐŸĐ»Đ”ĐœĐœĐŸĐŒ ŃŃŃŃĐ°ĐČĐ”. ĐĐ°ŃĐ”ĐŒ ĐČŃĐżĐŸĐ»ĐœŃŃŃ ĐČŃĐČĐ”ĐŽĐ”ĐœĐžĐ” ŃŃĐŸĐżŃ ĐČĐŸĐČĐœŃŃŃŃ ĐČ ĐœĐŸŃĐŒĐ°Đ»ŃĐœĐŸĐ” ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐ” ŃĐžŃ. 45 Đ),. ĐбŃŃĐœĐŸ ŃĐ°ŃĐ°ĐœĐœĐ°Ń ĐșĐŸŃŃŃ ĐČŃ ĐŸĐŽĐžŃ ĐœĐ° ŃĐČĐŸŃ ĐŒĐ”ŃŃĐŸ Ń ĐœĐ”ĐșĐŸŃĐŸŃŃĐŒ Đ·Đ°ŃŃŃĐŽĐœĐ”ĐœĐžĐ”ĐŒ. ĐĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐ” ĐČŃĐ”Ń ĐČŃĐČĐžŃ ĐŸĐČ ĐČ ĐłĐŸĐ»Đ”ĐœĐŸŃŃĐŸĐżĐœĐŸĐŒ ŃŃŃŃĐ°ĐČĐ” ĐŸŃŃŃĐ”ŃŃĐČĐ»ŃŃŃ ĐŸĐ±ŃĐ”Đč Đ°ĐœĐ”ŃŃДзОДĐč. ĐĐŸŃлД ŃĐ”ĐżĐŸĐ·ĐžŃОО ŃлДЎŃĐ”Ń ĐœĐ°Đ»ĐŸĐ¶ĐžŃŃ Đ·Đ°ĐŽĐœŃŃ ĐłĐžĐżŃĐŸĐČŃŃ Đ»ĐŸĐœĐłĐ”ŃŃ. ĐалОŃОД пДŃĐ”Đ»ĐŸĐŒĐŸĐČŃĐČĐžŃ Đ° Đ ĐžŃ.44 Đ ĐžŃ.45 Đ, Đ
- 2. ĐČ Đ±ĐŸĐ»ŃŃĐžĐœŃŃĐČĐ” ŃĐ»ŃŃĐ°Đ”ĐČ ĐŸĐżŃДЎДлŃĐ”Ń ĐżĐŸĐșĐ°Đ·Đ°ĐœĐžŃ Đș ĐŸĐżĐ”ŃĐ°ŃĐžĐČĐœĐŸĐŒŃ Đ»Đ”ŃĐ”ĐœĐžŃ ĐŒĐ”ŃĐŸĐŽĐ°ĐŒĐž ĐČĐœĐ”ĐŸŃĐ°ĐłĐŸĐČĐŸĐłĐŸ ĐŸŃŃĐ”ĐŸŃĐžĐœŃДза ОлО ĐČĐœŃŃŃĐ”ĐœĐœĐ”Đč ŃĐžĐșŃĐ°ŃОО. ĐĐ«ĐĐĐ„Đ ĐąĐĐ ĐĐĐĐĐ ĐĐХйРĐŃĐČĐžŃ Đž ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ĐŒĐŸĐ¶ĐœĐŸ ĐșлаŃŃĐžŃĐžŃĐžŃĐŸĐČĐ°ŃŃ ĐżĐŸ ĐŽĐČŃĐŒ ŃĐžĐżĐ°ĐŒ: ĐżĐŸĐ»ĐœŃĐč ĐČŃĐČĐžŃ ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž Đž пДŃĐžŃĐ°ŃĐ°ĐœĐœŃĐč (ĐżĐŸĐŽŃĐ°ŃĐ°ĐœĐœŃĐč) ĐČŃĐČĐžŃ (ŃĐžŃ.46). ĐŃĐž ĐżĐŸĐ»ĐœĐŸĐŒ ĐČŃĐČĐžŃ Đ” ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ĐżĐŸŃĐ»Đ”ĐŽĐœŃŃ ĐżĐŸĐ»ĐœĐŸŃŃŃŃ ĐČŃĐČĐžŃ ĐœŃŃĐ° Оз ĐČОлĐșĐž ĐłĐŸĐ»Đ”ĐœĐŸŃŃĐŸĐżĐœĐŸĐłĐŸ ŃŃŃŃĐ°ĐČĐ° Đž ŃĐŸŃĐžŃĐŸĐČĐ°ĐœĐ° ŃĐ°Đș, ŃŃĐŸ ĐœĐžĐ¶ĐœŃŃ ŃŃŃŃĐ°ĐČĐœĐ°Ń ĐżĐŸĐČĐ”ŃŃ ĐœĐŸŃŃŃ ĐŸĐ±ŃĐ°ŃĐ”ĐœĐ° ĐœĐ°Đ·Đ°ĐŽ, Đ° ĐłĐŸĐ»ĐŸĐČĐșĐ° ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž â ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸ. йДŃĐŒĐžĐœ пДŃĐžŃĐ°ŃĐ°ĐœĐœŃĐč ĐČŃĐČĐžŃ , ĐŸĐ·ĐœĐ°ŃĐ°Đ”Ń ĐČŃĐČĐžŃ ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž Оз ĐŸĐșŃŃжаŃŃĐžŃ Đ”Đ” ŃŃŃŃĐ°ĐČĐŸĐČ (ŃĐ°ŃĐ°ĐœĐœĐŸ- лаЎŃĐ”ĐČĐžĐŽĐœŃĐč Đž ŃĐ°ŃĐ°ĐœĐœĐŸ-ĐżŃŃĐŸŃĐœŃĐč ОлО ĐżĐŸĐŽŃĐ°ŃĐ°ĐœĐœŃĐč ŃŃŃŃĐ°ĐČŃ). ĐĐ”ŃĐžŃĐ°ŃĐ°ĐœĐœŃĐ” ĐČŃĐČĐžŃ Đž ĐŒĐŸĐ¶ĐœĐŸ ŃазЎДлОŃŃ ĐœĐ° ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœŃĐ” Đž лаŃĐ”ŃĐ°Đ»ŃĐœŃĐ” ĐČ Đ·Đ°ĐČĐžŃĐžĐŒĐŸŃŃĐž ĐŸŃ ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžŃ ŃŃĐŸĐżŃ ĐżĐŸ ĐŸŃĐœĐŸŃĐ”ĐœĐžŃ Đș ĐŽĐžŃŃĐ°Đ»ŃĐœĐŸĐŒŃ ĐŸŃĐŽĐ”Đ»Ń Đ±ĐŸĐ»ŃŃДбДŃŃĐŸĐČĐŸĐč ĐșĐŸŃŃĐž. ĐŃĐž Đ±ĐŸĐ»Đ”Đ” ŃĐ°ŃĐżŃĐŸŃŃŃĐ°ĐœĐ”ĐœĐœĐŸĐŒ ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸĐŒ ŃОпД ĐłĐŸĐ»ĐŸĐČĐșĐ° ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž палŃпОŃŃĐ”ŃŃŃ ŃĐœĐ°ŃŃжО. ĐĐ°ŃĐ”ŃĐ°Đ»ŃĐœŃĐč пДŃĐžŃĐ°ŃĐ°ĐœĐœŃĐč ĐČŃĐČĐžŃ ĐČŃŃŃĐ”ŃĐ°Đ”ŃŃŃ ŃДжД; ĐżŃĐž ĐœĐ”ĐŒ ĐłĐŸĐ»ĐŸĐČĐșĐ° ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ĐœĐ°ĐżŃĐ°ĐČĐ»Đ”ĐœĐ° ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸ Đž ĐŸĐ±ŃŃĐœĐŸ ĐŽĐŸŃŃŃĐżĐœĐ° палŃпаŃОО. ĐĐ”Ń Đ°ĐœĐžĐ·ĐŒ ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ. ĐĐ”ŃĐžŃĐ°ŃĐ°ĐœĐœŃĐ” ĐČŃĐČĐžŃ Đž ĐŸĐ±ŃŃĐœĐŸ ĐČĐŸĐ·ĐœĐžĐșĐ°ŃŃ ĐżŃĐž ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžĐž, ŃĐŸĐżŃĐŸĐČĐŸĐ¶ĐŽĐ°ŃŃĐ”ĐŒŃŃ ĐČĐœŃŃŃĐ”ĐœĐœĐ”Đč ŃĐŸŃĐ°ŃОДĐč Đž ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœŃĐŒ ŃĐłĐžĐ±Đ°ĐœĐžĐ”ĐŒ ŃŃĐŸĐżŃ. ĐĐŸŃĐșĐŸĐ»ŃĐșŃ ĐșĐŸŃŃĐž ŃŃĐŸĐżŃ ŃĐŒĐ”ŃĐ°ŃŃŃŃ ĐČ ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸĐŒ ĐœĐ°ĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐž, ĐżŃĐŸĐžŃŃ ĐŸĐŽĐžŃ ŃĐ°Đ·ŃŃĐČ ŃĐ°ŃĐ°ĐœĐœĐŸ-ĐżŃŃĐŸŃĐœĐŸĐč Đž ŃĐ°ŃĐ°ĐœĐœĐŸ-лаЎŃĐ”ĐČĐžĐŽĐœĐŸĐč ŃĐČŃĐ·ĐŸĐș. ĐŃĐž ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ ĐŒĐŸĐłŃŃ ĐČĐŸĐ·ĐœĐžĐșĐ°ŃŃ Ń ĐžĐłŃĐŸĐșĐŸĐČ ĐČ Đ±Đ°ŃĐșĐ”ŃĐ±ĐŸĐ», ĐșĐŸŃĐŸŃŃĐ” ĐżŃĐžĐ·Đ”ĐŒĐ»ŃŃŃŃŃ ĐœĐ° ŃŃĐŸĐżŃ ĐČ ŃĐŸŃŃĐŸŃĐœĐžĐž Đ”Ń ĐżŃĐžĐČĐ”ĐŽĐ”ĐœĐžŃ Đž ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐłĐŸ ŃĐłĐžĐ±Đ°ĐœĐžŃ. ĐĐ°ĐżŃДЎДлŃĐœĐŸĐ” ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐ” ŃĐłĐžĐ±Đ°ĐœĐžĐ” Đž ĐžĐœĐČĐ”ŃŃĐžŃ ŃŃĐŸĐżŃ ĐżŃĐžĐČĐŸĐŽŃŃ Đș ŃĐ°Đ·ŃŃĐČŃ ĐżĐ”ŃĐ”ĐŽĐœĐ”Đč, ĐČĐœŃŃŃĐ”ĐœĐœĐ”Đč Đž ĐœĐ°ŃŃĐ¶ĐœĐŸĐč ŃĐČŃĐ·ĐŸĐș Ń ĐŸŃĐŽĐ”Đ»Đ”ĐœĐžĐ”ĐŒ ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž. йаŃĐ°ĐœĐœĐ°Ń ĐșĐŸŃŃŃ ĐŸŃŃĐ°Đ”ŃŃŃ ĐČ ĐżĐ”ŃĐ”ĐŽĐœĐ”Đ±ĐŸĐșĐŸĐČĐŸĐŒ ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐž, ĐČ ŃĐŸ ĐČŃĐ”ĐŒŃ ĐșĐ°Đș ĐŸŃŃĐ°Đ»ŃĐœŃĐ” ĐșĐŸŃŃĐž ŃŃĐŸĐżŃ ŃĐŒĐ”ŃĐ°Đ”ŃŃŃ ĐČ ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœŃŃ ŃŃĐŸŃĐŸĐœŃ. ĐбŃĐ»Đ”ĐŽĐŸĐČĐ°ĐœĐžĐ”. Đ Đ°ĐœĐ°ĐŒĐœĐ”Đ·Đ” Đ±ĐŸĐ»ŃĐœĐŸĐłĐŸ ĐżŃĐžŃŃŃŃŃĐČŃĐ”Ń ŃŃĐ¶Đ”Đ»Đ°Ń ŃŃĐ°ĐČĐŒĐ° Ń ĐżĐŸŃĐČĐ»Đ”ĐœĐžĐ”ĐŒ ĐČŃŃĐ°Đ¶Đ”ĐœĐœĐŸĐč Đ±ĐŸĐ»Đž, ĐżŃОпŃŃ Đ»ĐŸŃŃĐž Đž Đ±ĐŸĐ»Đ”Đ·ĐœĐ”ĐœĐœĐŸŃŃĐž ĐżŃĐž палŃпаŃОО. ĐŃĐž ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸĐŒ ĐČŃĐČĐžŃ Đ” ŃŃĐŸĐżĐ° ŃĐŒĐ”ŃĐ”ĐœĐ° ĐČĐŸĐČĐœŃŃŃŃ, Đ° ŃĐ°ŃĐ°ĐœĐœĐ°Ń ĐșĐŸŃŃŃ ĐżĐ°Đ»ŃпОŃŃĐ”ŃŃŃ ŃĐœĐ°ŃŃжО. ĐŃĐŸĐČĐŸŃĐœĐ°Đ±Đ¶Đ”ĐœĐžĐ” ĐșĐŸĐ¶Đž ŃĐ°ŃŃĐŸ ĐœĐ°ŃŃŃĐ”ĐœĐŸ Оз-Đ·Đ° ĐŽĐ°ĐČĐ»Đ”ĐœĐžŃ ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž. Đ Đ”ĐœŃĐłĐ”ĐœĐŸĐłŃĐ°ŃĐžŃ. ĐĐ»Ń ĐČŃŃĐČĐ»Đ”ĐœĐžŃ ĐČŃĐČĐžŃ Đ° ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ĐŽĐŸŃŃĐ°ŃĐŸŃĐœĐŸ ŃĐ”ĐœŃĐłĐ”ĐœĐŸĐłŃĐ°ĐŒĐŒ ĐČ ĐŸĐ±ŃŃĐœŃŃ ĐżŃĐŸĐ”ĐșŃĐžŃŃ , ĐČĐșĐ»ŃŃĐ°Ń ĐżŃŃĐŒŃŃ, Đ±ĐŸĐșĐŸĐČŃŃ Đž ĐșĐŸŃŃŃ. ĐĐ»Ń ĐŽĐŸĐșŃĐŒĐ”ĐœŃĐžŃĐŸĐČĐ°ĐœĐžŃ Đž ĐžŃĐșĐ»ŃŃĐ”ĐœĐžŃ ĐžĐŒĐ”ŃŃĐžŃ ŃŃ ŃĐșŃŃŃŃŃ ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐŸĐČ ĐżĐŸŃлД ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐœĐ”ĐŸĐ±Ń ĐŸĐŽĐžĐŒŃ ĐșĐŸĐœŃŃĐŸĐ»ŃĐœŃĐ” ŃĐœĐžĐŒĐșĐž. ĐĄĐŸĐżŃŃŃŃĐČŃŃŃОД ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ. ĐĐŸĐ»ĐœŃĐč ŃĐ°ŃĐ°ĐœĐœŃĐč Đž пДŃĐžŃĐ°ŃĐ°ĐœĐœŃĐč ĐČŃĐČĐžŃ Đž ĐŒĐŸĐłŃŃ ŃĐŸŃĐ”ŃĐ°ŃŃŃŃ ŃĐŸ ŃлДЎŃŃŃĐžĐŒĐž ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃĐŒĐž: 1) пДŃĐ”Đ»ĐŸĐŒ ĐșĐŸŃŃĐ”Đč ĐżŃДЎплŃŃĐœŃ; 2) пДŃĐ”Đ»ĐŸĐŒ Đ»ĐŸĐŽŃжДĐș; 3) пДŃĐ”Đ»ĐŸĐŒ ŃĐ”ĐčĐșĐž ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž; 4) ŃĐ°Đ·ŃŃĐČ ŃĐČŃĐ·ĐŸĐș ĐłĐŸĐ»Đ”ĐœĐŸŃŃĐŸĐżĐœĐŸĐłĐŸ ŃŃŃŃĐ°ĐČĐ° Đž ĐżĐŸĐŽĐŽĐ”ŃжОĐČĐ°ŃŃĐžŃ ŃĐČŃĐ·ĐŸĐș ĐżŃДЎплŃŃĐœŃ. ĐĐ”ŃĐ”ĐœĐžĐ”. ĐĐ”ĐŸŃĐ»ĐŸĐ¶ĐœĐŸĐ” лДŃĐ”ĐœĐžĐ” Đ·Đ°ĐșŃŃŃŃŃ ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžĐč ĐČĐșĐ»ŃŃĐ°Đ”Ń ĐœĐ°Đ·ĐœĐ°ŃĐ”ĐœĐžĐ” Đ°ĐœĐ°Đ»ŃгДŃĐžĐșĐŸĐČ Đž ŃŃĐŸŃĐœŃŃ ŃĐ”ĐżĐŸĐ·ĐžŃĐžŃ ĐŽĐ»Ń ĐżŃĐ”ĐŽĐŸŃĐČŃĐ°ŃĐ”ĐœĐžŃ ĐœĐ”ĐșŃĐŸĐ·Đ° ĐșĐŸĐ¶Đž. ĐŃлО ŃŃĐŸŃĐœĐ°Ń ĐșĐŸĐœŃŃĐ»ŃŃĐ°ŃĐžŃ ĐŸŃŃĐŸĐżĐ”ĐŽĐ° ĐœĐ”ĐČĐŸĐ·ĐŒĐŸĐ¶ĐœĐ°, ŃлДЎŃĐ”Ń ĐżĐŸĐżŃŃĐ°ŃŃŃŃ ĐČŃĐżĐŸĐ»ĐœĐžŃŃ Đ·Đ°ĐșŃŃŃŃŃ ŃĐ”ĐżĐŸĐ·ĐžŃĐžŃ. ĐŃĐž ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸĐŒ ĐČŃĐČĐžŃ Đ” ŃĐœĐ°Ńала ŃлДЎŃĐ”Ń ĐżŃĐŸĐžĐ·ĐČĐ”ŃŃĐž ŃОлŃĐœŃŃ, ĐœĐŸ плаĐČĐœŃŃ ŃŃĐ°ĐșŃĐžŃ ĐČ ŃŃĐŸŃĐŸĐœŃ ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐłĐŸ ŃĐłĐžĐ±Đ°ĐœĐžŃ Đž ĐżŃĐžĐČĐ”ĐŽĐ”ĐœĐžĐ”, ŃĐ»Đ”ĐŽĐŸĐŒ Đ·Đ° ĐșĐŸŃĐŸŃŃĐŒĐž ĐœĐ° ĐłĐŸĐ»ĐŸĐČĐșŃ ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ĐŸĐșĐ°Đ·ŃĐČĐ°ŃŃ ĐŽĐ°ĐČĐ»Đ”ĐœĐžĐ”, ĐŸĐŽĐœĐŸĐČŃĐ”ĐŒĐ”ĐœĐœĐŸ ĐŸŃĐČĐŸĐŽŃ ĐżĐ”ŃĐ”ĐŽĐœĐžĐč ĐŸŃЎДл ŃŃĐŸĐżŃ. ĐŃĐž бДзŃŃпДŃĐœĐŸŃŃĐž ĐżĐŸĐșĐ°Đ·Đ°ĐœĐ° ĐŸŃĐșŃŃŃĐ°Ń ŃĐ”ĐżĐŸĐ·ĐžŃĐžŃ. ĐĐ°ŃĐ”ŃĐ°Đ»ŃĐœŃĐ” ĐČŃĐČĐžŃ Đž ĐŒĐŸĐ¶ĐœĐŸ ŃĐ”ĐżĐŸĐœĐžŃĐŸĐČĐ°ŃŃ ĐżŃŃĐ”ĐŒ Đ ĐžŃ.46
- 3. ĐżŃĐžĐ»ĐŸĐ¶Đ”ĐœĐžŃ ŃОлŃĐœĐŸĐč ŃŃĐ°ĐșŃОО Đ·Đ° ŃŃĐŸĐżŃ Ń ĐżĐŸŃлДЎŃŃŃĐžĐŒ ĐżŃĐžĐČĐ”ĐŽĐ”ĐœĐžĐ”ĐŒ ДД пДŃĐ”ĐŽĐœĐ”ĐłĐŸ ĐŸŃЎДла. ĐŃĐșŃŃŃŃĐ” ĐČŃĐČĐžŃ Đž ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ĐČĐżĐŸĐ»ĐœĐ” ĐŸĐ±ŃŃĐœŃ. ĐĐ” ŃлДЎŃĐ”Ń ĐżŃДЎпŃĐžĐœĐžĐŒĐ°ŃŃ ĐżĐŸĐżŃŃĐșŃ ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐŸŃĐșŃŃŃĐŸĐłĐŸ ĐČŃĐČĐžŃ Đ° ĐŽĐŸ ĐżĐŸŃŃŃĐżĐ»Đ”ĐœĐžŃ ĐČ ĐŸŃŃĐŸĐżĐ”ĐŽĐŸ-ŃŃĐ°ĐČĐŒĐ°ŃĐŸĐ»ĐŸĐłĐžŃĐ”ŃĐșĐŸĐ” ĐŸŃĐŽĐ”Đ»Đ”ĐœĐžĐ”. Đ ŃŃĐ»ĐŸĐČĐžŃŃ ŃпДŃОалОзОŃĐŸĐČĐ°ĐœĐœĐŸĐłĐŸ ĐŸŃĐŽĐ”Đ»Đ”ĐœĐžŃ ĐșĐŸĐ¶Ń ĐČĐŸĐșŃŃĐł ŃĐ°ĐœŃ Đ±ŃĐ”ŃŃ, ŃĐ°ĐœŃ ĐżŃĐŸĐŒŃĐČĐ°ŃŃ ŃŃĐ”ŃОлŃĐœŃĐŒ ŃĐžĐ·ĐžĐŸĐ»ĐŸĐłĐžŃĐ”ŃĐșĐžĐŒ ŃĐ°ŃŃĐČĐŸŃĐŸĐŒ. ĐĐ°Đș Đž ĐżŃĐž ĐČŃĐ”Ń ĐŸŃĐșŃŃŃŃŃ ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐ°Ń ĐžĐ»Đž ĐČŃĐČĐžŃ Đ°Ń ŃĐ”ĐżĐŸĐ·ĐžŃĐžŃ ĐŸŃŃŃĐ”ŃŃĐČĐ»ŃŃŃ ĐČ ŃŃĐ»ĐŸĐČĐžŃŃ ĐŸĐżĐ”ŃĐ°ŃĐžĐŸĐœĐœĐŸĐč. ĐĄŃĐ°Đ·Ń Đ¶Đ” ĐœĐ°Đ·ĐœĐ°ŃĐ°ŃŃ Đ°ĐœŃĐžĐ±ĐžĐŸŃĐžĐșĐž Đž ĐżĐŸ ĐżĐŸĐșĐ°Đ·Đ°ĐœĐžŃĐŒ ĐČĐČĐŸĐŽŃŃ ĐżŃĐŸŃĐžĐČĐŸŃŃĐŸĐ»Đ±ĐœŃŃĐœŃĐč Đ°ĐœĐ°ŃĐŸĐșŃĐžĐœ. ĐŃĐ»ĐŸĐ¶ĐœĐ”ĐœĐžŃ. ĐŃĐČĐžŃ Đž ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ĐŒĐŸĐłŃŃ ĐŸŃĐ»ĐŸĐ¶ĐœŃŃŃŃŃ ŃĐ°Đ·ĐČĐžŃĐžĐ”ĐŒ ĐœĐ”ŃĐșĐŸĐ»ŃĐșĐžŃ ŃĐ”ŃŃĐ”Đ·ĐœŃŃ ĐœĐ°ŃŃŃĐ”ĐœĐžĐč. 1. ĐĐČĐ°ŃĐșŃĐ»ŃŃĐœŃĐč ĐœĐ”ĐșŃĐŸĐ· ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž ŃĐ°ŃŃĐŸ ĐŸŃĐ»ĐŸĐ¶ĐœŃĐ”Ń ĐŽĐ»ĐžŃДлŃĐœĐŸĐ” лДŃĐ”ĐœĐžĐ” ŃŃĐžŃ ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžĐč. 2. ĐĐŸŃĐ”ŃŃ ĐŽĐČĐžĐ¶Đ”ĐœĐžĐč ĐČ ĐłĐŸĐ»Đ”ĐœĐŸŃŃĐŸĐżĐœĐŸĐŒ ŃŃŃŃĐ°ĐČĐ” Đž ŃŃĐ°ĐČĐŒĐ°ŃĐžŃĐ”ŃĐșĐžĐč Đ°ŃŃŃĐžŃ â ĐŸĐ±ŃŃĐœŃĐ” ŃĐČĐ»Đ”ĐœĐžŃ ĐżĐŸŃлД ĐČŃĐČĐžŃ ĐŸĐČ ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž. 3. ĐĐŸĐ·ĐŒĐŸĐ¶Đ”Đœ ĐžŃĐ”ĐŒĐžŃĐ”ŃĐșĐžĐč ĐœĐ”ĐșŃĐŸĐ· ĐșĐŸĐ¶Đž ĐČŃлДЎŃŃĐČОД ĐŽĐ°ĐČĐ»Đ”ĐœĐžŃ ĐżĐŸĐŽĐ»Đ”Đ¶Đ°ŃĐ”Đč ŃĐ°ŃĐ°ĐœĐœĐŸĐč ĐșĐŸŃŃĐž. ĐĐ«ĐĐĐ„Đ Đ ĐĐĐ ĐĐĐĐĐĐĐ«ĐĐĐ„Đ ĐĐĐĄĐąĐĐ ĐĐ ĐĐĐĐПХĐĐ« ĐŃДЎплŃŃĐœĐ° ŃĐČĐ»ŃĐ”ŃŃŃ ĐœĐ°ĐžĐŒĐ”ĐœĐ”Đ” ĐżĐŸĐŽĐČĐžĐ¶ĐœĐŸĐč ŃĐ°ŃŃŃŃ ŃŃĐŸĐżŃ Đž ĐČĐșĐ»ŃŃĐ°Đ”Ń Đ»Đ°ĐŽŃĐ”ĐČĐžĐŽĐœŃŃ, ĐșŃĐ±ĐŸĐČĐžĐŽĐœŃŃ Đž ŃŃĐž ĐșĐ»ĐžĐœĐŸĐČĐžĐŽĐœŃĐ” ĐșĐŸŃŃĐž. Đ ĐŸŃĐœĐŸĐČĐœĐŸĐŒ ŃОпОŃĐœŃĐ” ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ ŃĐŸŃŃĐ°ĐČĐ»ŃŃŃ ĐŒĐœĐŸĐ¶Đ”ŃŃĐČĐ”ĐœĐœŃĐ” пДŃĐ”Đ»ĐŸĐŒŃ ĐžĐ»Đž пДŃĐ”Đ»ĐŸĐŒĐŸĐČŃĐČĐžŃ Đž. ĐĐșŃĐžĐŸĐŒĐ°: ŃлДЎŃĐ”Ń ŃŃĐžŃĐ°ŃŃ, ŃŃĐŸ ĐŽĐžŃŃĐ°Đ»ŃĐœŃĐč пДŃĐ”Đ»ĐŸĐŒ ĐșŃĐ±ĐŸĐČĐžĐŽĐœĐŸĐč ОлО ĐșĐ»ĐžĐœĐŸĐČĐžĐŽĐœĐŸĐč ĐșĐŸŃŃĐ”Đč ĐČŃДгЎа ŃĐŸŃĐ”ŃĐ°Đ”ŃŃŃ Ń ĐČŃĐČĐžŃ ĐŸĐŒ ĐČ ĐżŃДЎплŃŃĐœĐ”-плŃŃĐœĐ”ĐČĐŸĐŒ ŃĐŸŃĐ»Đ”ĐœĐ”ĐœĐžĐž, ĐșĐŸŃĐŸŃŃĐč ĐŒĐŸĐł ŃĐżĐŸĐœŃĐ°ĐœĐœĐŸ ĐČĐżŃĐ°ĐČĐžŃŃŃŃ, Đ”ŃлО ĐœĐ” ĐŽĐŸĐșĐ°Đ·Đ°ĐœĐŸ ĐŸĐ±ŃĐ°ŃĐœĐŸĐ”. ĐĐ«ĐĐĐ„Đ Đ ĐĐĐ ĐĐĐĐĐĐĐ«ĐĐĐ„Đ Đ ĐĐ ĐĐĐĐПХĐĐ-ĐĐПХĐĐĐĐ«Đ„ ĐĄĐŁĐĄĐąĐĐĐĐ„ ĐĐ° ĐžŃĐșĐ»ŃŃĐ”ĐœĐžĐ”ĐŒ I-ĐŸĐč, ĐČŃĐ” плŃŃĐœĐ”ĐČŃĐ” ĐșĐŸŃŃĐž ŃĐŸĐ”ĐŽĐžĐœĐ”ĐœŃ ĐŒĐ”Đ¶ĐŽŃ ŃĐŸĐ±ĐŸĐč ĐżĐŸĐżĐ”ŃĐ”ŃĐœĐŸĐč ŃĐČŃĐ·ĐșĐŸĐč. ĐŃĐŸŃĐ°Ń ĐżĐ»ŃŃĐœĐ”ĐČĐ°Ń ĐșĐŸŃŃŃ ŃĐ°Đ·ĐŒĐ”ŃĐ°Đ”ŃŃŃ Đž ŃĐșŃĐ”ĐżĐ»Đ”ĐœĐ° ŃĐČŃĐ·ĐșĐ°ĐŒĐž ĐŒĐ”Đ¶ĐŽŃ ĐŒĐ”ĐŽĐžĐ°Đ»ŃĐœĐŸĐč Đž лаŃĐ”ŃĐ°Đ»ŃĐœĐŸĐč ĐșĐ»ĐžĐœĐŸĐČĐžĐŽĐœĐŸĐč ĐșĐŸŃŃŃĐŒĐž Đž ĐŽĐ”ĐčŃŃĐČŃĐ”Ń ĐșĐ°Đș пДŃĐČĐžŃĐœŃĐč ŃŃабОлОзаŃĐŸŃ ĐČŃĐ”ĐłĐŸ плŃŃĐœĐ”ĐČĐŸĐłĐŸ ĐșĐŸĐŒĐżĐ»Đ”ĐșŃĐ°. ĐŃĐČĐžŃ ĐČ ĐżŃДЎплŃŃĐœĐ”-плŃŃĐœĐ”ĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń , ĐșĐ°Đș ĐżŃĐ°ĐČĐžĐ»ĐŸ, ĐżŃĐžĐČĐŸĐŽĐžŃ Đș пДŃĐ”Đ»ĐŸĐŒŃ ĐŸŃĐœĐŸĐČĐ°ĐœĐžŃ II плŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž. ĐбŃŃĐœĐŸ ĐČŃĐČĐžŃ Đž ĐŒĐŸĐłŃŃ ĐžĐŒĐ”ŃŃ ĐČŃĐ” плŃŃĐœĐ”ĐČŃĐ” ĐșĐŸŃŃĐž. ĐĐșŃĐžĐŸĐŒĐ°: пДŃĐ”Đ»ĐŸĐŒ ĐŸŃĐœĐŸĐČĐ°ĐœĐžŃ II плŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž ŃĐČĐ»ŃĐ”ŃŃŃ Ń Đ°ŃĐ°ĐșŃĐ”ŃĐœŃĐŒ ĐżŃĐžĐ·ĐœĐ°ĐșĐŸĐŒ ĐžĐŒĐ”ŃŃĐ”ĐłĐŸŃŃ ĐœĐ°ŃŃŃĐ”ĐœĐžŃ ŃĐ”Đ»ĐŸŃŃĐœĐŸŃŃĐž ĐżŃДЎплŃŃĐœĐ”-плŃŃĐœĐ”ĐČŃŃ ŃŃŃŃĐ°ĐČĐŸĐČ. ĐлаŃŃĐžŃĐžĐșĐ°ŃĐžŃ. ĐŃĐČĐžŃ Đž Đž пДŃĐ”Đ»ĐŸĐŒĐŸĐČŃĐČĐžŃ Đž ĐČ ĐżŃДЎплŃŃĐœĐ”-плŃŃĐœĐ”ĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ĐżĐŸĐ»ŃŃОлО ĐœĐ°Đ·ĐČĐ°ĐœĐžĐ” ĐČŃĐČĐžŃ ĐŸĐČ ĐĐžŃŃŃĐ°ĐœĐșĐ°. ĐĄ ŃĐŸŃĐșĐž Đ·ŃĐ”ĐœĐžŃ ĐœĐ”ĐŸŃĐ»ĐŸĐ¶ĐœĐŸĐč ĐżĐŸĐŒĐŸŃĐž ŃŃĐž ĐČŃĐČĐžŃ Đž ĐŒĐŸĐ¶ĐœĐŸ ŃазЎДлОŃŃ ĐœĐ° ĐŽĐČĐ” ĐłŃŃппŃ: ĐŸĐŽĐœĐŸŃŃĐŸŃĐŸĐœĐœĐžĐ” Đž ŃĐ°ŃŃ ĐŸĐŽŃŃОДŃŃ (ĐŽĐžĐČĐ”ŃгОŃŃŃŃОД). ĐŃĐž ĐŸĐŽĐœĐŸŃŃĐŸŃĐŸĐœĐœĐžŃ ĐČŃĐČĐžŃ Đ°Ń ĐžĐŒĐ”Đ”ŃŃŃ ŃĐŒĐ”ŃĐ”ĐœĐžĐ” ŃĐ”ŃŃŃĐ”Ń ĐžĐ»Đž ĐČŃĐ”Ń ĐżŃŃĐž плŃŃĐœĐ”ĐČŃŃ ĐșĐŸŃŃĐ”Đč ĐČ ĐŸĐŽĐœĐŸĐŒ ĐœĐ°ĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐž (ŃĐžŃ. 47). ĐŃĐž ŃĐ°ŃŃ ĐŸĐŽŃŃĐžŃ ŃŃ ĐČŃĐČĐžŃ Đ°Ń ĐžĐŒĐ”Đ”ŃŃŃ ŃĐ°ŃŃĐ”Đ»ĐžĐœĐ°, ĐŸĐ±ŃŃĐœĐŸ ĐŒĐ”Đ¶ĐŽŃ I Đž II плŃŃĐœĐ”ĐČŃĐŒĐž ĐșĐŸŃŃŃĐŒĐž. ĐĐ”Ń Đ°ĐœĐžĐ·ĐŒ ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ. ĐĐŽĐœĐŸŃŃĐŸŃĐŸĐœĐœĐžĐč ĐČŃĐČĐžŃ ĐŒĐŸĐ¶Đ”Ń ĐČĐŸĐ·ĐœĐžĐșĐœŃŃŃ ĐżĐŸŃлД ĐżĐ°ĐŽĐ”ĐœĐžŃ ĐœĐ° ŃŃĐŸĐżŃ, ĐœĐ°Ń ĐŸĐŽŃŃŃŃŃŃ ĐČ ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐž ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐłĐŸ ŃĐłĐžĐ±Đ°ĐœĐžŃ (ŃĐžŃ.48). ĐĐŸĐŒĐżŃĐ”ŃŃĐžĐŸĐœĐœŃĐ” ŃĐžĐ»Ń (ŃĐžŃ.49) ĐżŃĐž Đ°ĐČŃĐŸĐŒĐŸĐ±ĐžĐ»ŃĐœŃŃ Đ°ĐČĐ°ŃĐžŃŃ ĐžĐ»Đž ŃДзĐșĐŸĐŒ ŃĐșŃŃŃĐžĐČĐ°ĐœĐžĐž ŃŃĐŸĐżŃ ŃĐ°ĐșжД ĐŒĐŸĐłŃŃ ĐżŃĐžĐČĐ”ŃŃĐž Đș ŃŃĐŸĐŒŃ ŃĐžĐżŃ ĐČŃĐČĐžŃ Đ°. Đ Đ°ŃŃ ĐŸĐŽŃŃОДŃŃ ĐČŃĐČĐžŃ Đž ĐŸĐ±ŃŃĐœĐŸ ĐœĐ°ŃŃŃпаŃŃ ĐżŃĐž ĐČĐŸĐ·ĐŽĐ”ĐčŃŃĐČОО ĐżŃŃĐŒĐŸĐč Đ ĐžŃ.48 Đ ĐžŃ. 47
- 4. ĐșĐŸĐŒĐżŃĐ”ŃŃĐžĐŸĐœĐœĐŸĐč ĐżĐŸĐČŃДжЎаŃŃĐ”Đč ŃОлŃ, ŃĐ°ŃŃДплŃŃŃĐ”Đč ĐŒĐ”Đ¶ĐżĐ»ŃŃĐœĐ”ĐČŃĐč ĐżŃĐŸĐŒĐ”Đ¶ŃŃĐŸĐș (ŃĐžŃ.49). Đ Đ°ŃŃ ĐŸĐŽŃŃĐžĐŒŃŃ ĐČŃĐČĐžŃ Đ°ĐŒ ŃĐ°ŃŃĐŸ ŃĐŸĐżŃŃŃŃĐČŃŃŃ ĐŸŃŃŃĐČĐœŃĐ” ĐșŃĐ°Đ”ĐČŃĐ” пДŃĐ”Đ»ĐŸĐŒŃ ĐČ ĐżŃДЎплŃŃĐœĐ”-плŃŃĐœĐ”ĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń . ĐбŃĐ»Đ”ĐŽĐŸĐČĐ°ĐœĐžĐ”. ĐбŃŃĐœĐŸ Đ±ĐŸĐ»ŃĐœĐŸĐč жалŃĐ”ŃŃŃ ĐœĐ° ŃОлŃĐœŃŃ Đ±ĐŸĐ»Ń ĐČ ŃŃĐ”ĐŽĐœĐ”ĐŒ ĐŸŃЎДлД ŃŃĐŸĐżŃ, ĐżŃОпŃŃ Đ»ĐŸŃŃŃ Đž ĐžĐœĐŸĐłĐŽĐ° паŃĐ”ŃŃДзОŃ. ĐŃĐž ĐŸŃĐŒĐŸŃŃĐ” ĐŒĐŸĐ¶Đ”Ń ĐČŃŃŃŃ- паŃŃ ĐŸŃĐœĐŸĐČĐ°ĐœĐžĐ” I плŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž ОлО ĐœĐ°Đ±Đ»ŃĐŽĐ°ŃŃŃŃ ŃĐșĐŸŃĐŸŃĐ”ĐœĐžĐ” пДŃĐ”ĐŽĐœĐ”ĐłĐŸ ĐŸŃЎДла ŃŃĐŸĐżŃ. ХлДЎŃĐ”Ń ŃŃĐ°ŃДлŃĐœĐŸ ĐžŃŃĐ»Đ”ĐŽĐŸĐČĐ°ŃŃ Đž ĐŽĐŸĐșŃĐŒĐ”ĐœŃĐžŃĐŸĐČĐ°ŃŃ ĐœĐ”ŃĐČĐœĐŸ-ŃĐŸŃŃĐŽĐžŃŃŃĐč ŃŃĐ°ŃŃŃ ŃŃĐŸĐżŃ. Đ Đ”ĐœŃĐłĐ”ĐœĐŸĐłŃĐ°ŃĐžŃ. ĐĐ°Đș ĐżŃĐ°ĐČĐžĐ»ĐŸ, ĐŽĐŸŃŃĐ°ŃĐŸŃĐœĐŸ ŃĐœĐžĐŒĐșĐŸĐČ ĐČ ĐżŃŃĐŒĐŸĐč, Đ±ĐŸĐșĐŸĐČĐŸĐč Đž ĐșĐŸŃĐŸĐč ĐżŃĐŸĐ”ĐșŃĐžŃŃ . ĐĐŸŃĐșĐŸĐ»ŃĐșŃ ŃŃĐž ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ ĐœĐ”ŃДЎĐșĐŸ ĐœĐŸŃŃŃ ŃĐșŃŃŃŃĐč Ń Đ°ŃĐ°ĐșŃĐ”Ń Đž ĐŽĐ»Ń ŃĐŸŃĐœĐŸĐč ĐŽĐžĐ°ĐłĐœĐŸŃŃĐžĐșĐž ĐŒĐŸĐłŃŃ ĐżĐŸŃŃĐ”Đ±ĐŸĐČĐ°ŃŃ ŃĐœĐžĐŒĐșĐŸĐČ ĐČ ŃŃĐ°ĐČĐœĐžŃДлŃĐœŃŃ ĐżŃĐŸĐ”ĐșŃĐžŃŃ . ĐĐșŃĐžĐŸĐŒĐ°: ĐČ ĐœĐŸŃĐŒĐ” ĐČĐœŃŃŃĐ”ĐœĐœĐžĐč ĐșŃĐ°Đč ŃŃĐ”ĐŽĐœĐ”Đč ĐșĐ»ĐžĐœĐŸĐČĐžĐŽĐœĐŸĐč ĐșĐŸŃŃĐž ĐœĐ°Ń ĐŸĐŽĐžŃŃŃ ĐœĐ° ĐŸĐŽĐœĐŸĐč Đ»ĐžĐœĐžĐž Ń ĐČĐœŃŃŃĐ”ĐœĐœĐžĐŒ ĐșŃĐ°Đ”ĐŒ II плŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž (ŃĐžŃ.50). ĐŃĐ±ĐŸĐ” ĐœĐ°ŃŃŃĐ”ĐœĐžĐ” ŃŃĐŸĐč Đ»ĐžĐœĐžĐž ŃĐșĐ°Đ·ŃĐČĐ°Đ”Ń ĐœĐ° ĐœĐ”ŃŃабОлŃĐœĐŸĐ” ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžĐ” (ĐČŃĐČĐžŃ ) ĐČ ŃŃŃŃĐ°ĐČĐ” ĐĐžŃŃŃĐ°ĐœĐșĐ°. ĐĐșŃĐžĐŸĐŒĐ°: ĐŸŃĐșĐŸĐ»ŃŃĐ°ŃŃĐčŃĐč ОлО ĐșĐŸĐŒĐżŃĐ”ŃŃĐžĐŸĐœĐœŃĐč пДŃĐ”Đ»ĐŸĐŒ ĐșŃĐ±ĐŸĐČĐžĐŽĐœĐŸĐč ĐșĐŸŃŃĐž ŃĐ°ŃŃĐŸ ŃĐŸŃĐ”ŃĐ°Đ”ŃŃŃ Ń ĐČŃĐČĐžŃ Đ°ĐŒĐž ĐČ ĐżŃДЎплŃŃĐœĐ”-плŃŃĐœĐ”ĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń . ĐĄĐŸĐżŃŃŃŃĐČŃŃŃОД ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ. ĐŃĐČĐžŃ Đž ĐČ ŃŃŃŃĐ°ĐČĐ” ĐĐžŃŃŃĐ°ĐœĐșĐ° ĐŒĐŸĐłŃŃ ŃĐŸŃĐ”ŃĐ°ŃŃŃŃ ŃĐŸ ŃлДЎŃŃŃĐžĐŒĐž ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃĐŒĐž: 1) пДŃĐ”Đ»ĐŸĐŒ ĐŸŃĐœĐŸĐČĐ°ĐœĐžŃ ĐČŃĐŸŃĐŸĐč плŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž; 2) ĐŸŃĐșĐŸĐ»ŃŃĐ°ŃŃĐ” пДŃĐ”Đ»ĐŸĐŒŃ ŃĐŒĐ”Đ¶ĐœŃŃ ĐżŃДЎплŃŃĐœĐ”ĐČŃŃ ĐžĐ»Đž плŃŃĐœĐ”ĐČŃŃ ĐșĐŸŃŃĐ”Đč; 3) ĐŸŃĐșĐŸĐ»ŃŃĐ°ŃŃĐč ОлО ĐșĐŸĐŒĐżŃĐ”ŃŃĐžĐŸĐœĐœŃĐč пДŃĐ”Đ»ĐŸĐŒ ĐșŃĐ±ĐŸĐČĐžĐŽĐœĐŸĐč ĐșĐŸŃŃĐž; 4) ĐžŃĐ”ĐŒĐžŃ ŃŃĐŸĐżŃ ĐČŃлДЎŃŃĐČОД ŃĐżĐ°Đ·ĐŒĐ° ОлО ŃŃĐŸĐŒĐ±ĐŸĐ·Đ° Đ°ŃŃĐ”ŃĐžĐč ŃŃĐŸĐżŃ; 5) пДŃĐ”Đ»ĐŸĐŒĐŸĐČŃĐČĐžŃ ĐșĐ»ĐžĐœĐŸĐČĐžĐŽĐœŃŃ ĐžĐ»Đž лаЎŃĐ”ĐČĐžĐŽĐœĐŸĐč ĐșĐŸŃŃĐ”Đč. ĐĐ”ŃĐ”ĐœĐžĐ”. ĐĐ”ĐŸŃĐ»ĐŸĐ¶ĐœĐ°Ń ĐżĐŸĐŒĐŸŃŃ ĐżŃĐž ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃŃ ŃŃŃŃĐ°ĐČĐ° ĐĐžŃŃŃĐ°ĐœĐșĐ°, ĐČĐșĐ»ŃŃĐ°Đ”Ń Đ°ĐœĐ°Đ»ŃгДŃĐžĐșĐž, лДЎ, ĐżŃĐžĐżĐŸĐŽĐœŃŃĐŸĐ” ĐżĐŸĐ»ĐŸĐ¶Đ”ĐœĐžĐ” ĐșĐŸĐœĐ”ŃĐœĐŸŃŃĐž Đž ŃŃĐŸŃĐœĐŸĐ” ĐœĐ°ĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐ” ĐŽĐ»Ń Đ·Đ°ĐșŃŃŃĐŸĐč ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐżĐŸĐŽ ĐŸĐ±ŃĐ”Đč Đ°ĐœĐ”ŃŃДзОДĐč. ĐąŃга Đ·Đ° палŃŃŃ ŃŃĐŸĐżŃ Ń ĐżŃĐŸŃĐžĐČĐŸŃŃĐłĐŸĐč Đ·Đ° Đ»ĐŸĐŽŃжĐșŃ ĐŸĐ±ŃŃĐœĐŸ ĐżŃĐžĐČĐŸĐŽĐžŃ Đș ŃĐ”ĐżĐŸĐ·ĐžŃОО. ĐŃлО Đ°ĐœĐ°ŃĐŸĐŒĐžŃĐ”ŃĐșĐž ŃĐŸŃĐœĐ°Ń ŃĐ”ĐżĐŸĐ·ĐžŃĐžŃ ĐœĐ” ĐŽĐŸŃŃĐžĐłĐœŃŃĐ°, ŃŃДбŃĐ”ŃŃŃ ĐŸŃĐșŃŃŃĐŸĐ” ĐČĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐ” Ń ĐČĐœŃŃŃĐ”ĐœĐœĐ”Đč ОлО ĐČĐœĐ”ŃĐœĐ”Đč ŃĐžĐșŃĐ°ŃОДĐč ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ, Đž ĐżĐŸŃлДЎŃŃŃĐ”Đč ĐžĐŒĐŒĐŸĐ±ĐžĐ»ĐžĐ·Đ°ŃОДĐč ĐČ ŃĐ”ŃĐ”ĐœĐžĐ” 6 ĐœĐ”ĐŽĐ”Đ»Ń Ń ĐŽĐ°Đ»ŃĐœĐ”ĐčŃĐžĐŒ ĐœĐŸŃĐ”ĐœĐžĐ”ĐŒ ŃŃĐżĐžĐœĐ°ŃĐŸŃĐ° ĐČ ŃĐ”ŃĐ”ĐœĐžĐ” ĐłĐŸĐŽĐ°. ĐŃĐ»ĐŸĐ¶ĐœĐ”ĐœĐžŃ. ĐŃĐČĐžŃ Đž ĐČ ĐżŃДЎплŃŃĐœĐ”-плŃŃĐœĐ”ĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ŃĐ°ŃŃĐŸ ĐŸŃĐ»ĐŸĐ¶ĐœŃŃŃŃŃ ŃĐ°Đ·ĐČĐžŃĐžĐ”ĐŒ ĐŽĐ”ĐłĐ”ĐœĐ”ŃĐ°ŃĐžĐČĐœĐŸĐłĐŸ Đ°ŃŃŃĐŸĐ·Đ° ОлО ĐœĐ°ŃŃŃĐ”ĐœĐžĐ”ĐŒ ĐșŃĐŸĐČĐŸĐŸĐ±ŃĐ°ŃĐ”ĐœĐžŃ ĐČ ĐŽĐžŃŃĐ°Đ»ŃĐœĐŸĐŒ ĐŸŃЎДлД ŃŃĐŸĐżŃ. ĐĐ«ĐĐĐ„Đ Đ ĐĐПХĐĐĐ€ĐĐĐĐĐĐĐĐ«Đ„ Đ ĐĐĐĐ€ĐĐĐĐĐĐĐĐ«Đ„ Đ ĐĄĐŁĐĄĐąĐĐĐĐ„ ĐŃĐČĐžŃ Đž ĐČ ĐżĐ»ŃŃĐœĐ”ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ Đž ĐŒĐ”Đ¶ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ĐČŃŃŃĐ”ŃĐ°ŃŃŃŃ ĐŽĐŸĐČĐŸĐ»ŃĐœĐŸ ŃĐ°ŃŃĐŸ Đž, ĐșĐ°Đș ĐżŃĐ°ĐČĐžĐ»ĐŸ, ĐżŃĐŸŃĐČĐ»ŃŃŃŃŃ ŃĐŒĐ”ŃĐ”ĐœĐžĐ”ĐŒ ŃĐ”ĐłĐŒĐ”ĐœŃĐ° ŃĐ°Đ»Đ°ĐœĐłĐž ĐșĐœĐžĐ·Ń. Đ ĐžŃ.49 Đ ĐžŃ.50
- 5. ĐĐ”Ń Đ°ĐœĐžĐ·ĐŒ ĐżĐŸĐČŃĐ”Đ¶ĐŽĐ”ĐœĐžŃ. ĐŃĐČĐžŃ Đž ĐČ ĐżĐ»ŃŃĐœĐ”ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ĐŸĐ±ŃŃĐ»ĐŸĐČĐ»Đ”ĐœŃ ĐŽĐ°ĐČĐ»Đ”ĐœĐžĐ”ĐŒ ĐČ ŃĐŸŃĐ”ŃĐ°ĐœĐžĐž Ń ĐżĐ”ŃĐ”ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžĐ”ĐŒ ĐżŃĐŸĐșŃĐžĐŒĐ°Đ»ŃĐœĐŸĐč ŃĐ°Đ»Đ°ĐœĐłĐž. ĐŃĐŸ ĐČŃĐ·ŃĐČĐ°Đ”Ń ŃĐ°Đ·ŃŃĐČ ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœĐŸĐč ŃĐ°ŃŃĐž ĐșĐ°ĐżŃŃĐ»Ń Đž ĐČŃĐČĐžŃ ĐżŃĐŸĐșŃĐžĐŒĐ°Đ»ŃĐœĐŸĐč ŃĐ°Đ»Đ°ĐœĐłĐž ĐČ ŃŃĐ»ŃĐœŃŃ ŃŃĐŸŃĐŸĐœŃ. ĐĐœŃŃŃĐ”ĐœĐœĐžĐ” ОлО ĐœĐ°ŃŃĐ¶ĐœŃĐ” ĐČŃĐČĐžŃ Đž ĐČ ĐżĐ»ŃŃĐœĐ”ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ŃĐČĐ»ŃŃŃŃŃ ŃДзŃĐ»ŃŃĐ°ŃĐŸĐŒ ĐČĐŸĐ·ĐŽĐ”ĐčŃŃĐČĐžŃ ĐżĐŸĐČŃДжЎаŃŃĐ”Đč ŃОлŃ, ŃĐ°Đ·ĐŽĐČОгаŃŃĐ”Đč ĐŒĐ”Đ¶ĐżĐ°Đ»ŃŃĐ”ĐČĐŸĐč ĐżŃĐŸĐŒĐ”Đ¶ŃŃĐŸĐș. ĐŃĐž ŃĐ»ĐŸĐ¶ĐœĐŸĐŒ ĐČŃĐČĐžŃ Đ” ĐČĐŸĐ»ŃŃĐœĐ°Ń ĐżĐ»Đ°ŃŃĐžĐœĐșĐ° Đ±ĐŸĐ»ŃŃĐŸĐłĐŸ палŃŃĐ° ĐČĐŒĐ”ŃŃĐ” Ń ŃĐ”ŃĐ°ĐŒĐŸĐČĐžĐŽĐœĐŸĐč ĐșĐŸŃŃŃŃ ŃĐŽĐ”ŃжОĐČĐ°Đ”Ń ŃĐ°Đ»Đ°ĐœĐłŃ ĐœĐ° ĐŽĐŸŃŃĐ°Đ»ŃĐœĐŸĐč ĐżĐŸĐČĐ”ŃŃ ĐœĐŸŃŃĐž плŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž (ŃĐžŃ. 51). ĐбŃĐ»Đ”ĐŽĐŸĐČĐ°ĐœĐžĐ”. ĐŃĐž ĐČŃĐČĐžŃ Đ°Ń ĐČ ĐżĐ»ŃŃĐœĐ”ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ĐŸŃĐŒĐ”ŃĐ°ŃŃŃŃ Đ±ĐŸĐ»Ń, Đ·Đ°ĐŒĐ”ŃĐœĐ°Ń ĐŽĐ”ŃĐŸŃĐŒĐ°ŃĐžŃ Đž ĐżŃОпŃŃ Đ»ĐŸŃŃŃ ŃŃŃŃĐ°ĐČĐ°, ĐœĐ”ĐČĐŸĐ·ĐŒĐŸĐ¶ĐœĐŸŃŃŃ Ń ĐŸĐŽĐžŃŃ. ĐĐ°Đș ĐżŃĐ°ĐČĐžĐ»ĐŸ, ĐœĐ°Đ±Đ»ŃĐŽĐ°Đ”ŃŃŃ ĐżĐ”ŃĐ”ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžĐ” палŃŃĐ°, ĐșĐŸŃĐŸŃŃĐč ŃĐŽĐČĐžĐœŃŃ ĐœĐ° ŃŃĐ»ŃĐœŃŃ ĐżĐŸĐČĐ”ŃŃ ĐœĐŸŃŃŃ ĐżĐ»ŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž. ĐŃĐž ŃĐ»ĐŸĐ¶ĐœŃŃ ĐČŃĐČĐžŃ Đ°Ń ĐŒĐŸĐ¶ĐœĐŸ палŃпОŃĐŸĐČĐ°ŃŃ ŃĐ”ŃĐ°ĐŒĐŸĐČĐžĐŽĐœŃŃ ĐșĐŸŃŃŃ ĐŽĐŸŃŃĐ°Đ»ŃĐœĐ”Đ” плŃŃĐœĐ”ĐČĐŸĐč. ĐĐŸĐ·ĐŒĐŸĐ¶ĐœĐŸ ŃĐŸŃĐ”ŃĐ°ĐœĐžĐ” ĐČŃĐČĐžŃ Đ° ĐČ ĐżĐ”ŃĐČĐŸĐŒ плŃŃĐœĐ”ŃĐ°Đ»Đ°ĐœĐłĐŸĐČĐŸĐŒ ŃŃŃŃĐ°ĐČĐ” Ń ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐ°ĐŒĐž ŃĐ”ŃĐ°ĐŒĐŸĐČĐžĐŽĐœŃŃ ĐșĐŸŃŃĐ”Đč. ĐĐșŃĐžĐČĐœĐŸĐ” ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžĐ” ĐŽĐžŃŃĐ°Đ»ŃĐœĐŸĐč ŃĐ°Đ»Đ°ĐœĐłĐž палŃŃĐ° ĐżŃĐžĐČĐŸĐŽĐžŃ Đș ŃŃĐžĐ»Đ”ĐœĐžŃ Đ±ĐŸĐ»Đž, ĐŸŃĐŽĐ°ŃŃĐ”ĐčŃŃ ĐœĐ° ĐżĐŸĐŽĐŸŃĐČĐ”ĐœĐœŃŃ ĐżĐŸĐČĐ”ŃŃ ĐœĐŸŃŃŃ ĐżĐ»ŃŃĐœĐ”ŃĐ°Đ»Đ°ĐœĐłĐŸĐČĐŸĐłĐŸ ŃŃŃŃĐ°ĐČĐ°. Đ Đ”ĐœŃĐłĐ”ĐœĐŸĐłŃĐ°ŃĐžŃ. ĐŃĐČĐžŃ Đž ĐČ ĐżĐ»ŃŃĐœĐ”ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ĐŽĐžĐ°ĐłĐœĐŸŃŃĐžŃŃŃŃ ĐœĐ° ŃĐœĐžĐŒĐșĐ°Ń ĐČ ĐżŃŃĐŒĐŸĐč ĐżŃĐŸĐ”ĐșŃОО, ĐżĐŸŃĐșĐŸĐ»ŃĐșŃ, ĐșĐ°Đș ĐżŃĐ°ĐČĐžĐ»ĐŸ, ĐŒĐ”Đ¶ĐŽŃ ĐŽĐžŃŃĐ°Đ»ŃĐœŃĐŒ ĐŸŃĐŽĐ”Đ»ĐŸĐŒ плŃŃĐœĐ”ĐČĐŸĐč ĐșĐŸŃŃĐž Đž ĐżŃĐŸĐșŃĐžĐŒĐ°Đ»ŃĐœĐŸĐč ŃĐ°Đ»Đ°ĐœĐłĐŸĐč ĐžĐŒĐ”Đ”ŃŃŃ ĐœĐ°ŃŃŃĐ”ĐœĐžĐ” ĐșĐŸĐœĐłŃŃŃĐœŃĐœĐŸŃŃĐž ŃŃŃŃĐ°ĐČĐœŃŃ ĐżĐŸĐČĐ”ŃŃ ĐœĐŸŃŃĐ”Đč. ĐŃĐČĐžŃ Đž ĐČ ĐŒĐ”Đ¶ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń Đ»ŃŃŃĐ” ĐČĐžĐŽĐœŃ ĐœĐ° ŃĐœĐžĐŒĐșĐ°Ń ĐČ ĐżŃŃĐŒĐŸĐč Đž ĐșĐŸŃĐŸĐč ĐżŃĐŸĐ”ĐșŃĐžŃŃ ; ŃĐ°ŃŃĐŸ ĐŸĐœĐž ŃĐŸŃĐ”ŃĐ°ŃŃŃŃ Ń ĐżĐ”ŃĐ”Đ»ĐŸĐŒĐ°ĐŒĐž ŃĐ°Đ»Đ°ĐœĐł палŃŃĐ”ĐČ ŃŃĐŸĐżŃ. ĐĐ”ŃĐ”ĐœĐžĐ”. ĐŃĐČĐžŃ ĐČ ĐżŃĐŸĐșŃĐžĐŒĐ°Đ»ŃĐœĐŸĐŒ ĐŒĐ”Đ¶ŃĐ°Đ»Đ°ĐœĐłĐŸĐČĐŸĐŒ ŃŃŃŃĐ°ĐČĐ” ĐŒĐŸĐ¶ĐœĐŸ лДŃĐžŃŃ ĐŒĐ”ŃĐŸĐŽĐŸĐŒ Đ·Đ°ĐșŃŃŃĐŸĐč ŃĐ”ĐżĐŸĐ·ĐžŃОО Ń ĐżĐŸŃлДЎŃŃŃĐžĐŒ ĐżŃĐžĐ±ĐžĐœŃĐŸĐČĐ°ĐœĐžĐ”ĐŒ ŃŃĐ°ĐČĐŒĐžŃĐŸĐČĐ°ĐœĐœĐŸĐłĐŸ палŃŃĐ° Đș ŃĐŸŃĐ”ĐŽĐœĐ”ĐŒŃ (ŃĐžŃ.52). ĐŃĐž ĐœĐ”ŃŃабОлŃĐœĐŸĐč ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐœĐ”ĐŸĐ±Ń ĐŸĐŽĐžĐŒĐŸ ŃŃĐŸŃĐœĐŸĐ” ĐœĐ°ĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐ” ĐŽĐ»Ń ĐČĐœŃŃŃĐ”ĐœĐœĐ”Đč ŃĐžĐșŃĐ°ŃОО. ĐŃĐČĐžŃ Đž ĐČ ĐżĐ»ŃŃĐœĐ”-ŃĐ°Đ»Đ°ĐœĐłĐŸĐČŃŃ ŃŃŃŃĐ°ĐČĐ°Ń ŃŃДбŃŃŃ ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐżĐŸĐŽ ĐŒĐ”ŃŃĐœĐŸĐč Đ°ĐœĐ”ŃŃДзОДĐč. ĐĐ»Ń ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐŽĐŸŃŃĐ°Đ»ŃĐœĐŸĐłĐŸ ĐČŃĐČĐžŃ Đ° ĐŸĐ±ŃŃĐœĐŸ ĐŽĐŸŃŃĐ°ŃĐŸŃĐœĐŸ пДŃĐ”ŃĐ°Đ·ĐłĐžĐ±Đ°ĐœĐžŃ ĐČ ĐČŃĐČĐžŃ ĐœŃŃĐŸĐŒ ŃŃŃŃĐ°ĐČĐ” ĐČ ŃĐŸŃĐ”ŃĐ°ĐœĐžĐž Ń ŃŃĐ°ĐșŃОДĐč ĐČ ĐŽĐžŃŃĐ°Đ»ŃĐœĐŸĐŒ ĐœĐ°ĐżŃĐ°ĐČĐ»Đ”ĐœĐžĐž. (ŃĐžŃ.53) ĐĄŃабОлŃĐœĐŸŃŃŃ ŃĐ”ĐżĐŸĐ·ĐžŃОО ĐŽĐŸŃŃОгаДŃŃŃ ĐżŃĐžĐŒĐ”ĐœĐ”ĐœĐžĐ”ĐŒ ĐŒĐ”ŃаллОŃĐ”ŃĐșĐŸĐč ŃĐžĐœŃ ŃŃĐŸĐșĐŸĐŒ ĐŽĐŸ 5 ĐœĐ”ĐŽĐ”Đ»Ń, Đ° ĐżŃĐž ĐœĐ”ŃŃабОлŃĐœĐŸĐč ŃĐ”ĐżĐŸĐ·ĐžŃОО ОлО бДзŃŃпДŃĐœĐŸĐč Đ”Ń ĐżĐŸĐżŃŃĐșĐ” ŃŃДбŃĐ”ŃŃŃ ĐŸŃĐșŃŃŃĐ°Ń ŃĐ”ĐżĐŸĐ·ĐžŃĐžŃ Đž ĐČĐœŃŃŃĐ”ĐœĐœŃŃ ŃĐžĐșŃĐ°ŃĐžŃ. Đ ĐžŃ. 51 Đ ĐžŃ.53 Đ ĐžŃ.52